


1Copenhagen Research Group for Inflammatory Skin (CORGIS), Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, and 2Section of Epidemiology, Department of Public Health, University of Copenhagen, Copenhagen, Denmark
Psoriasis is associated with cardiometabolic comorbidity; however, whether this is due to common lifestyle-related risk factors is unclear. This study investigated the association between psoriasis and cardiometabolic comorbidity, taking body mass index and smoking into account. The population comprised expectant mothers in the Danish National Birth Cohort (established 1996–2002). During pregnancy, the women were asked about physician-diagnosed psoriasis. Any association with self-reported cardiometabolic comorbidity 11 years later was assessed using logistic regression. The cohort was also followed up for hospital-diagnosed comorbidity, including cardiac death, until 31 December 2014, and the risk was assessed using Cox regression. A total of 2,435 women with psoriasis (2.90%) and 81,388 women without were identified. Psoriasis was significantly associated with self-reported hypercholesterolaemia (adjusted odds ratio 1.31; 1.01–1.70) and hospital-diagnosed hypertension (adjusted hazard ratio 1.33; 1.08–1.65). Women with psoriasis have an increased risk of developing cardiometabolic comorbidity in early adult life.
Key words: psoriasis; cardiovascular disease; metabolic disease; comorbidity; risk factor; cardiometabolic disease.
Accepted Nov 20, 2018; Epub ahead of print Nov 21, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Christoffer Blegvad, Copenhagen Research Group for Inflammatory Skin (CORGIS), Department of Dermatology and Allergy, Herlev and Gentofte Hospital, Kildegårdsvej 28, DK-2900 Hellerup, Denmark. E-mail: christoffer.blegvad.01@regionh.dk
Psoriasis is associated with cardiometabolic disorders; however, whether this is due to the common lifestyle-related risk factors overweight and smoking is unclear. This study investigated the relationship between psoriasis and cardiometabolic disorders taking these confounders into account. The study population consisted of women with and without psoriasis from a nationwide birth cohort in Denmark. Psoriasis was markedly associated with hypercholesterolaemia and hypertension. Women with psoriasis have an increased risk of developing cardiometabolic disorders in early adult life. Screening for classic risk factors might therefore be advisable.
Psoriasis is an inflammatory skin disease that affects 2–4% of the population in the Western world (1, 2). Psoriasis is known mainly from registry studies to be associated with a range of comorbidities, including cardiometabolic diseases (3, 4). The underlying mechanism is unknown, but has been proposed to be a systemic inflammatory state known as the “psoriatic march”, in which interplay between inflammatory mediators, such as cytokines and adipokines, ultimately lead to insulin resistance, atherosclerosis, and finally cardiovascular diseases, such as myocardial infarction and stroke (5). However, this comorbidity could be due to other factors, such as overweight and smoking. Data on these important confounding factors is seldom available in the registries. In this study involving a cohort of women in which there was self-reported data available, it was possible to control for these confounding factors. The purpose of the present study was to investigate the association between psoriasis and cardiometabolic comorbidity in women, taking the possibly confounding effects of body mass index (BMI) and smoking into account (Fig. S1).
The Danish National Birth Cohort (DNBC) was used to identify study participants. The DNBC is a nationwide cohort consisting of approximately 85,000 unique mothers who were interviewed about their health status halfway through pregnancy, between 1996 and 2002 (6). The mothers and their children have since been followed up using interviews and online questionnaires. DNBC data were used from the first telephone interview, carried out during the first half of pregnancy and the follow-up questionnaire to the mothers when the child was 11 years old. In Denmark, all inhabitants are assigned a unique 10-digit personal identification number in the Danish Civil Registration System (CRS), which allows linkage at the individual level with other national registries, including the DNBC (7). Data on age and vital status were available from the CRS. In addition to the DNBC and the CRS, the Danish National Patient Registry (DNPR) was used (8). The DNPR was established in 1978 and contains information on all hospital-based inpatient diagnoses, and since 1994, also outpatient diagnoses. Diagnosis codes are recorded according to the International Classification of Diseases, eighth revision (ICD-8) until 1994 and tenth revision (ICD-10) thereafter.
Baseline psoriasis status was obtained from the first interview during pregnancy, where the mothers were asked about the presence of physician-diagnosed psoriasis: “Have you ever had any skin disease?” → “Was the skin disease diagnosed by a doctor?” → “What kind of skin disease?” → “Psoriasis?”. In a sub-analysis, severe psoriasis was defined as a hospital (inpatient or outpatient) diagnosis of psoriasis (ICD-8 696.19 and ICD-10 L40.0, L40.4, L40.8, and L40.9) at the time of inclusion in the current study, i.e. the first pregnancy interview. This method of using ICD hospital diagnoses as the classifier for severe psoriasis has been validated previously (3).
The outcome of interest was cardiometabolic comorbidity. Self-reported information on lifetime experience of comorbidity was obtained from the 11-year questionnaire in the DNBC. The comorbidities were: hypertension, thrombosis (unspecified arterial or venous), type 2 diabetes (T2D), and hypercholesterolaemia. Furthermore, a composite outcome measure of metabolic syndrome was defined in accordance with the International Diabetes Federation guidelines: waist circumference ≥80 cm or BMI > 30 kg, plus 2 of the following: T2D, hypertension, or dyslipidaemia (9). Waist circumference and BMI were also obtained from the 11-year questionnaire in this case. For the hospital diagnoses, data from the DNPR were used. The ICD-10 diagnoses included were: hypertension (I10–I15), ischaemic heart disease (I20–I25, including cardiac death), T2D (E11), and hypercholesterolaemia (E78.0).
Information on the possible confounding factors pre-pregnancy BMI and smoking were obtained from the first pregnancy interview in the DNBC. The mother’s age at this time-point was also used for adjustment.
Baseline characteristics were expressed with means and standard deviations for continuous variables, and used frequencies and percentages in the case of categorical variables. Statistical testing for differences was performed using unpaired Student’s t-test and χ2 test, respectively. Two separate sub-studies were performed. Firstly, multiple logistic regression was used to estimate crude and adjusted odds ratios (ORs) for the association between baseline psoriasis and self-reported cardiometabolic comorbidity, as stated by subjects who responded to the 11-year questionnaire. Secondly, Cox regression was used to estimate crude and adjusted hazard ratios (HRs) to estimate the risk of incident hospital-diagnosed cardiometabolic comorbidity in all women with and without baseline psoriasis. Here, the women were followed up from the date of the first pregnancy interview to the date of cardiometabolic event, death, or 31 December 2014, whichever came first. Women with a history of event before the time of inclusion were excluded from the analysis. Calendar time was the underlying time variable. Both sub-studies were adjusted for age, pre-pregnancy BMI, and smoking status from the first pregnancy interview. To investigate the small individual effect of each confounding factor, sub-analyses adjustment was carried out for 1 confounder at a time. All results are reported with 95% confidence intervals (CIs) where possible. Analyses were performed using SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC, USA) and STATA software version 14.0 (StataCorp, College Station, TX, USA).
The study was performed in accordance with the “Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)” statement (10). Approval was granted as required from the Danish Data Protection Agency (reference Sund-2017-09), while ethical approval is not required for registry-based health studies in Denmark.
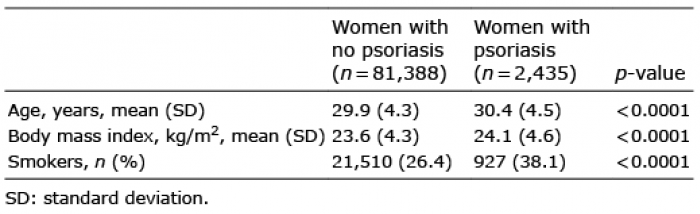
A total of 83,823 women who had participated in the first interview during pregnancy were identified, 2,435 (2.90%) of whom had reported having psoriasis (Table I and Fig. S2). At the time of inclusion, women with psoriasis were slightly older, on average, than women without psoriasis, they generally had a higher BMI, and a higher proportion smoked (38.1% vs. 26.4%). Of all the women, 125 (0.15%) had severe (hospital-diagnosed) psoriasis at the time of inclusion. The 11-year follow-up questionnaire was completed by 38,903 women (46.41%), 1,047 (2.69%) of whom had psoriasis and 52 (0.13%) of whom had severe psoriasis at inclusion.
Table I. Characteristics at the time of inclusion during pregnancy
In the first sub-study of baseline psoriasis and self-reported comorbidity from the 11-year follow-up questionnaire (Table II), it was found that hypercholesterolaemia was significantly associated with psoriasis even after adjusting for confounders (adjusted OR 1.31; 1.01–1.70). The other self-reported comorbidities of interest (hypertension, thrombosis, T2D, and metabolic syndrome) did not show any significant associations with psoriasis.
Table II. Association between baseline psoriasis and self-reported cardiometabolic comorbidity from the 11-year follow-up questionnaire
A sub-analysis of the hypercholesterolaemia results examined the (small) confounding effects of age, BMI, and smoking status separately, and they were found to be roughly equally important when looking at the respective adjusted ORs (data not shown).
When looking at severe (i.e. hospital-diagnosed) baseline psoriasis, a strong association with hypercholesterolaemia was found (adjusted OR 2.71; 1.41–6.41) (Table III). Interestingly, the composite outcome of metabolic syndrome showed a very strong association with severe psoriasis (adjusted OR 4.63; 1.38–15.47), even though no such association was found in the analysis of self-reported psoriasis. Again, no significant associations were found between severe psoriasis and the self-reported diagnoses of hypertension, thrombosis, or T2D.
Table III. Association between severe baseline psoriasis and self-reported cardiometabolic comorbidity from the 11-year follow-up questionnaire
In the second sub-study of baseline psoriasis and incident hospital-diagnosed comorbidity, an increased risk was found in the crude analyses of all diagnoses included: hypertension, ischaemic heart disease, T2D, and hypercholesterolaemia (Table IV). In the case of T2D, there was a highly significant interaction between psoriasis and BMI. We therefore stratified according to normal weight (BMI < 25 kg) or overweight (BMI ≥ 25 kg) in all analyses of T2D, and the increased risk of T2D was then evident only in the overweight women with psoriasis. In the fully adjusted model, only hypertension remained at significantly increased risk (adjusted HR 1.33; 1.08–1.65).
Table IV. Risk of incident hospital-diagnosed cardiometabolic comorbidity in women with baseline psoriasis
Again, the isolated effect of the separate confounders for hypertension were examined and it was found that age was the most important, followed by smoking status. Adjustment for BMI alone did not affect the crude estimate (data not shown).
In a sub-analysis of severe baseline psoriasis, the increased risk of hospital-diagnosed hypertension was even more evident (adjusted HR 2.14; 1.02–4.49). An increased risk of T2D was also found in the overweight women with psoriasis (adjusted HR 4.50; 1.12–18.07) but this was based on very few cases. The absolute number of cases in the remaining categories was less than 3, and for reasons of confidentiality, the results cannot be shown.
In this study, of mainly younger women with psoriasis, an increased risk of early cardiometabolic comorbidity was found. After adjustment for the important confounders age, BMI, and smoking status, it was found that the risk of self-reported hypercholesterolaemia and hospital-diagnosed hypertension was significantly increased in women with psoriasis. Overall, these data support the idea that psoriasis is an important independent risk factor for cardiometabolic disease. The present study also shows the importance of taking the confounding effect of BMI and smoking into account.
In general, the results showed a unidirectional association between psoriasis and the comorbidities investigated. This supports the results of previous research on psoriasis and hypertension (11), ischaemic heart disease (3, 12), T2D (11, 13, 14), and hypercholesterolaemia (15, 16). Our results are also consistent with the hypothesis of there being an underlying common pathogenetic mechanism, such as the “psoriatic march”, as described in the Introduction (5).
Only self-reported hypercholesterolaemia and hospital-diagnosed hypertension were at significantly increased risk in the fully adjusted model, but the women in our study were young in relation to development of the comorbidities under investigation, and there was still a general tendency of increased risk. As shown by Gelfand et al., the increased risk of myocardial infarction in psoriasis is most obvious in younger patients with severe psoriasis (12). Our study supports the notion that psoriasis in younger patients carries an independent risk of cardiovascular risk factors and comorbidity, and that this might be even stronger in patients with severe psoriasis. In the case of self-reported metabolic syndrome, an extremely strong association was found, but it was based on only 3 cases, and could simply have been due to chance.
A highly significant interaction was found between psoriasis and BMI in relation to T2D, and we therefore performed the analyses with stratification according to BMI. Interestingly, it was only in overweight women that psoriasis was an independent risk factor for T2D, and to our knowledge this has not been found previously (17).
In the analysis of psoriasis in relation to self-reported comorbidity (Table II), there was a clear association between hypercholesterolaemia and psoriasis, which remained significant after adjustment for confounding factors. However, this was not as obvious in the analysis of hospital-diagnosed comorbidity (Table IV), even though the result was still in agreement with the result of analysis of the self-reported data. One reason for this could be that hypercholesterolaemia is most often treated by the general practitioner, and there is therefore no information available in the hospital-based registries. One way of circumventing this issue would be to use claimed medical prescriptions for certain drugs as a proxy for disease. This method is, however, not viable for a diagnosis such as hypercholesterolaemia. Although it is a disease that must be measured and diagnosed by a physician, many patients try dietary intervention or have no treatment at all, and the disease is therefore never recorded.
In contrast, a markedly increased risk of hypertension was found in the analysis of hospital-diagnosed comorbidity (Table IV) that was not identified in the analysis of self-reported data. One explanation for this could be that hypertension can be diagnosed at home and therefore might be over-reported in the self-reported data. Furthermore, the analysis of self-reported comorbidity had less power than the analysis of hospital-diagnosed comorbidity, since its study population was less than half the size. It is therefore possible that the risk contribution of psoriasis was attenuated, making it difficult to show any associations between psoriasis and hypertension in the smaller amount of self-reported data. A “healthy worker effect” among those who responded to the 11-year follow-up may also have reduced the prevalence of comorbidity in the self-reported data. This would not be a problem in the hospital data, since hypertension is diagnosed by trained professionals and the full baseline population is used. Here, however, there is a risk of surveillance bias due to patients with psoriasis possibly having more doctor’s visits and therefore being more likely to get a diagnosis of hypertension, so this should be kept in mind. We tried to address discrepancies in what is recorded by analysing both self-reported comorbidity and hospital-diagnosed comorbidity in the same population.
Women with psoriasis were identified on both a self-reported physician-diagnosed basis and a registry/hospital-diagnosed basis. The validity of the self-reported measure in the current study is high. As part of a clinical study, we have previously validated this self-reported physician-diagnosed psoriasis and could confirm the diagnosis in a satisfactory 80.8% of cases (18). Furthermore, in women with severe (hospital-diagnosed) psoriasis at inclusion time, 83.2% also reported having psoriasis in the DNBC. This validation of the psoriasis diagnosis is a strength of the current study compared with previous research (11). Self-reported data on the important confounders BMI and smoking were available, information that is not often available in the large registries. It was also possible to analyse both self-reported comorbidity and hospital-diagnosed comorbidity. It is known that some selection bias exists in the DNBC, and the participants are slightly healthier and have higher socioeconomic status than the source population; however, a study on the effect of non-participation showed no resulting bias for 3 different associations (19, 20). The better health and socioeconomic status, of course, affects women with and without psoriasis equally, but it can be speculated that it is more difficult to show significant associations with the comorbidities examined because there are fewer events overall in our cohort. In combination with the fact that the women are relatively young and therefore have not reached an age at which cardiometabolic diseases become prevalent, our results can be considered to be very conservative and may just be the “tip of the iceberg”. Our analyses of severe psoriasis were unfortunately limited by the low number of cases, but an even greater risk was clear in self-reported hypercholesterolaemia and hospital-diagnosed hypertension. The remaining results in the analysis of severe psoriasis have been presented with broad confidence intervals and should be interpreted accordingly. Regarding generalizability, our study was carried out in a female cohort and the results might therefore not be directly extrapolatable to the general population.
In conclusion, the present study shows that early screening for the classic cardiometabolic risk factors hypertension, hypercholesterolaemia, and hyperglycaemia may be of importance when treating patients with psoriasis, and that this also applies to younger patients. Furthermore, weight loss with regard to prevention of T2D appears to be even more crucial for patients with psoriasis. Our results support the underlying hypothesis of the “psoriatic march”.
The Danish National Birth Cohort was established with a significant grant from the Danish National Research Foundation. Additional support was obtained from the Danish Regional Committees, the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Health Foundation, and other minor grants. The DNBC Biobank has been supported by the Novo Nordisk Foundation and the Lundbeck Foundation.
Follow-up of mothers and children has been supported by the Danish Medical Research Council (SSVF 0646, 271-08-0839/06-066023, O602-01042B, 0602-02738B), the Lundbeck Foundation (195/04, R100-A9193), the Innovation Fund Denmark 0603-00294B (09-067124), the Nordea Foundation (02-2013-2014), Aarhus Ideas (AU R9-A959-13-S804), the University of Copenhagen (Strategic Grant IFSV 2012), and the Danish Council for Independent Research (DFF – 4183-00594 and DFF – 4183-00152).
This paper was supported by an unrestricted research grant from the LEO Foundation, and also from Herlev and Gentofte Hospital.
CZ has served as a scientific consultant for AbbVie, Pfizer, Janssen-Cilag, Merck & Co., Inc., Eli Lilly, Takeda, and Novartis and as a clinical study investigator for AbbVie, Amgen, Eli Lilly, Merck & Co., Inc., Takeda, LEO Pharma, and Novartis. LS has been a paid speaker for Pfizer, AbbVie, Eli Lilly, Novartis, and LEO Pharma, and has been a consultant or has served on Advisory Boards with Pfizer, AbbVie, Janssen Cilag, Novartis, Eli Lilly, LEO Pharma and Sanofi. She has served as an investigator for Pfizer, AbbVie, Eli Lilly, Novartis, Amgen, Regeneron, and LEO Pharma and has received research and educational grants from Pfizer, AbbVie, Novartis, Sanofi, Janssen Cilag, and LEO Pharma. CB, A-MNA, and AA have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize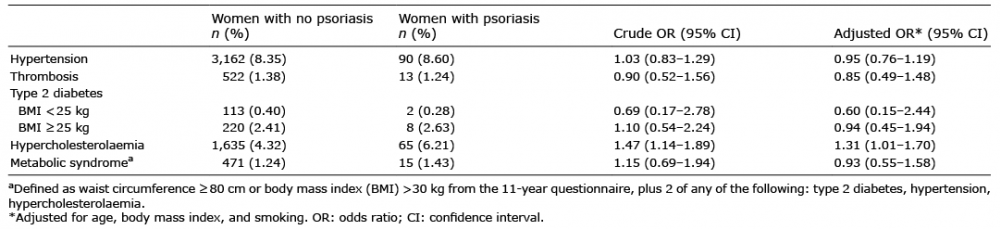 Click to show fullsize
Click to show fullsize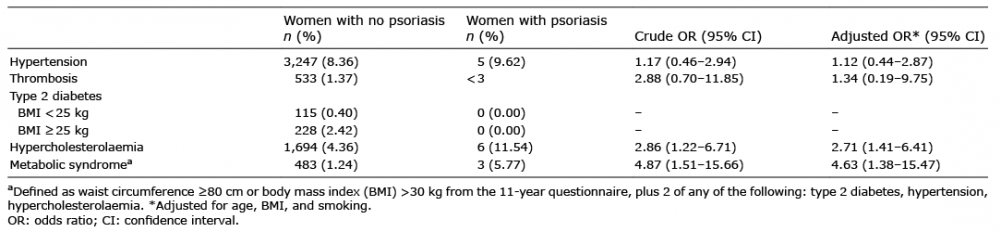 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize