


1National Skin Centre, Singapore, and 2Headquarters Medical Corps, Singapore Armed Forces, Singapore
#These authors have contributed equally and should be considered as first authors.
Atopic dermatitis (AD) is a systemic inflammatory disorder. However, the relationship between severity of AD and metabolic and atopic conditions is not well studied. The aim of this study was to elucidate the relationship between severity of AD and comorbidities, such as metabolic conditions (increased body mass index, hypertension, hyperlipidaemia, and type II diabetes mellitus) and other atopic manifestations (allergic rhinitis, asthma and food allergies). A retrospective population-based national study of a cohort of young adult males conscripted into military service in Singapore over a 5-year period was performed, utilizing military electronic medical records. A dose-dependent effect was found between the association of comorbidities and severity of AD. Metabolic and atopic conditions were significantly correlated with having moderate-to-severe AD. An association of metabolic and atopic conditions with severity of adult AD was found, which suggests that chronic severe AD may result in increased disease burden and morbidity.
Key words: atopic dermatitis; eczema; co-morbidities; atopy; metabolic.
Accepted Mar 21, 2019; E-published Mar 21, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Yik Weng Yew, National Skin Centre, 1 Mandalay Rd, 308205 Singapore, Singapore. E-mail: yikweng.yew@mail.harvard.edu
- Associations between metabolic and atopic diseases with atopic dermatitis severity are not well described.
- Positive correlations were found between metabolic and atopic co-morbidites and an increasing severity of AD in our study.
- Management of metabolic and atopic co-morbidities, is important in the holistic management of adult AD.
Atopic dermatitis (AD) is a chronic relapsing inflammatory skin disease with several reported disease associations (1), which affects up to 10% of adults (2). Comorbidities, such as metabolic conditions (increased body mass index (BMI), hypertension, hyperlipidaemia, diabetes mellitus) and atopic conditions (allergic rhinitis, asthma and food allergies) are reportedly associated with a higher risk of adult AD (3–7). AD has been described as a systemic inflammatory and allergic skin disease (1); hence the presence of metabolic comorbidities and atopic conditions in patients with AD is postulated to lead to a chronic inflammatory state, which perpetuates disease progression, leading to a more severe form of AD (8, 9). With a paucity of studies examining the link between comorbidities and the severity of AD in adults (10, 11), the aim of this study was to further investigate the postulated associations in the Singapore population.
Singapore is an urbanized, multi-ethnic society with an increasing prevalence of AD, atopic and metabolic conditions, similar to that in other developed countries (2, 12). Singapore also has a predominantly conscript army, which requires all eligible male adult citizens to undergo baseline medical health screening prior to enlistment for military service. Utilizing the data from this national military electronic medical record (EMR), this study examined, in a national cohort of young adult males, the hypothesis that metabolic and atopic comorbidities are associated with increased severity of AD.
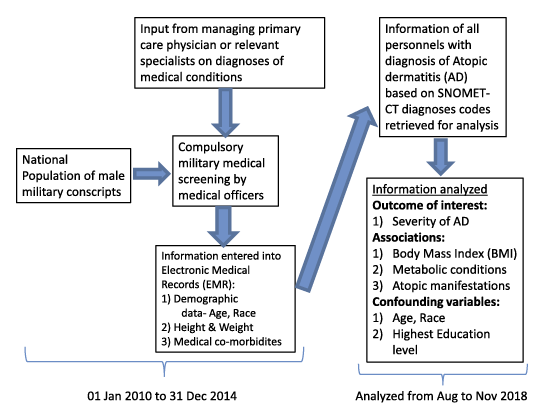
The study cohort consisted of all military conscripts with a diagnosis of AD made during their military medical screening from 1 Jan 2010 to 31 Dec 2014. Subjects were identified from the Singapore Armed Forces EMR using validated Systematized Nomenclature of Medicine - Clinical Terms (SNOMET-CT) diagnosis codes (D0-10130, D0-10183-87). Diagnoses of hypertension, hyperlipidaemia, type 2 diabetes mellitus, allergic rhinitis, asthma and food allergies were retrieved from the EMR using SNOMET-CT diagnoses codes. During their medical screening, all cases had their diagnosis codes documented in the military health records after assessment by military medical officers with verification from the relevant specialists.
Information such as demographic data (age, ethnic groups), highest education level achieved (as a surrogate marker for socio-economic status) and anthropometric measurements, such as height, weight and BMI, were retrieved for analysis as covariates and potential confounders (Fig. 1). Severity of AD for each subject was recorded in the EMR as mild, moderate or severe. This physician-based severity classification was global and based on the body surface area affected, frequency of disease flare, treatments required, and functional impact of those affected. It reflects how the disease was affecting the subject’s daily functional activities. For example, mild cases of AD had limited involvement, requiring only topical therapy with infrequent flares, while moderate AD has more frequent intermittent flares. Severe cases of AD were those with extensive involvement, requiring systemic immunosuppressants and/or significant impact to function.
Odds ratio (OR), 95% confidence interval (CI), and p-values were calculated to test the null hypotheses of the association between the various comorbidities and risks of having moderate or severe AD compared with mild AD. In order to adjust for potential confounding, multivariate analysis was carried out, with a logistic regression model with the dependent binary outcome as developing moderate/severe AD and aforementioned confounding factors as the independent variables. Multicollinearity between the independent variables was assessed using the variation inflation factor (VIF). In view of multiple comorbidities of interest, Bonferroni correction adjustments were applied to p-values to address the issue of multiple testing. The Statistical Package for Social Sciences (IBM SPSS Version 22) was utilized to perform the analysis.
Fig. 1. Flow chart of study procedures.
This study received approval from the Singapore Armed Forces (SAF) Institutional Review Board, and a waiver of consent from participants was granted as the study was a retrospective chart review.
A total of 10,077 personnel had a diagnosis of AD and were included in this study. Baseline demographic information are summarized in Table I. The median age was 20 years. The majority of the study cohort were Chinese (85.2%), followed by Malays (7.3%) and Indians (4.9%). Among the study cohort, a total of 2,606 personnel (25.8%) were classified to have moderate-to-severe AD. Among those who had moderate-to-severe AD, 80.6% had moderate AD and 19.4% had severe AD (Table II).
Table I. Distribution of characteristics across atopic dermatitis (AD) cases
Table II. Association of comorbidities with moderate-to-severe atopic dermatitis
The median BMI of the cohort was 22.1 kg/m2. Metabolic conditions, such as hypertension, hyperlipidaemia and type 2 diabetes mellitus, were relatively uncommon, ranging from 0.3% to 2.8%. Close to a quarter (23.3%) of the cohort had a previous diagnosis of asthma, and 17.9% of the cohort had a previous diagnosis of allergic rhinitis. Known diagnoses of food allergies were uncommon (1.8%).
Increased BMI (overweight or obese), as well as hypertension, hyperlipidaemia, and type 2 diabetes mellitus (metabolic conditions) were significantly correlated with having moderate-to-severe AD. Those who were overweight (defined as BMI ≥ 23 kg/m2) (13) were more likely to have moderate-to-severe disease (OR: 1.23, 95% CI: 1.12–1.35, p < 0.001). Those who were obese (defined as BMI ≥ 27.5 kg/m2) (13) were even more likely to have moderate-to-severe AD (OR: 1.44, 95% CI: 1.28–1.63, p < 0.001). Those who had hypertension, hyperlipidaemia and/or type 2 diabetes mellitus were also significantly more likely to have moderate-to-severe AD (OR: ranging from 1.43 to 6.85). The presence of allergic rhinitis, asthma and food allergies (atopic conditions) were also associated with increased risk of having moderate-to-severe AD. Having allergic rhinitis and/or asthma was associated with 5.88-times higher risk of having moderate-to-severe AD compared with those with no atopic conditions (95% CI: 5.33–6.49, p < 0.001). Those with confirmed food allergies were associated with 1.83-times higher risk of having moderate-to-severe AD (95% CI: 1.36–2.47, p < 0.001).
Multivariate logistic regression was performed to adjust for confounding. Metabolic conditions, such as increased BMI, hypertension, hyperlipidaemia and type 2 diabetes mellitus, remained significantly associated with moderate-to-severe AD after adjustment for the various confounding factors and Bonferroni corrections (Table II). Having type 2 diabetes mellitus was the most strongly associated with an increased risk of moderate-to-severe AD among all the metabolic conditions (OR: 5.62, 95% CI: 2.15–14.6, p < 0.001). Atopic conditions (allergic rhinitis/asthma) were also significantly associated with an increased risk of moderate-to-severe AD (OR: 6.92, 95% CI: 6.21–7.72, p < 0.001). The association of food allergies with severity of AD was no longer positive or significant after adjustment for confounding factors. There was no evidence of multicollinearity between the independent variables included in the regression model (VIF ranged between 1.007 and 1.169).
The effect of having multiple metabolic conditions on the risk of having moderate-to-severe AD (Table III) was evaluated. While having one or more metabolic conditions gave a higher risk of having moderate-to-severe AD (OR 1.24; 95% CI: 1.12–1.37, p < 0.001), having 2 or more metabolic conditions gave an even higher risk of having a more severe AD (OR 1.88; 95% CI: 1.43–2.47, p < 0.001). This dose effect was also observed in individuals with 3 or more metabolic conditions. They have a 2.73-times risk of having moderate-to-severe AD, but this was not statistically significant after Bonferroni correction (95% CI: 1.04–7.12, p = 0.041, corrected p = 0.246).
Table III. Association of number of metabolic comorbidities with moderate-to-severe atopic dermatitis
A notable finding of this study was the significant association between metabolic comorbidities, such as hypertension, hyperlipidaemia and type 2 diabetes mellitus, and moderate-to-severe AD. A significant dose effect of more metabolic conditions conferred a higher risk of having moderate-to-severe AD. Moreover, the data also suggest a dose effect of increased BMI on severity of AD. This meant that individuals who were obese, compared with those who were overweight, had a further increased risk of having moderate-to-severe AD.
Proportionately, co-existing metabolic conditions in patients with AD were uncommon in our study population. This is not unexpected, given the young age of the study population. A study on hypertension in Singapore male conscripts with comparable demographics to the current study, found a prevalence of 1.6%, which was similar to our study findings of 1.7% (14).
These findings are consistent with local population studies (12), and since the prevalence of metabolic conditions are likely to increase with age, these findings have added relevance.
There have been reports of a positive association between BMI and AD in adolescents (15, 16), but these results were not stratified according to severity of AD. The evidence of the association of cardiovascular risk factors and adult AD also remains controversial. A positive association was found in 1 US study (3), but an Asian AD cohort in Taiwan found a significantly increased risk of ischaemic stroke only (17) and 2 recent studies reported no association of hypertension and type 2 diabetes with AD (18, 19). A recent systematic and meta-analysis review by Ascott et al. reported that significant associations with cardiovascular outcomes were more common in cohort studies, but no evidence was found among cross-sectional studies (20). Anderson et al. suggested that these conflicting findings on cardio-metabolic risk in adults with AD in a general population may also be attributed to the heterogeneity of AD classifications in the study populations (21). One systematic review and meta-analysis has suggested that, while adult patients with AD may have an increased prevalence of some disease risk factors, such as obesity and smoking, AD is unlikely to be an independent risk factor for cardiometabolic disease (9). The prevalence rates of these cardiometabolic disease risk factors were also lower in patients with AD compared with those with psoriasis (22). Some authors have proposed that any observed associations between AD and cardiovascular diseases might have been confounded by poor health behaviours of patients with AD, such as smoking, reduced physical activity and drinking alcohol (20). It must be pointed out that these large population cohort or database studies may not always take into account the severity of AD in their analyses. However, a recent review found that increasing severity of atopic eczema was associated with increased risk of cardiovascular outcomes (21).
These findings, however, are consistent with a recent report that showed a biochemical correlation of moderate-to-severe AD with systemic inflammation (23). In adult patients with AD, it has also been found that there is an increased coronary artery calcium score in the cardiac computed tomography angiography of the coronary tree (24). This might suggest that, in individuals with poorly controlled or severe disease, there is a considerable level of inflammatory burden from the skin. These patients may require tighter control of their metabolic conditions, which forms an important component in the holistic management of chronic adult AD.
Atopic conditions were significant risk factors for moderate-to-severe AD in our study population. This is consistent with a study by Thijs et al. (25), who reported that the clinical endotype of adult AD associated with co-existent atopic conditions was associated with more severe and extensive AD. This endotype also correlated with the highest levels of serum mediators, such as PARC, TIMP-1 and sCD14, and a predominantly Th-2 cytokine profile. The observed association of atopic conditions with a more severe clinical phenotype of AD is parallel with findings that severe AD is associated with persistence of asthma into adulthood. The atopic march phenomenon describes a common pathomechanism of the development of AD at a young age with that of other atopic conditions later on; hence, this may explain the higher OR between atopic conditions and severity, compared with metabolic conditions (26). Interestingly, the association with atopic conditions was also found to significantly lower the remission rate compared with patients without concomitant allergic conditions (27). However, it remains to be determined whether control of the associated atopic manifestations leads to an improvement in AD. We believe that the chronic immune-activated state of atopic conditions potentially affects the inflammatory pathways of AD. However, these risk associations may represent epiphenomena; hence, further prospective large-scale studies are required. Nonetheless, we believe that, in the group of adult patients with AD with severe chronic disease, more resources are required to regularly screen for the aforementioned conditions and to actively manage their comorbidities.
To the best of our knowledge, this is the first study to evaluate the association of comorbidities with the severity of AD. The strength of this study is the large sample size, consisting of a national population cohort of more than 10,000 subjects. The validity of the results is further reinforced by mandatory nature of health screening in the population; with almost no missing data from existing electronic medical records. This is in contrast with a questionnaire-based study, which may have reporting or recall bias. Based on local studies of AD in earlier epidemiological studies in Singapore (28, 29), the sex ratio of AD was found to be equal, hence our results may be extrapolated to the overall young adults of our local population.
However, limitations of our study would be that any correlations made in the study are subjected to possible reverse causation given the retrospective nature of the study and potential non-differential misclassification from the diagnostic codes. Validated severity AD scoring scales, such as SCORing Atopic Dermatitis (SCORAD) and Eczema Area and Severity Index (EASI), were not available in the EMR; instead it utilized a global severity classification that was meant to serve a clinical and functional purpose. There is also potential surveillance bias, as patients with severe AD or comorbidities may receive more frequent medical attention. Duration of AD was not captured in the system, and certain known risk factors of adult AD, such as environmental risk factors (e.g. dietary, smoking, exercise and other lifestyle habits) as well as family history of AD and atopy, were not present in the military EMR.
In conclusion, this study has demonstrated the significant relationship of comorbidities with the severity of adult AD. While large-scale longitudinal studies are required to address the relationship of these comorbidities and AD, this represents a step in building our understanding of the associations with the more severe form of AD in adults. Mitigating strategies in order to screen, detect and treat metabolic and atopic conditions are therefore important to reduce the overall disease burden of chronic adult AD.
The authors acknowledge the contribution of Ms Janet Lim from Headquarters Medical Corps, Singapore Armed Forces towards data extraction. The contents of this paper do not represent the policy or stand of the Ministry of Defence, Singapore or the Singapore Armed Forces.
Ethics. This study was granted exemption from the Singapore Armed Forces Institution Review Board.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize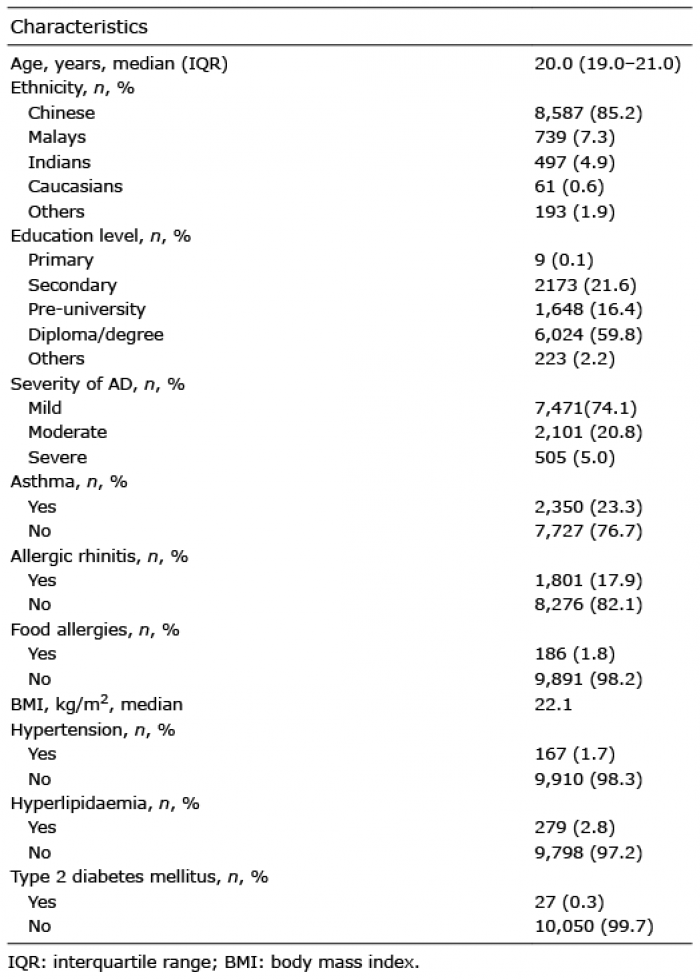 Click to show fullsize
Click to show fullsize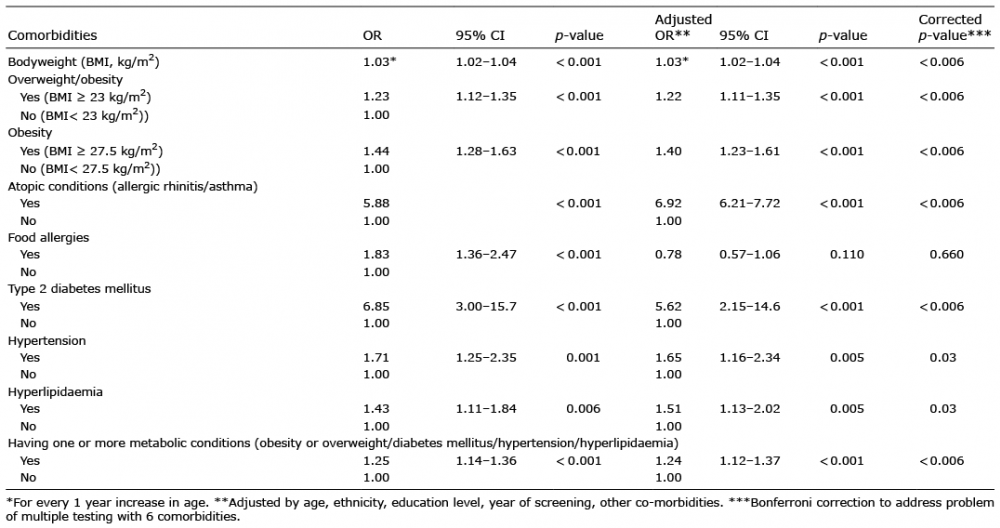 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize