


Kungsholmens Hudklinik, Warfvinges Väg 35, SE-115 21 Stockholm, Sweden. *E-mail: carl.swartling@svettmottagningen.se
Accepted Mar 8, 2019; E-published Mar 8, 2019
Morbihan syndrome (MS) is a rare condition that is considered either a subtype (1) or a late-stage complication of rosacea (2). While its pathogenesis is not fully known, it is characterised by the clinical features of erythema and overt oedema of the upper two-thirds of the face. The erythematous oedema is accompanied by telangiectasias, and occasionally by papules, pustules and nodules. The swelling and distortion in the disease cause visual impairment, discomfort and cosmetic concerns (1, 2). The abundance of mast cells, producing vasoactive substances, proteases and cathelicidins, such as Cath-37, may be important in the pathogenesis of rosacea as well as of MS (3), and studies indicate that the antihistamine ketotifen shows beneficial outcome in the treatment of rosacea (4). Omalizumab is a humanised monoclonal antibody that binds the circulating IgE antibodies and may stabilise mast cells in the treatment of chronic urticaria (5). Typical flushes in MS and rosacea are similar to the temporary erythematous swellings observed in urticaria and angioedema. Accordingly, we hypothesize that omalizumab could stabilize mast cells in MS and reduce the temporary swelling.
A 56-year-old woman, with moderate erythematous rosacea, developed persistent and prominent erythematous oedema of the face (Fig. 1A), lasting for one year. Firm swelling of the eyelids, impairing vision, accompanied oedema of the cheeks and forehead. Neither itching nor scaling was observed. Pronounced swelling was seen after exposure to hot, cold and windy weather, and to a lesser extent to stress, sunlight and spicy food. The patient could not work or participate in the social events, due to her symptoms. She was diagnosed with Morbihan disease after excluding allergies, various connective tissue diseases such as dermatomyositis and superior vena cava syndrome.
The patient was tested with a normal skin prick test, tryptase, antinuclear antibodies, thyroid function test, full blood count and X-ray of the lungs and mediastinum. Skin punch biopsy demonstrated non-specific inflammation consistent with rosacea.
MS was treated with lymecycline 300 mg twice daily for 3 months and later isotretinoin 10–20 mg daily for 4 months, but there was no effect on the swelling or erythema.
Because of the temporary swelling caused by physical stimuli, in addition to the permanent oedema, we initiated a trial treatment with omalizumab 450 mg subcutaneously.
A dramatic reduction in the swelling was seen 1–2 weeks post-treatment (Fig. 1B) and the patient subsequently became tolerant to the physical stimuli. The MS cleared completely after 5 months of monthly omalizumab injections, an initial dose of 450 mg and consecutive doses of 300 mg (Fig. 1C). Maintenance treatment was given for a further two months, every 4–6 weeks, and was then discontinued successfully without clinical relapse, 6 months later. The quality of life was markedly improved after omalizumab injections and the patient was able to resume working, instead of being on sick leave.
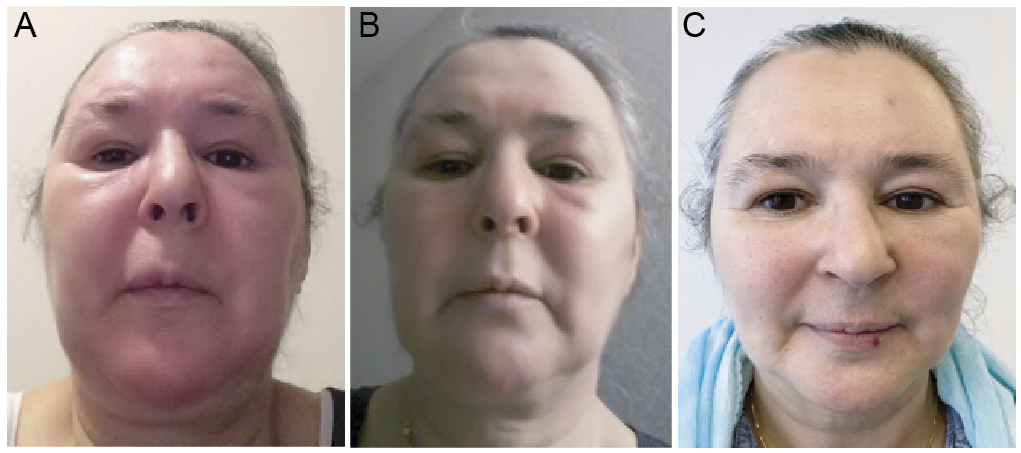
Fig. 1. A) Pre-treatment photo of prominent and persistent erythematous edema of the face. Firm swelling of the eyelids impairing vision. The patient was on sick leave. B) A reduction of the edema was observed two weeks after the first subcutaneous injection with the monoclonal antibody - omalizumab 450 mg. The patient tolerated windy and cold weather and noticed less tenderness. C) The patient is in her normal condition after monthly injections of omalizumab for five months. Her quality of life was substantially improved, and she was able resume normal life, including returning to work. A written permission from the patient to publish these photos was obtained.
Our case report explores omalizumab as a therapy option in the treatment of MS, especially when the swelling attacks are observed in response to physical stimuli. The patient was completely symptom-free 5 months after the initiation of the monthly omalizumab injections, and 6 months after receiving the last injection she still showed no signs of erythematous oedema or swelling. No side effects were reported.
Antihistamines are the first-line treatment for urticaria and angioedema, and omalizumab is the second-line option for the treatment of refractory chronic cases not responsive to antihistamine (6). Omalizumab has been shown to be a potent drug in the treatment of severe cases of urticaria with few side effects (7). Subcutaneous injection of omalizumab may stabilise the mast cells, by decreasing Fc receptors on the cell surface, in addition to binding the circulating IgE (8). The flushes seen in MS and rosacea are similar to those in urticaria and angioedema. Improvement in symptoms with the use of omalizumab was therefore hypothesized. Additional arguments for initiating a trial treatment with omalizumab were: previously positive results of ketotifen in the treatment of rosacea (4), and the abundant mast cells in rosacea-affected skin on histological examination (2, 9). Surprisingly, not only did the temporary flushes subside after the repeated omalizumab injections but also the permanent swelling disappeared. The patient could already tolerate cold, hot and windy weather after only one injection of omalizumab. After the additional two injections the permanent swelling was markedly reduced. Tetracyclines, which presumably work by inhibiting the metalloproteases in MS, were not sufficient to improve the patient’s condition. The patient also failed to respond to isotretinoin, perhaps due to the absence of the papulo-pustular phenotype. Without guidelines, we chose a higher initial dose of omalizumab (450 mg) than recommended for urticaria, to achieve a supramaximal effect. However, a good clinical response was also maintained with the traditional dose of 300 mg monthly. The pathogenesis of MS is still obscure. It is proposed that MS is a late stage or variant of rosacea (1). The facial skin is an area with sympathetic, parasympathetic and nociceptive C-fibres, which all have the potential to create vasodilation and oedema. Subsequently, corresponding stimuli such as stress (sympathetic β-adrenergic fibres) heat (sudomotor fibres), gustatory (parasympathetic fibres) and noxious (nociceptive C-fibres) may lead to deterioration of rosacea and MS. The mast cells seem to play an important role in the pathogenesis of rosacea and MS by producing the precursor to Cath-37 and the necessary proteases to activate the microbial peptide. Cathelicidins from keratinocytes are also activated by proteases from mast cells. Cath-37 attracts immune cells and provokes inflammation as well as angiogenesis, which are typically observed in rosacea and MS (3, 9). Furthermore, upon stimulation, mast cells liberate several vasoactive substances, leading to oedema and inflammation. In addition to humoral stimulation, the mast cells are also activated by nociceptive C-fibres and are subsequently important cells in neurogenic inflammation (10). The trigeminal nerve responds to noxious stimuli, and its sensory function is complemented by a motor axon reflex, with liberation of vasoactive neuropeptides, such as substance P (11), producing the typical flare, which is augmented by degranulation of the innervated mast cells. In case report studies, botulinum toxin has been successfully used in rosacea (12, 13). Botulinum toxin inhibits the release of neuropeptides from the nociceptive C-fibres as well as from sudomotor fibres (14). The flare and innervation of mast cells are subsequently inhibited. The option of botulinum toxin injections was proposed as an alternative to omalizumab, but the patient declined, due to a fear of needles. In conclusion, omalizumab injections were successfully used in the treatment of MS. These findings highlight mast cells as a key cell in the pathogenesis of rosacea and MS.
CS is the owner of Svettmottagningen (Stockholm), Svedklinikken (Copenhagen), Svetteklinikken (Norge) and Sweat Clinic (London). PK and IE have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize