


Department of Dermatology and Plastic Surgery, Akita University Graduate School of Medicine, 1-1-1 Hondo, Akita 010-8543, Japan. E-mail: chiba-t@gipc.akita-u.ac.jp
Accepted Apr 30, 2019; E-published May 2, 2019
The effect of anti-interleukin (IL)-4/-13 treatment, dupilumab, on allergic diseases and the resulting various unexpected phenomena have been reported in the literature. The clinical features of mycosis fungoides (MF) with multiple erythematous lesions are similar to those of atopic dermatitis (AD). Thus, anti-IL-4/-13 therapy may be erroneously administered to patients with MF with features similar to those of AD. This report is the first to describe a case of MF diagnosed after administration of dupilumab for AD.
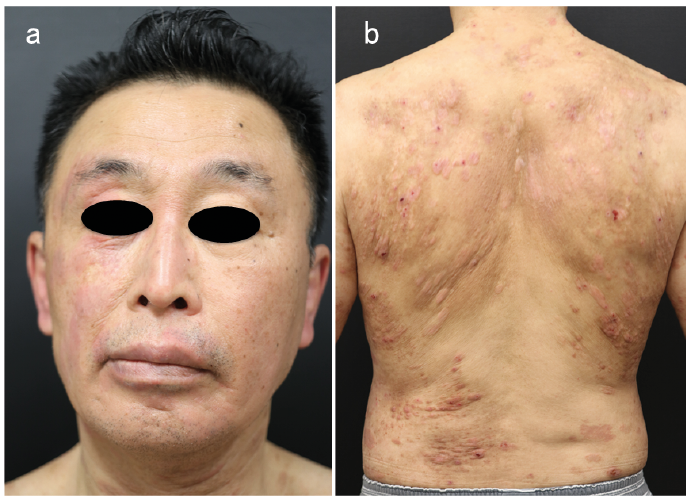
A 58-year-old man had had AD since early childhood. Although remission had occurred in adolescence, eczema had appeared on his trunk and limbs at the age of 47 years. He presented to a dermatologist and was administered topical corticosteroid ointment, betamethasone butyrate propionate, based on the diagnosis of recurrent AD. In 2013 the patient was referred to our university for treatment of a carcinoma of the maxillary sinus using chemoradiotherapy. Treatment was successful. Subsequently, the patient continued treatment for AD in our department. The cutaneous eruption was somewhat controlled by topical treatments; however, at times he experienced intense itching (Fig. 1). He reported a history of allergic rhinitis, conjunctivitis and asthma. Given the severity of his AD, treatment with dupilumab 600 mg, subcutaneously was initiated on the first day, followed by 300 mg every 2 weeks in 2018. Serum examination prior to administration revealed elevated levels of thymus-and activation-regulated chemokine (TARC, 4,634 pg/ml; normal range: < 450 pg/ml), IgE (1,280 IU/ml; normal range: < 250 IU/ml), and lactate dehydrogenase (LDH, 269 U/l; normal range: 124–224 U/l). The eosinophil count was within normal limits. The Eczema Area and Severity Index (EASI) was 34.4, while the Dermatology Life Quality Index (DLQI) was 8. During treatment with dupilumab, the faint erythematous lesions on the face and trunk became more obvious, despite continuous application of the topical steroid (Fig. 2). After 1 month, the EASI and DLQI were slightly decreased (29 and 6, respectively); however, there was no improvement in pruritic symptoms. Laboratory tests revealed that TARC, IgE, and LDH levels were 3,948 pg/ml, 924 IU/ml, and 287 U/l, respectively. Owing to exacerbation of the ery-thematous lesions, skin biopsy of the erythematous macule on the trunk was performed. Histopathology showed band-like atypical lymphocytic infiltration into the dermis. Atypical epidermotropic lymphocytes without spongiosis were observed in the epidermis, which formed Pautrier’s microabscess (Fig. 3). Almost all of these infiltrated lymphocytes were positive for CD3 and CD4. There was clonal rearrangement of T-cell receptors. Computed tomography scan revealed no lymphadenopathy. Based on these findings, the patient was diagnosed with MF. Dupilumab was discontinued, and topical treatment with steroid is being administered to the patient in addition to initiating narrow-band ultraviolet B therapy.
Fig. 1. (a) Erythematous lesions on the face. (b) Poikiloderma lesions accompanied by papules and nodules on the back. Written permission from the patient is given to publish these photos.
Fig. 2. (a) Face and (b) back after 1 month of treatment with dupilumab. Written permission from the patient is given to publish these photos.
Fig. 3. Histopathology of the biopsy specimen from the erythematous lesion on the chest shows lymphocytic infiltrate in the dermis with prominent epidermotropism (a: haematoxylin and eosin; H&E ×100) and atypical lymphocytes into the epidermis (b: H&E ×400).
This report describes a case of MF that was misdiagnosed as AD following administration of dupilumab. MF is the most common type of cutaneous lymphoma originating from T cells (1). Typically, skin lesions of MF are well-defined erythematous lesions without itching; however, it is occasionally difficult to clinically differentiate between MF and AD. In addition, coexistence of MF and AD in the same patient has been reported in several studies (2, 3). Because the prognosis of MF differs from that of AD, it is important to differentiate these conditions.
Dupilumab, a human monoclonal antibody for IL-4 and IL-13 receptors sharing the α subunit of the IL-4 receptor, was approved in Japan in 2018 (4). It is expected to be more effective than conventional treatments with no severe side-effects for treatment of moderate-to-severe atopic dermatitis (5). Dupilumab may be considered as a prospective treatment option for IL-4 and IL-13-related allergic diseases, such as asthma. Furthermore, some curative effects were reported for bullous pemphigoid and alopecia areata (6, 7). To the best of our knowledge, this is the first case of MF becoming apparent in a patient with AD who was treated with dupilumab. Dupilumab therapy did not alleviate AD symptoms in this patient, but induced a flare-up of the cutaneous lesions. This sign provided a clue about the presence of MF.
MF is considered as a T-helper (Th) 2-related disease, occasionally inducing eosinophilia and increase in IgE, as seen in AD. The Th1 and Th2 immuno-balance in the skin microenvironment of MF is altered due to the disease stage. The tumour cells in the lesional skin of tumour-stage shift to a Th2 phenotype, which is characterized by production of IL-4, IL-5, IL-10 and IL-13 (8, 9). On the other hand, a polarized Th-2 cytokine pattern was not demonstrated among cultured skin-infiltrating non-malignant T cells isolated from early MF (10). Otherwise, lesional T cells and peripheral blood T cells in the early stage of MF showed a Th1 cytokine pattern by increasing expression of interferon (IFN)-γ, (11). In the initial stage of MF, a Th1 dominance might be a beneficial response for patients because IFN-γ interferes with tumour cells and stops them from growing and multiplying. It also stimulates the immune system by triggering killer T cells to attack tumour cells. Thus, dupilumab could enhance the Th1 response and reveal an anti-tumour effect; however, erythema exacerbated in the current case. The use of antagonist for the IL-4 and IL-13 receptors at the patch stage of MF may promote tumour progression. The biological effect of IL-4/13 antagonist for the microenvironment of MF warrants future investigation. We have reported here a case of MF that was misdiagnosed as AD. Once again, the differential diagnosis between severe AD and early MF is often difficult and it should be borne in mind that adult-onset AD is often found to be MF or Sézary syndrome.


 Click to show fullsize
Click to show fullsize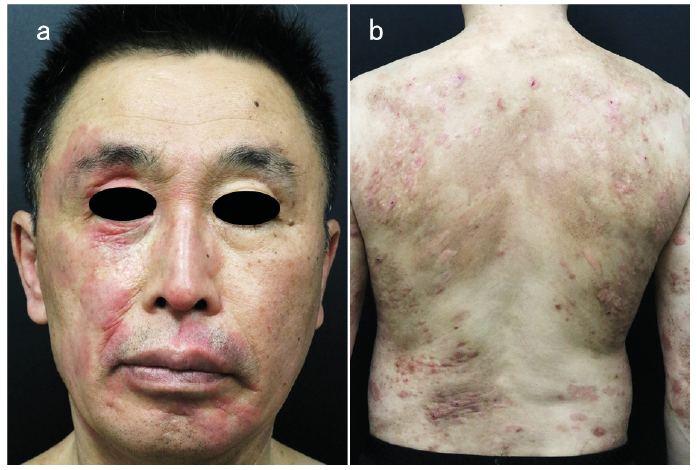 Click to show fullsize
Click to show fullsize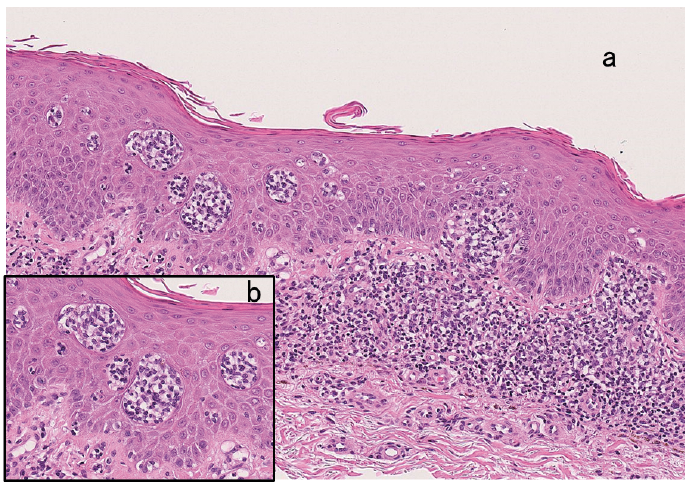 Click to show fullsize
Click to show fullsize