


1Department of Dermatology and Allergy, Technical University of Munich, Munich, Germany, 2European Federation of Allergy and Airway Disease Patient’s Associations, Brussels, Belgium, and 3IMAS International, Munich, Germany
Atopic eczema is one of the most common non-communicable inflammatory skin diseases, and has a huge socioeconomic impact. Studies on the everyday economic impact of atopic eczema on patients, however, are limited. To estimate the annual extra out-of-pocket spending due to atopic eczema among patients in Europe, a cross-sectional study using computer-assisted phone interviewing of patients with atopic eczema was performed in 9 European countries. A total of 1,189 patients (56% women) with atopic eczema, who were either eligible for, or on, systemic treatment, participated in the study between October 2017 and March 2018. Mean extra spending on everyday necessities was €927 per patient per year for healthcare expenses, and this figure was slightly, but not statistically significantly, influenced by the severity of atopic eczema. Emollients and moisturizers accounted for the highest monthly costs, followed by medication that was not reimbursed, doctors’ and hospital costs. Atopic eczema-related out-of-pocket costs pose a substantial burden for affected individuals, are higher than in other chronic diseases, and should always be included in economic assessments of the impact of this disease.
Key words: atopic eczema; atopic dermatitis; economic impact; out-of-pocket costs.
Accepted Dec 6, 2018; E-published Dec 6, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Johannes Ring, Department of Dermatology and Allergy, Technical University of Munich, Biedersteiner Str. 29, DE-80802 Munich, Germany. E-mail: johannes.ring@tum.de
Atopic eczema is a skin disease with a huge impact on the everyday lives of affected patients’ and their families, but little awareness in the general population. This study including 1,189 people with atopic eczema living in 9 European countries found that extra out-of-pocket spending due to the atopic eczema is another setback with a mean amount of €927 spent by every patient per year. Out-of-pocket costs are a substantial burden in atopic eczema and much higher than in other chronic diseases. These costs should always be taken into account in individual as well as economic assessments of the disease.
Atopic eczema (AE, atopic dermatitis) is one of the most common non-communicable inflammatory skin diseases. It affects 1–3% of the adult population in Europe (1–3). The chronic or relapsing nature of AE, with itch as the predominant symptom, can have a huge impact on affected individuals (4). Several studies have shown that physical wellbeing and quality of life can be severely impaired, especially in patients with severe AE (5–8). However, to date, the impact and intensity of symptoms in the daily life of individuals with AE have gained limited attention. In particular, the economic implications of AE, including both the individual burden and the impact on the overall economy, have not been studied. Days missed at work due to AE, disease-related extra spending in different areas, such as clothing and cleaning products, as well as overall out-of-pocket payment per month for AE-related healthcare aspects can have a huge financial impact. With new insights into the pathogenesis of AE (9–11) and an increase in new treatment strategies and biologicals (12–16), the real-life economic impact of AE is gaining importance. The aim of this large European study was to assess this economic impact and, in particular, the out-of-pocket extra expenses due to AE in the daily life of affected individuals.
This cross-sectional study was conducted by telephone to ensure nationwide coverage, using computer-assisted telephone interviewing (CATI) in 9 large European countries (Czech Republic, Denmark, France, Germany, Italy, the Netherlands, Spain, Sweden and the UK). Individuals with AE who were candidates for systemic treatment or phototherapy or who were currently on systemic treatment or phototherapy were eligible for participation. Therefore, most of the study participants had initially had moderate-to-severe AE. Recruitment was based on physician referral (dermatologists, allergologists and general practitioners (GPs)) in all countries, whereas additional and alternative channels were also used in Denmark, Sweden, the Netherlands and the Czech Republic, e.g. via support groups or recommendation, in accordance with national regulations. To assess the economic burden, items were derived from validated questionnaires, tested for comprehension and practicability as well as for consistency, and then finalized after extensive discussion with experts. Participants were asked “Can you estimate how many days in a year you have missed work or study because of your atopic eczema? This could be because of visiting a doctor, not feeling well or anything else related to your eczema” and “Can you estimate how much money you have to pay out of your pocket per month on average for the following healthcare aspects for your atopic eczema, because these medical treatments are not (completely) reimbursed by a healthcare insurer or national health service?”. Furthermore, the assessment included spending on everyday necessities by reading out different areas for potentials extra spending. If the individual had extra expenses in these areas due to AE, they were asked to estimate the additional amount of extra spending as a percentage increase per month.
The current severity of AE among participants was assessed with the validated Patient Oriented Eczema Measure (POEM) (with the approval of the University of Nottingham) assessing the severity of symptoms, such as dry skin and itch, over the last 7 days (17) to allow comparison between severity of disease and economic impact. The POEM score ranges from 0 to 28 and differentiates between “clear/almost clear” (0–2 points), “mild” (3–7 points), “moderate” (8–16 points), “severe” (17–24 points) and “very severe” (25–28 points) severity of AE (18).
The study was approved by the local ethics committees of all participating centres in each country.
Additional expenses for the daily requirement (in Euro), as well as for the percentage increase were asked about as open questions and then categorized into suitable groups, such as spending less than €5. In countries with other currencies, the costs were converted into Euro according to the current official conversion rates from 5 February 2018. Mean spending, however, was calculated based on the actual values reported by the patients. Percenteages for total expenses were calculated from all individuals who did not report ”no expenditures”.
All statistical analyses were performed using SPSS software version 14.0.
A total of 1,189 patients (56% women) with AE participated in the study between October 2017 and March 2018, with a mean interview time of 25 min. A total of 180 patients were recruited in each of Germany, France, Spain, Italy and the UK, 150 in the Netherlands, 52 in the Czech Republic, 50 in Denmark, and 37 in Sweden. Of these patients, 55% (648) currently had mild AE or were clear of AE according to POEM, and 45% had moderate, severe or very severe AE. Thirteen percent of patients were in age group 18–29 years, 30% were 30–39 years, 35% were 40–49 years, and 22% were 50 years or older. With respect to education levels, 85% reported a higher and 15% a lower education according to their highest level of education (Table I).
Table I. Baseline of study population with atopic eczema (AE) in 9 European countries
Overall, 57% of patients had missed at least 1 day (1–5 days) and 26% at least 1 week (6–10 days) at work due to AE within the previous year, and 13% missed 11 days or more (Fig. 1). Most missed work days were reported by patients who had been recently diagnosed with AE, individuals receiving systemic treatment, those who were less satisfied with their treatment, and those with current moderate or severe AE.
Fig. 1. Number of work days missed due to atopic eczema within the last 12 months. POEM: Patient Oriented Eczema Measure.
Extra spending on everyday necessities is common among patients with AE. While only 5% of respondents did not report extra expenses, the vast majority of patients with AE spend in mean additional €927.12 per year on healthcare. The mean extra spending per month was €77.26, with emollients and moisturizers accounting for the highest monthly costs (€27.63), followed by €17.74 for medication and €8.68 for doctors and hospitals. Further additional mean monthly costs were identified in numerous other areas, such as phototherapy (€8.48), bandages (€7.12), travel expenses (€5.69), and in-patient treatment (€1.94) (Fig. 2).
Fig. 2. Mean out-of-pocket payment per month for several healthcare aspects of atopic eczema (AE) (in Euro; €). TP: test persons.
In addition to €927.12 on annual healthcare expenses, people with AE also have to spend extra money on everyday necessities. In general, most people spent extra money on personal hygiene products, representing a 18% additional expense per month. A total of 1,011 participants (85%) reported having to spend a mean of 18% extra on personal hygiene, 670 (58%) reported spending 9% extra on washing powder, 654 (55%) reported spending 8% extra on clothing, and 440 (37%) 7% extra on bedding. In addition, participants reported additional monthly expense on other everyday products, such as gloves, cleaning products, and food (Fig. 3).
Fig. 3. Extra spending in different areas of daily life due to atopic eczema (AE), as reported by patients (%). TP: test persons.
Healthcare expenses were not greatly influenced by the current severity of AE and appeared relatively stable. Extra monthly costs are also substantial for patients with clear or mild disease condition. There was a small difference in extra monthly spending of 9% (p = 0.181) between moderate/severe AE compared with the mild/clear condition. The main reason for this was that most expense is related to emollients and moisturizers, which are used by almost all respondents. Substantial differences, however, were seen between mild/clear AE and moderate/severe AE with respect to the mean number of days of work absenteeism and hospital stays. With increasing severity of AE, mean number of days spent in hospitals increased 1.36-fold and work absenteeism due to AE 3.85-fold.
This large cross-national survey with approximately 1,200 participants from 9 European countries demonstrates the substantial economic impact of AE on the daily life of patients and their families. Mean extra expense for an individual due to AE is €927.12 per year, which is not reimbursed. More than half of participants had missed at least 1 day, and 26% at least 6 days of work due to AE within the last year. This highlights the substantial impact AE has on the life of patients, not only with respect to the frequently reported substantial decrease in quality of life, but also in financial terms (4–6, 19, 20).
Previous studies of the financial impact of AE have focused mainly on direct and indirect costs. A study based on 32 patients with AE in South Korea, for example, estimated the total annual direct and indirect costs as approximately €3,200 per patient (21). For Spain, a recent study based on a review of registries of patients with AE seeking healthcare calculated direct and indirect costs as an overall mean of €1,504 per patient per year. Specifically for patients with mild, moderate and severe AE, they calculated €885, €2,111 and €3,397, respectively, per patient per year (22). None of these studies, however, included the out-of-pocket costs of individual patients.
To date, the out-of-pocket costs of AE in general have received only limited attention. An earlier study from the USA found that 36% of out-of-pocket costs are due to household items and 41% to medication (23). However, these data also included patients with AE without health insurance, who pay all of their healthcare costs including costs for emollients and over-the-counter (OTC) corticosteroids out-of-pocket, and therefore cannot easily be transferred to Europe with its healthcare insurance system. For Germany, annual out-of-pockets costs for patients with AE were assessed in a study with 148 participants in 2005 as a mean of €583 per year for every individual affected. The majority (€342) of this amount was the extra cost of everyday products, such as food, clothing, washing, etc. due to AE (24). These findings are consistent with our study, when corrected for inflation since 2005.
Compared with the out-of-pocket costs reported for other chronic diseases, the mean extra spend of €927.12 due to AE is high. For example, Jungen et al. (25) recently reported a mean of €224 ± €406 annual out-of-pocket costs for patients with psoriasis, whereas older studies estimated mean out-of-pocket costs for moderate-to-severe plaque-type psoriasis in Germany to be between €562 (26) and €794 (27) per year. This suggests that out-of-pocket costs today are higher for patients with AE than for those with psoriasis. However, our findings for AE are also higher compared with reported out-of-pocket costs for severe non-dermatological diseases. Patients with rheumatoid arthritis in Germany, for example, are reported have mean out-of-pocket expenses of €628 per year (28), patients with psoriasis arthritis €412 per year, and those with systemic lupus erythematosus €424 per year (29) (Table II).
Days of sick leave due to AE exceeded those of a similar study by van Os-Medendorp et al. (30), performed in the Netherlands in 2015. They reported self-reported sick leave due to AE in 42% of patients during the previous 12 months (30), compared with 57% in our large European sample. Due to this high level of burden and work loss, further analyses, as proposed by Nørreslet et al. (4) in their systematic literature review, would be beneficial.
Table II. Economic impact of atopic eczema (AE) compared with other diseases
A major strength was the inclusion of a large number of patients with AE from several large European countries in this study assessing real-life out-of-pocket expenses for everyday necessities due to AE. In particular, conducting interviews by phone with a mean duration of 25 min seems to allow a comprehensive estimation of the economic impact.
At the same time, the phone approach is also one of the main limitations of the study, since it might lead to bias with respect to interviewer, recall and social desirability. In particular, as the proportion of included patients with higher education above the respective national averages in all countries, selection bias cannot fully be excluded. Hypothetically, higher education could have led to a higher ability to pay for extra costs in general, which could have led to an overestimation of out-of-pocket costs. However, also asking respondents for a mean out-of-pocket expenses per month for healthcare expenses per corresponding area, and then extrapolating those to total yearly out-of-pocket expenses, might have biased the results. IIt is possible that not all areas were registered, some might have even been fully forgotten. In addition, although we do not know if the patients included in each country are representative of patients with AE in participating countries, the large number of patients across Europe ensures a sound insight in the financial impact of AE, with the limitation that all included participants were candidates for, or currently on, systemic treatment and thus had moderate-to-severe forms of AE. However, it should also be noted that emollients and moisturizers accounted for the greatest costs, the use of which on the whole-body surface is the basis for treating AE of whatever severity, including mild forms (16).
Calculating the direct and indirect costs does not fully meet the demands of evaluating the financial burden of AE with its complex impact on the daily life of patients. In addition to impairment of quality of life, the assessment of out-of-pocket costs is essential in evaluating the impacts of a disease. Considering the substantial amounts all of the patients with AE in this study spent each year due to the disease, future studies, and especially Health Technology Assessment for AE, should include out-of-pocket costs, which represent a high economic burden on society.
This study was supported by an unrestricted research grant provided by Sanofi Genzyme and Regeneron.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize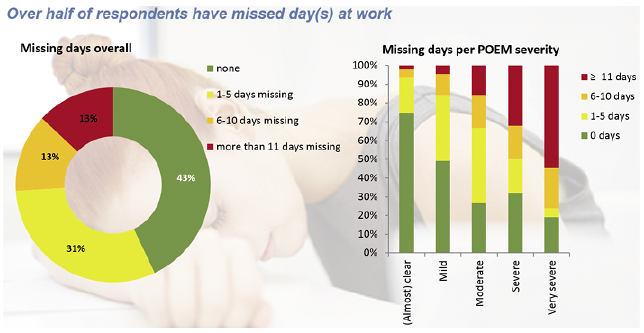 Click to show fullsize
Click to show fullsize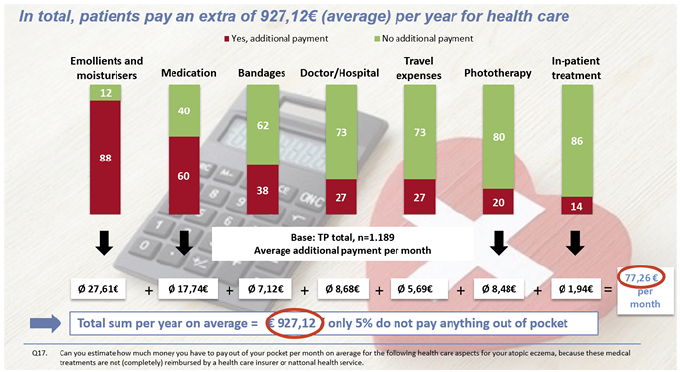 Click to show fullsize
Click to show fullsize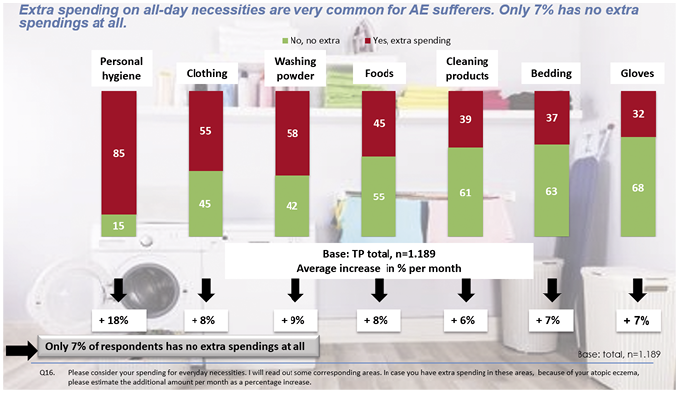 Click to show fullsize
Click to show fullsize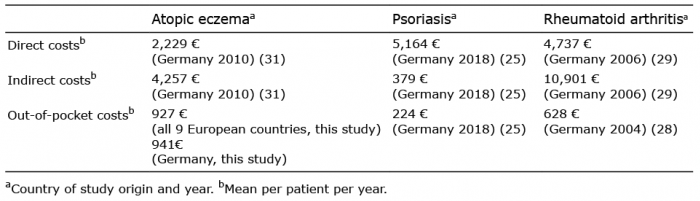 Click to show fullsize
Click to show fullsize