


Department of Dermatology, Iwate Medical University, Uchimaru 19-1, Morioka 020-8505, Japan. *E-mail: ayawata@iwate-med.ac.jp and hamano@iwate-med.ac.jp
Accepted Apr 30, 2019; E-published May 2, 2019
Extramammary Paget’s disease (EMPD) is a rare intraepithelial malignant tumour that arises mostly in the epidermis of areas where apocrine glands are distributed, i.e. mainly in the anogenital and axillary skin. In general, the prognosis of EMPD is good when the tumour cells are limited to the epidermis, but poor when they invade the dermis and metastasize to lymph nodes or other organs. Nodal metastasis is reportedly one of the most important prognostic factors in EMPD (1). On the other hand, brain metastasis from EMPD is very rare, and there have been no reports of meningeal carcinomatosis (MC) from EMPD.
We report here a rare case of MC in advanced EMPD due to bone metastasis and discuss the features of brain metastasis from EMPD. If cognitive impairment and dementia-like disorientation occur suddenly, MC and brain metastasis should be suspected, and magnetic resonance imaging (MRI) examination should be conducted.
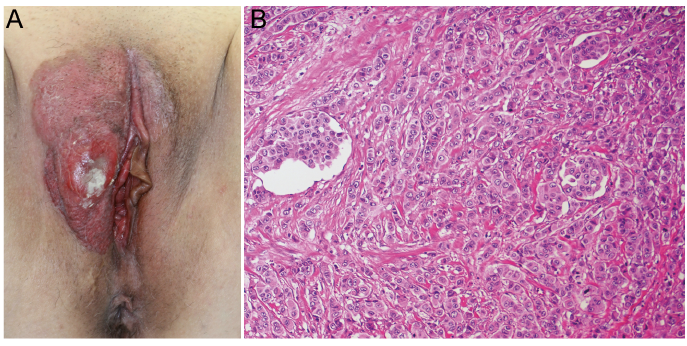
A 65-year-old woman visited our hospital because of genital bleeding and bilateral leg oedema. She had a medical history of spinal column stenosis and appendicitis. Physical examination revealed indurated erythema on both labia majora, accompanied by an ulcerative tumour on the right labium majorum (Fig. 1A). Right inguinal lymph node enlargement was evident, and a skin biopsy of the tumour yielded a diagnosis of EMPD. Positron emission tomography (PET) demonstrated 18F-fluorodeoxyglucose (FDG) uptake in multiple lymph nodes and sagittal T2-weighted MRI revealed high signal intensity in the L4 vertebral bone (Fig 2A). The genital tumour was resected palliatively. Histopathological examination demonstrated that Paget cells had proliferated in the epidermis and dermis, and had also invaded lymph vessels (Fig. 1B). Docetaxel monotherapy was administered monthly at a dose of 60 mg/m2. After 3 cycles, the nodal disease disappeared on PET images and the high signal intensity in the L4 vertebral bone was reduced. After 5 cycles, gadolinium-enhanced T1-weighted MRI revealed multiple small spots in the brain, suggesting metastases of EMPD to the central nervous system (CNS) (Fig. 2B). We performed 30 Gy of cranial irradiation in 10 fractions. This reduced the brain metastases, but the patient developed nausea, vomiting and gait disturbance, followed gradually by memory impairment and trunk dystonia. Gadolinium-enhanced T1-weighted MRI demonstrated enhancement along the cerebellar sulcus of the brain (Fig. 2C). For diagnosis, lumbar puncture was performed, and analysis of the cerebrospinal fluid (CSF) revealed an increased WBC count and an elevated CSF protein level. Cytopathological examination confirmed the diagnosis of MC from EMPD (Fig. 3). Disturbance of consciousness gradually progressed, and the patient died approximately one month after diagnosis of MC.
Fig. 1. (A) Physical examination of the Extramammary Paget’s disease (EMPD) lesion on both labia majora with indurated erythema and an ulcerative tumour on the right labium majorum. (B) Paget cells had infiltrated the epidermis and dermis, and the tumour cells also invaded the lymph vessels (haematoxylin-eosin (HE), original magnification ×200).
Fig. 2. Magnetic resonance imaging (MRI) image. (A) Sagittal T2-weighted MRI revealed an axial bone metastasis in the L4 vertebra. (B) Gadolinium-enhanced T1-weighted MRI revealed multiple metastatic lesions in the brain. (C) Gadolinium-enhanced T1-weighted MRI revealed enhancement along the cerebellar sulcus of the brain.
Fig. 3. Cytopathological examination revealed atypical cells with a high N/C ratio, unevenly distributed nuclei, and containing a mucus-like substance. (A) Giemsa stain (original magnification ×400). (B) Papanicolaou stain (original magnification ×400).
EMPD is a malignant neoplasm arising from apocrine sweat glands, such as those in the anogenital and axillary regions. The most common pattern of EMPD metastatic spread is via the lymphatic system or intra-epithelial infiltration. The prognosis of EMPD is favourable if diagnosis and treatment are started early, but poor if distant metastases are present. Nodal metastasis is reportedly one of the most important prognostic factors in EMPD (1). To our knowledge, only a few cases of EMPD with brain metastases have been reported (2, 3), and meningeal carcinomatosis (MC) from EMPD has not been documented previously.
Meningeal carcinomatosis is multifocal seeding of the leptomeninges by malignant cells, such as breast cancer, small cell lung cancer (SCLC) and melanoma, and is characterized by diffuse invasion of the meninges and cerebrospinal fluid.
MC presents with signs and symptoms of multifocal neuraxis disease, such as headache, nausea, vomiting, cranial nerve palsies and cognitive impairment (4). Our patient suddenly developed dementia-like disorientation. The gold standard for diagnosis of MC is CSF examination via lumbar puncture. Initial CSF cytology is positive in 50% of cases and repeated spinal fluid analysis up to a maximum of 3 times yields up to 90% positive cytology (5, 6). In cases that are cytology-negative, but clinically suspicious, an elevated CSF opening pressure, the CSF protein level, a high CSF WBC count, and a low CSF glucose level can support a diagnosis of MC. Notably, MRI is also effective for MC diagnosis in 83–85% of patients with solid tumours. The most common features revealed by MRI are pial enhancement and nodularity, along with nodular disease, neural enhancement, and white matter changes (7).
In breast carcinoma, there are several routes that carcinoma cells can potentially take to involve the meninges. Such involvement can follow metastasis to: (i) the meninges, (ii) brain parenchyma, (iii) axial bones, (iv) choroid plexus, or (v) cranial nerves (8). Most cases of EMPD brain metastasis show disseminated lesions, resulting mainly from intraspinal axial bone metastasis. In the present case, we determined the routes of brain metastasis from EMPD.
Therefore, in patients with bone metastasis of EMPD, it is necessary to be mindful of the possible onset of MC and brain metastasis. If cognitive impairment and dementia-like disorientation occur suddenly, MC and brain metastasis should be suspected, and MRI examination should be conducted. Treatment options for MC include intrathecal chemotherapy, systemic chemotherapy and radiation therapy, but no standard treatment for MC has yet been established. Furthermore, no definitive guidelines are available for management of brain metastasis from EMPD because the blood-brain barrier is a complicating factor. In this context, effective treatment is limited to radiation therapy (2, 3).
The human epidermal growth factor receptor 2 (HER2) protein is often overexpressed in EMPD. Trastuzumab, a humanized monoclonal antibody against HER2, is useful for the treatment of advanced EMPD overexpressing HER2 protein, but ineffective against the brain metastasis (2). Lapatinib, a dual HER1/HER2 tyrosine kinase inhibitor, can theoretically penetrate the blood-brain barrier. In breast cancer, patients treated with both trastuzumab and lapatinib after developing brain metastases reportedly have a significantly longer survival period than those who receive either a single or no HER2-targeting agent (9). Therefore, as is the case for breast cancer, treatment that can penetrate the blood-brain barrier may be effective for MC and brain metastasis from EMPD; however, this approach is not yet permitted in Japan.
We have described a case of advanced EMPD that developed into MC and brain metastasis. This is the first reported case of MC from EMPD that was diagnosed on the basis of CSF cytology and MRI. Effective treatments for management of MC and brain metastasis from EMPD remain to be explored.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize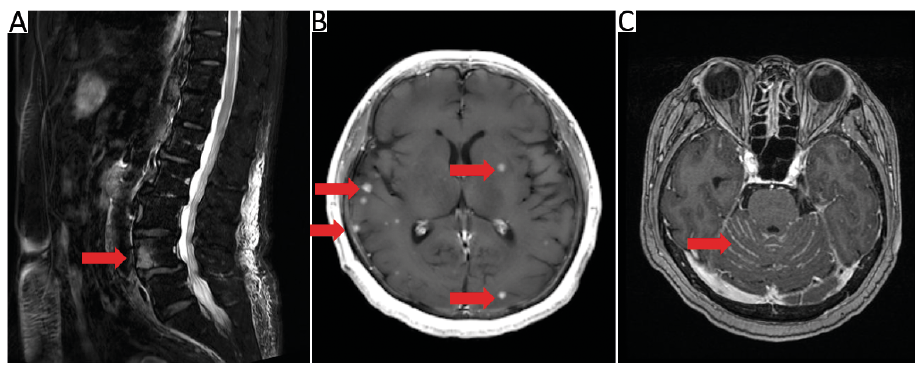 Click to show fullsize
Click to show fullsize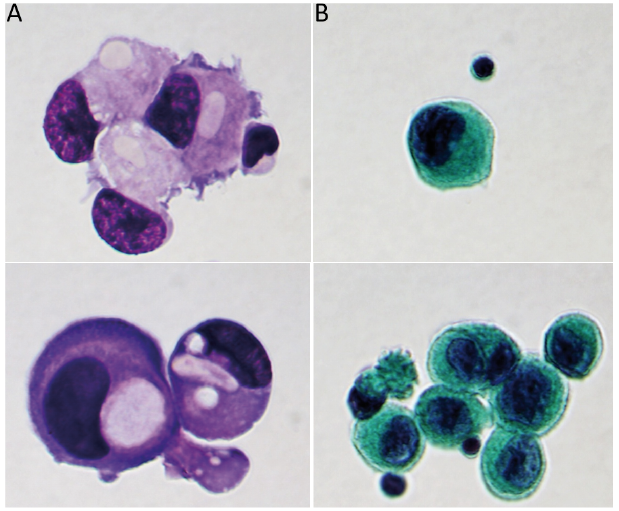 Click to show fullsize
Click to show fullsize