


¹PEDEGO Research Unit, University of Oulu, 2Department of Dermatology and Medical Research Center Oulu, 3Unit of General Practice, Oulu University Hospital, and 4Center for Life Course Epidemiology and Systems Medicine, University of Oulu, Oulu, Finland
Atopic dermatitis is associated with several comorbidities. Epidemiological studies on psychiatric comorbidities in adult atopic dermatitis patients are sparse. We analyzed psychiatric comorbidities in a Finnish nationwide adult atopic dermatitis cohort. The study included 57,690 adult patients with atopic dermatitis as cases and 40,363 individuals diagnosed with melanocytic naevi as controls. Data was obtained from the statutory Finnish Care Register for Health Care. The prevalence of preselected comorbidities between the atopic dermatitis and control groups was compared. Every psychiatric disorder studied was more common in patients with atopic dermatitis than in controls. At least one psychiatric diagnosis was found in 17.2% of the atopic dermatitis patients and 13.1% of controls. Psychiatric morbidity is significant in patients with atopic dermatitis and therefore assessing patients’ mental health status should be considered as part of standard care.
Key words: atopic dermatitis; comorbidities; mental disorder.
Accepted Mar 8, 2019; E-published Mar 8, 2019
Acta Derm Venereol
Corr: Laura Huilaja, Department of Dermatology, Medical Research Center Oulu, University of Oulu, Aapistie 5A, FIN-90220 Oulu, Finland; E-mail: laura.huilaja@oulu.fi
Atopic dermatitis is associated with several comorbidities. In this study we investigated psychiatric comorbidities of adult patients with atopic dermatitis. Our study shows that at least one psychiatric diagnosis was found in 17.2% of the atopic dermatitis patients. Actually, every mental diagnosis studied was more common in patients with atopic dermatitis compared to the melanocytic naevi controls. We report, for the first time, that atopic dermatitis is associated with both schizophrenia and bipolar disorders. Since psychiatric morbidity is significant in patients with atopic dermatitis, assessing patients’ mental health status should be considered as part of standard care.
Atopic dermatitis (AD) is the most common inflammatory skin disease (1). Most previous studies on psychiatric comorbidities focused on attention-deficit hyperactivity disorders in children with AD (2). Only recent studies take into account the possible association of AD with different psychiatric diseases in adults (3–8).
Register studies from Taiwan and the United States (5, 7) have reported an association between both anxiety and depression and AD in adults. In addition, a South Korean study found an increased risk for anxiety in AD patients (6). In contrast, a recent Danish study found no heightened risk for either anxiety or depression in patients with AD, although an increased use of anxiolytic or anti-depressive medication was found (8).
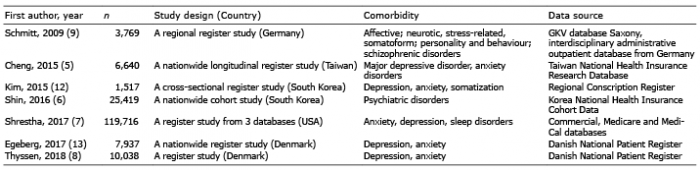
Only one previous study has reported the associations between AD and psychiatric comorbidities other than depression or anxiety in adolescent and adult patients with AD. AD was found to be associated with affective, stress-related, behavioural disorders and psychoses (9). Epidemiological data on AD are largely based on self-reported questionnaire studies (Tables I and II) (3, 10, 11, 14–17, 19) and previous results concerning the association of anxiety and depression with AD are inconsistent (5–8). To clarify the associations between AD and its psychiatric comorbidities at a national level, we conducted a retrospective study using the Finnish Care Register for Health Care (CRHC).
Table I. Register studies about atopic dermatitis and its psychiatric comorbidities in the adult population
Table II. Survey studies about atopic dermatitis and its psychiatric comorbidities
This was a retrospective register study of adult cases of AD diagnosed in Finnish hospitals between 1st January 1987 and 31st December 2014. Patient records were obtained from the CRHC, which is maintained by the National Institute of Health and Welfare. Records with a diagnosis of AD (code 6918B in the International Classification of diseases [ICD]-9, and L20.0 in ICD-10) were selected. The CRHC covers all hospitals in Finland and the outpatient visits from 1998 onwards are also included. The unique social security number, given to every Finnish citizen, ensures that a person is included in the CRHC only once. In Finland, ICD-9 was used between 1987 and 1995, and ICD-10 has been used since 1996. In this study, the control population was comprised of patients diagnosed with melanocytic naevi (ICD-9: 2160-9A and ICD-10: D22) during the same period. Patients diagnosed with melanoma (ICD-9: 172 and ICD-10: C43 and D03) were excluded from the melanocytic naevi control population. Patients were defined as having AD or melanocytic naevi when they had at least one documented diagnosis of the disease in question in the CRHC database. If a case had both AD and melanocytic naevi diagnoses, it was included in the AD group. Since this study focuses on the comorbidities in adults with AD, only patients who had reached the age of 25 by the end of the study period, were included in the analysis. The psychiatric diagnoses, including both primary and subsidiary diagnoses (Table III), as well as sex, were gathered for both AD and control patients from the CRHC. The initial database query yielded records for 142,745 patients with AD and 40,363 with melanocytic naevi. Of these, all AD cases aged > 25 years (n = 57,690) were included in the present study and compared with melanocytic naevi controls from the same age group.
Table III. Diagnoses of psychiatric comorbidities included in the study
The characteristics of the patients with AD and controls with melanocytic nevi are summarized in Table IV. At least one mental disorder was diagnosed in 17.2% of patients with AD compared with 13.1% of controls (odds ratio [OR] 1.25, 95% confidence interval [CI] 1.20–1.30). All the psychiatric diagnoses studied were significantly more common in the AD group compared to the controls (Table V).
Table IV. Characteristics of patients in atopic dermatitis (AD) and melanocytic naevi groups
Table V. Comorbidities in patients with atopic dermatitis (AD) (n = 57,690) and melanocytic naevi (naevi) (n=40,363) controls
Mental disorders were more frequent in women than in men with AD: at least one psychiatric disorder was present in 18.6% of women and 14.8% of men. Each of the psychiatric disorders included in the study was more common in women than in men with AD, apart from the “psychotic disorders” (present in 2.4% and 3.0% of female and male patients, respectively); “schizophrenia and schizotypal disorder” (present in 1.0% and 1.5% of female and male patients, respectively) and “disorders of adult personality and behaviour” (present in 2.2% of both women and men). In patients with melanocytic naevi, all mental disorders were more frequent in women than in men, except for the “psychotic disorders” which were equally as common in both sexes. While the risk for “any psychiatric disorder” was greater in AD patients than in controls, regardless of sex, there was no significant sex difference in this metric. However, the association between AD and “psychotic disorders” was significantly stronger in men than in women (OR 1.66 in men vs. 1.42 in women, p = 0.01), whereas the risk for anxiety disorders was found to be significantly higher in women (OR 1.19 in women vs. 1.05 in men, p = 0.04) (Fig. 1). No significant differences in the risks of mental disorders were found between sexes in other psychiatric diagnoses studied.
Fig. 1. Odds ratios for psychiatric disorders stratified by sex in patients with atopic dermatitis compared to controls.
The main finding in our study was that patients with AD have a higher risk for all psychiatric comorbidities than the controls: at least one psychiatric diagnosis was reported in 17.2% of patients with AD and in 13.1% of those with melanocytic naevi. Previously, only a regional German study reported the association between AD and several psychiatric comorbidities (9). It found that 34% of patients with AD had at least one psychiatric diagnosis. While this proportion appears to be much higher than the 17% identified in our study, it is worth noting that almost 75% of the psychiatric diagnoses in the German study were classified as “neurotic, stress-related and somatoform disorders”, which may reflect a possible selection bias, since the data were gathered from an insurance-based health register only.
We found that, among all psychiatric diagnoses studied in patients with AD, the risk for depression was the most pronounced, being present in 10.4% of AD patients. This finding is in line with previous register studies (Table I): In the Taiwanese study, AD patients had a seven-fold greater risk for major depression and almost a six-fold greater risk for any depressive disorder, compared with the age- and sex-matched control group (5). The register study from the US has also reported AD to be significantly associated with depression (7). In the Taiwanese register-based case-control study, five to six-fold increase in the risk for major depression and any depressive disorder in the AD populations were found (5).
Anxiety disorders have been associated with AD in register studies (Table I), and anxiety was the third most common psychiatric comorbidity in AD patients in our study. Our findings are comparable to studies from the United States (7) and South Korea (6), which reported that patients with AD are twice as likely to have an an-xiety disorder as healthy individuals. In contrast to other register study findings and our results, the recent Danish register study (8) found that moderate-to-severe AD was associated with an increased risk of antidepressant and anxiolytic medication use, but not with depression or anxiety. Although their study was nationwide, the limited size of their study population may have affected their findings.
Until now, only the regional German study (n = 3,769) had reported an association between AD and stress-related, behavioural and affective disorders and psychoses (9). “Neurotic, stress-related and somatoform disorders” was the second most common category of psychiatric diagnoses, present in 9.1% of patients with AD in our study. The German study found a surprisingly high prevalence of this category, which, being present in 27.4% of the AD population, was the most common psychiatric diagnosis (9). However, the study was regional and partially based on insurance-covered health data, which may explain the higher prevalence rate in comparison to the present study.
Here, we show an association between schizophrenia, bipolar disorder and AD that, to our knowledge, has not previously been reported. Both “schizophrenia and schizotypal disorder” and “bipolar disorder and manic episodes” were significantly more common in patients with AD than in the control group. Previously, an association between AD and psychoses (OR 1.46) was reported (9), but schizophrenia, as a distinct diagnosis, was not studied and bipolar disorders were included in the group of affective disorders.
We found that mental disorders in general were more frequent in women than in men with AD. Only “psychotic disorders” (3.0% vs. 2.4%) and “schizophrenia and schizotypal disorder” (1.5% vs. 1.0%) were more common in males. It is known that mental disorders are more common in female dermatological patients in general (18). A South Korean study reported a surprisingly high prevalence of depression (10.4%), anxiety (9.8%) and somatization (11.7%) in young adult males with AD (19) but it was conducted only among male conscripts and had a small study sample (n = 1 517). Furthermore, the psychiatric diagnoses were defined and classified by military health officers, which may have led to overestimation of the prevalence of these disorders. Interestingly, although the overall prevalence of mental disorders was greater in females, they seemed to not have a heightened risk for psychiatric morbidity in general. We found females with AD to have a higher risk for the “anxiety disorders” only, compared to men with AD.
The underlying causes of the psychiatric comorbidity in patients with AD are not completely understood. Intense pruritus, sleep disturbance, emotional stress, social stigma and increased levels of cytokines common to both dermatological and psychiatric conditions are commonly suggested as aetiological factors (20). Being a chronic disease, AD places a heavy, long-term burden on patients and their families, resulting in a serious impact on their daily lives, which may lead to psychiatric comorbidities. Chronically elevated levels of pro-inflammatory cytokines, which cross the blood-brain barrier, have been reported in prolonged atopic eczema; this effect has been hypothesized to function as a risk factor for autism spectrum disorders, and possibly other psychiatric comorbidities, in AD patients (21).
The major strength of our study is that it is a population-based epidemiological study with one of the largest AD populations ever studied. Another strength is that all diagnoses were made in a specialized setting. Our findings in the control group are comparable to the general population (22–24), which further strengthens our results.
A weakness of the study is that it was not possible to verify the accuracy of the AD diagnosis. We had no information on the disease severity or patients’ socioeconomic status and were unable to analyze the association with psychiatric morbidity. We cannot exclude the possibility that some control individuals had AD that was treated only in primary care. Based on our registry data we were unable to analyze any temporal relationships between AD onset and psychiatric diagnoses. In addition, our results were not adjusted to the possible somatic comorbidities.
This study provides new population-based epidemiological information about AD and its psychiatric comorbidities in adults on a national level. Our findings emphasize the important role of dermatologists in evaluating mental health of AD patients (25), especially if there are difficulties with compliance.
IRB approval status: This study was exempted from review by the IRB (Ethical committee of Northern Ostrobothnia Hospital District) since it was a register-based study.
Conflicts of interest: SK has received educational grants from Novartis, Leo Pharma, SanofiGenzyme, AbbVie, Janssen-Cilag and honoraria from SanofiGenzyme for speaking. KT has received educational grants from Novartis and Pfizer and honoraria from Novartis, Abbvie, Janssen-Cilag, SanofiGenzyme and Lilly for consulting and/or speaking. LH has received educational grants from Shire, Janssen-Cilag, Novartis, AbbVie and LeoPharma, honoraria from Novartis, Abbvie and UCB Pharma for consulting and/or speaking and is an investigator for Abbvie. JJ and MT have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize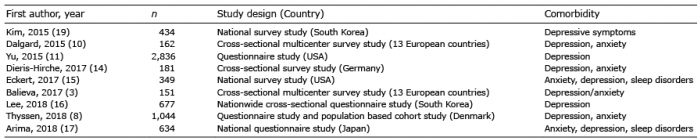 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize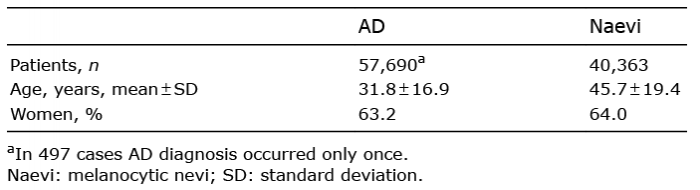 Click to show fullsize
Click to show fullsize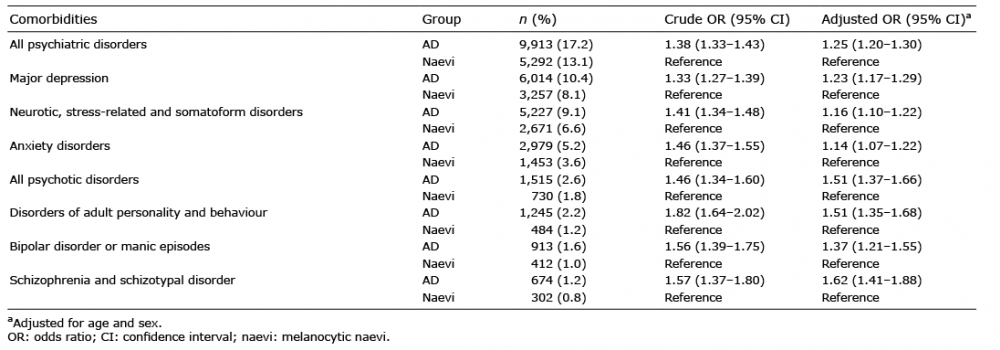 Click to show fullsize
Click to show fullsize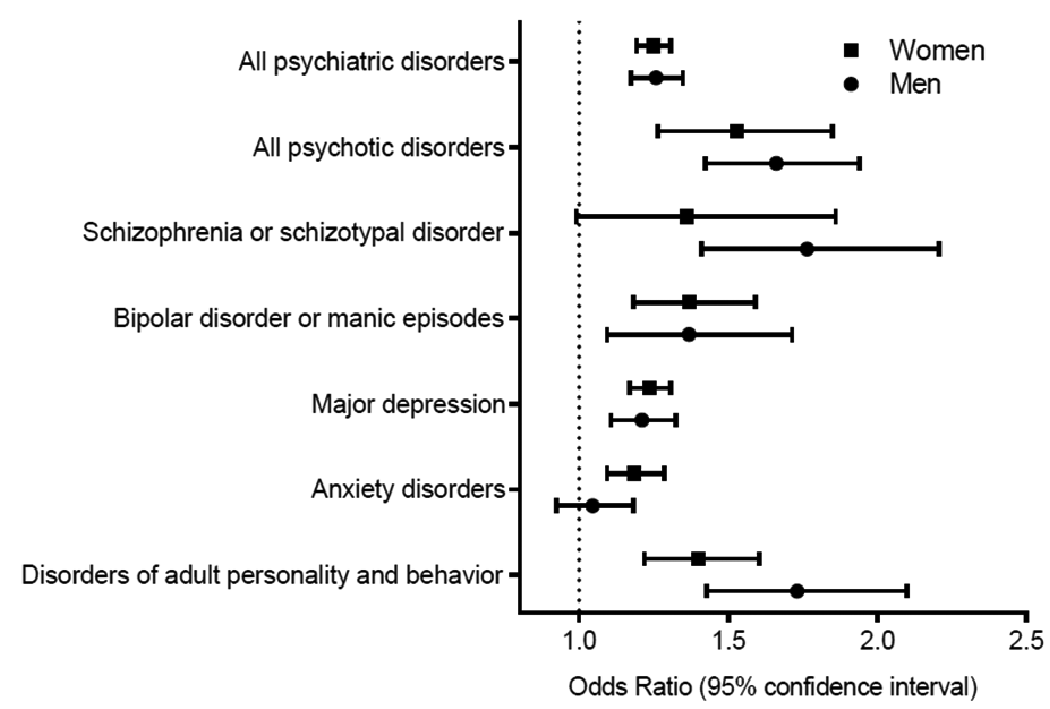 Click to show fullsize
Click to show fullsize