


1Department of Dermatology, Nara Medical University School of Medicine, 840 Shijo, Kashihara, Nara 634-8522, Japan, 2Department of Surgical Pathology, and 3Department of Ophthalmology, Kyoto Prefectural University of Medicine, Kyoto, Japan. E-mail: fumim@naramed-u.ac.jp
Accepted Mar 13, 2019; E-published Mar 14, 2019
Iatrogenic immunodeficiency-associated lymphoproliferative disorders (LPD) are lymphoid proliferations or lym-phomas that arise after treatment with immunosuppressive drugs (e.g. methotrexate) (1). LPD are strongly associated with Epstein-Barr virus (EBV) infections, probably due to defective immunosurveillance.
Pseudolymphoma is characterized as a benign reactive polyclonal T- or B-cell lymphoproliferative process, which clinically and histologically simulates cutaneous lym-phoma (2, 3). We describe here an unusual case, in which cutaneous B-cell pseudolymphoma-like lesions arose on 2 different organs, the lip and conjunctivae, in a patient who received long-term treatment with cyclosporine for prurigo. As histological examinations of both sites revealed follicular hyperplasia with scattered EBV-positive cells, it might be appropriate to refer to these lesions as iatrogenic immunodeficiency-associated LPD, although they do not fit into any of the immunodeficiency-associated LPD categories listed in the 2017 World Health Organization (WHO) classification (1).
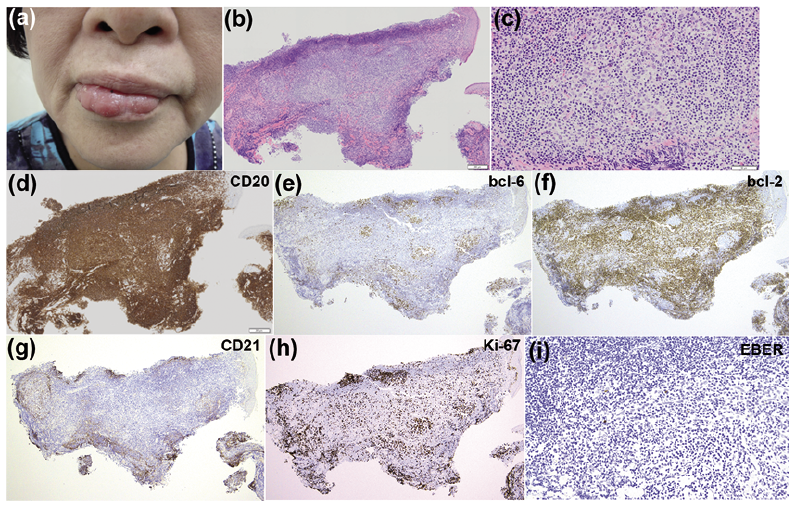
A 72-year-old woman presented with swelling of the lower lip, which had evolved over a 5-month period. Her medical history included diabetes mellitus and prurigo nodularis. She had been treated with 100 mg cyclosporine per day for approximately 10 years for intractable generalized prurigo, which often recurred when the dose of cyclosporine was reduced. Clinical examination revealed an elastic, soft, red-coloured tumour, which covered almost the entire lower lip (Fig. 1a). Laboratory investigations detected the following abnormal values: white blood cell count 95×102/µl (reference range 33–86×102/µl), lactate dehydrogenase 318 U/l (124–222 U/l), creatinine kinase 186 U/l (41–153 U/l), alkaline phosphatase 460 U/l (106–322 U/l), blood urea nitrogen 22 mg/dl (8–20 mg/dl), creatinine 0.93 mg/dl (0.46–0.79 mg/dl), soluble interleukin-2 receptor 563 U/ml (145–519 U/ml) and IgG4 188 mg/dl (4.5–117 mg/dl). Tests for anti-SS-A and anti-SS-B antibodies were negative. A skin biopsy demonstrated dense nodular lymphocytic infiltrates with germinal centres (GC) surrounded by dense infiltrates of small round lymphocytes admixed with plasma cells and eosinophils (Figs. 1b, c). Most of the cells in the infiltrates were positive for CD20 (Fig. 1d), and a small number were positive for CD3. The cells in the GC were positive for CD20 (Fig. 1d), CD10, and bcl-6 (Fig. 1e), and negative for bcl-2 (Fig. 1f). The networks of CD21+ follicular dendritic cells were confined to the GC (Fig. 1g). Ki-67 staining showed high proliferation rates in the GC (Fig. 1h). In situ hybridization for EBV-encoded small RNA (EBER) showed scattered positive cells (Fig. 1i). Few IgG4+ plasma cells were present. In situ hybridization and gene rearrangement studies confirmed that light-chain restriction and immunoglobulin heavy chain rearrangement, respectively, were absent. Positron emission tomography/computed tomography did not show any extracutaneous lesions. The patient was diagnosed with cutaneous B-cell pseudolymphoma (2).
Fig. 1. Clinical and histopatho-logical findings of the lip lesion. (a) A reddish tumour on the lower lip. (b) Skin biopsy revealed a dense infiltrate of small lymphocytes in the dermis, admixed with plasma cells and eosinophils (haematoxylin and eosin; ×20). (c) A higher magnification image of (b) (×200). (d) Immunohistochemistry showed that the dense infiltrate of lymphocytes was positive for CD20 (×40). (e–h) Immunohistochemistry showed that the cells in the follicles expressed bcl-6 (e), but were negative for bcl-2 (f). CD21+ follicular dendritic cells were restricted to the germinal centres (GC) (g). Ki-67 staining showed high proliferation rates in the GC (h) (×40). (i) In situ hybridization for EBV-encoded small RNA (EBER) showed scattered positive cells (×200).
Three months prior to the appearance of the tumour on her lip, the patient had developed a salmon-coloured nodule on her right conjunctiva (Fig. S1a). She was referred to the ophthalmology department and underwent an excisional biopsy, followed by topical steroid therapy, which resulted in resolution of the conjunctival lesion. Histopathological examination of the conjunctival nodule revealed a dense infiltrate of mature lymphocytes within the conjunctival substantia propria, with multiple nests of lymphocytes forming follicles with GC (Fig. S1b). The immunohistochemistry results were similar to the skin biopsy findings; i.e. the follicle-forming cells were positive for CD20 (Fig. S1c), CD10, bcl-6 (Fig. S1d), CD21 (Fig. S1e) and Ki-67 (Fig. S1f) and were confined to the GC. Bcl-2 was not detected (Fig. S1g), but scattered EBER-positive cells were seen within the GC (Fig. S1h). No light-chain restriction was detected. A diagnosis of reactive lymphoid hyperplasia (RLH) of the conjunctiva was made.
Approximately 6 months after excision of the conjunctival nodule, new nodules appeared on both lower conjunctivae (Fig. S1i). The nodules on the conjunctivae and the tumour on the lip gradually increased in size. At 3 months after the patient’s initial visit to the Department of Dermatology, cyclosporine treatment was discontinued, but oral prednisolone (PSL) was initiated at a dose of 25 mg/day to treat intractable prurigo. The tumour on the patient’s lip and the nodules on her conjunctivae completely disappeared within 10 days. The oral PSL dose was gradually tapered. However, when the PSL dose was decreased to 5 mg every other day, the lesion on the lower lip recurred. Thus, the PSL dose was increased to 15 mg and maintained at 7.5 mg/day. No recurrence has been observed since.
The patient was initially diagnosed with B-cell pseudolymphomas of the lip and conjunctivae based on immunohistochemical and molecular examinations (2). Cutaneous pseudolymphomas (CPL) are divided into T- and B-cell pseudolymphomas, depending on the predominant cell type in the associated infiltrates (2, 3). Although pseudolymphomas appear more often in the skin, other organs, including the eyes, can be affected (4). CPL, especially T-cell CPL, are sometimes associated with particular drugs (most commonly anti-epileptic agents) (3). Rare cases of cyclosporine-related T-cell (5) or B-cell (6, 7) CPL have been reported. However, in the present case the lesion on the lower lip recurred after the PSL dose was tapered, even though the cyclosporine therapy had been stopped, suggesting that the lesions were not directly caused by cyclosporine. Another possibility is that pseudolymphomas occur as skin manifestations of IgG4-related diseases (8). Although the serum level of IgG4 was slightly elevated in our patient, the low number of IgG4+ plasma cells and the absence of fibrosis in the skin biopsy specimens and the absence of systemic manifestations meant that this possibility could be excluded. The involvement of multiple sites and a relapsing course are unusual for B-cell pseudolymphoma; thus, we examined the patient for a persistent underlying infection, and EBV was detected in the lesions. Since the patient had been treated with cyclosporine for many years, and a few EBV-positive cells were seen in the lesions, iatrogenic immunodeficiency-associated LPD should be considered (1). Iatrogenic immunodeficiency-associated LPD constitute a spectrum, ranging from polymorphic infiltrates with polyclonal lymphoid or plasmacytic proliferations to a subset of B-cell lymphoma. They often involve extranodal sites, such as the skin and gastrointestinal tract (1). The histology of the lip and conjunctivae in this patient might best fit into the category of florid follicular hyperplasia in a post-transplant setting (9); however, the finding of follicular hyperplasia in iatrogenic immunodeficiency-associated LPD has not been described in detail.
This case exhibited an uncommon presentation; i.e. pseudolymphoma-like lesions developed on the lip and conjunctivae. The detection of EBV might indicate underlying immunodeficiency. Histological examinations revealed follicular hyperplasia in all of the lesions, suggesting that this case might be a precursor of iatrogenic immunodeficiency-associated LPD, although follicular hyperplasia is not mentioned in the current WHO classification (1). Thus, this case might expand the histological spectrum of iatrogenic immunodeficiency-associated LPD. Finally, ocular lesions are usually reported under the name RLH in the ophthalmological field (10). Our patient’s findings suggest that RLH of the ocular surface and CPL are basically identical entities.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize