


Department of Dermatology, Venereology and Allergology, University Medical Center, Ruprecht-Karls-University, Im Neuenheimer Feld 440, DE-69120 Heidelberg, Germany. E-mail: ferdinand.toberer@med.uni-heidelberg.de
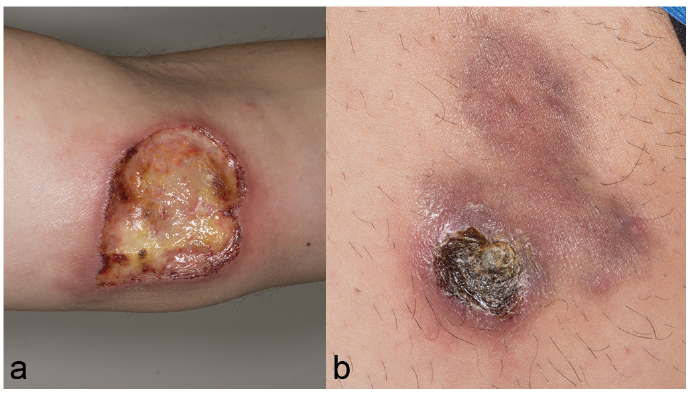
A 36-year-old man presented with a 10-month history of painless ulceronecrotic lesions on his left upper arm and right thigh. Clinical examination revealed an ulceration measuring 4×4 cm, with a fibrinous base, crust-covered borders and a surrounding livid erythema, on his left upper arm (Fig. 1a). The right thigh showed a necrotic papule covered by a brownish crust (Fig. 1b). The patient had familial Mediterranean fever (homozygous M694V mutation), which was treated with colchicine (1.5 mg/day). Laboratory analysis, including blood count, metabolic panel, hepatitis B/C, EBV and HIV serologies, was unremarkable. C-reactive protein values (34.8 mg/l) and erythrocyte sedimentation rate (32 mm/1st h) were slightly elevated. A skin biopsy from the arm was performed and revealed a dense dermal infiltrate composed of histiocytes, lymphocytes, multinucleated giant cells, plasma cells and neutrophils, forming tuberculoid and suppurative granulomas (Fig. 2). Focally, vessels showed signs of luminal obliteration and vasculitis.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical picture. (a) Left upper arm. (b) Right thigh.
Fig. 2. Section of biopsy from the arm, showing a mixed dermal infiltrate forming granulomas (haematoxylin-eosin stain; original magnification ×100).
Acta Derm Venereol 2019; XX: XX–XX.
Diagnosis: Lues maligna (malignant syphilis)
Immunohistochemical staining for Treponema pallidum showed fine spirochetes (Fig. 3). The histological diagnosis of lues was confirmed by serum investigation, which showed a titre of rapid plasma reagin (RPR) (1:64) and T. pallidum particle agglutination (TPPA) (1:81920). Syphilis immunoglobulin G/M was positive on immunoblot assay. The patient was treated with benzathinepenicillin, 2.4 million units weekly, intramuscularly, for 3 weeks. The lesions healed completely leaving residual poikilodermatic scars.
Lues maligna (LM), also referred to as malignant syphilis or ulceronodular syphilis, is a rare atypical variant of secondary syphilis, usually occurring in immunosuppressed patients, mainly those with HIV infection (1, 2). Immunodeficiency caused by HIV may favour the predominance of the agent’s virulence in the agent-host-contest (1). Malnutrition, alcohol abuse, diabetes, intravenous drug use and concomitant debilitating disorders are also reported as predisposing factors for LM (1, 3–5). Nevertheless, few cases are described in immunocompetent patients (1, 3, 4). Clinically, LM is characterized by polymorphous, mostly disseminated, papulonodular and ulcerated cutaneous lesions, frequently covered by rupioid crusts (3). Associated systemic symptoms (fever, malaise, and arthralgia) are common, but not a diagnostic prerequisite (3).
In the HIV uninfected population LM is rarely described, and only 14 cases are on record prior to 1988, the year in which the first case of LM in a HIV-infected patient was reported (6–8). From 1989 to 1994, an additional 12 cases were reported (6). Eleven of these 12 patients were either HIV-positive or at high risk for HIV infection (6). These findings underline the association of LM with HIV.
LM, as secondary syphilis in general, often acts as “great mimicker” and should be considered as a differential diagnosis in multiple clinical settings, both in immunosuppressed and immunocompetent populations (8). LM eruptions have been reported to mimic malignant (cutaneous T-cell lymphoma), infectious (fungal, bacterial and mycobacterial infections) and inflammatory (pityriasis lichenoides et varioliformis acuta, necrotizing vasculitis, pustular psoriasis, erythema exudativum, sarcoidosis) dermatoses (1, 5).
The patient described here had familial Mediterranean fever (FMF), a rare autosomal recessive autoinflammatory disease characterized by paroxysmal fever, peritonitis, arthritis and myalgia (9). A variety of cutaneous lesions occurring in patients with FMF have been described including urticaria, angioneurotic oedema, non-specific purpura, “erysipelas-like erythema”, subcutaneous nodules, cutaneous vasculitis and Raynaud’s phenomenon (9). We considered the possibility of cutaneous eruptions associated with FMF in the present case; nevertheless, ulcero-necrotic lesions do not belong to the spectrum of skin lesions associated with FMF. Pyoderma gangrenosum was also considered as potential differential diagnosis, but the lesions were not painful and the histopathological findings did not support this diagnosis. From a clinical point of view, systemic vasculitis (such as periarteritis nodosa) and calciphylaxia may also be considered as a differential diagnosis if LM lesions reveal a livedoid aspect.
In conclusion, LM is rare in immunocompetent patients, and the present case will contribute to an expanded pool of evidence. Whenever confronted with ulcero-necrotic lesions dermatologists should consider LM as differential diagnosis, even in not immunosuppressed patients and in the absence of systemic symptoms. Increased awareness of this rare manifestation of secondary syphilis will help to avoid delay in diagnosis and treatment.
Fig. 3. Immunohistochemical stain showing fine spirochetes (original magnification ×400).


 Click to show fullsize
Click to show fullsize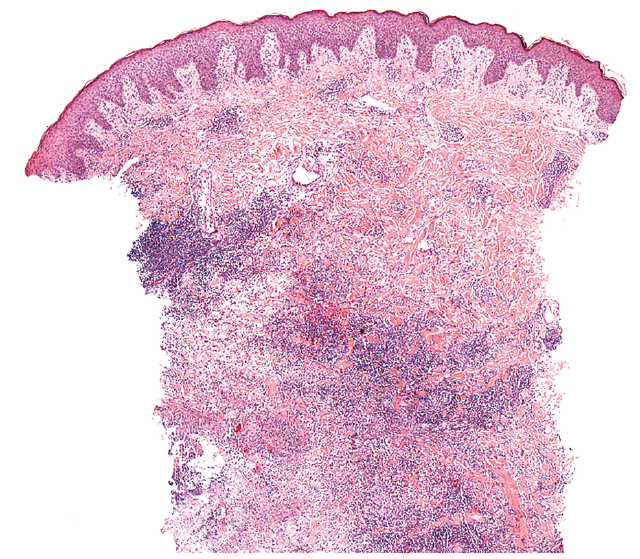 Click to show fullsize
Click to show fullsize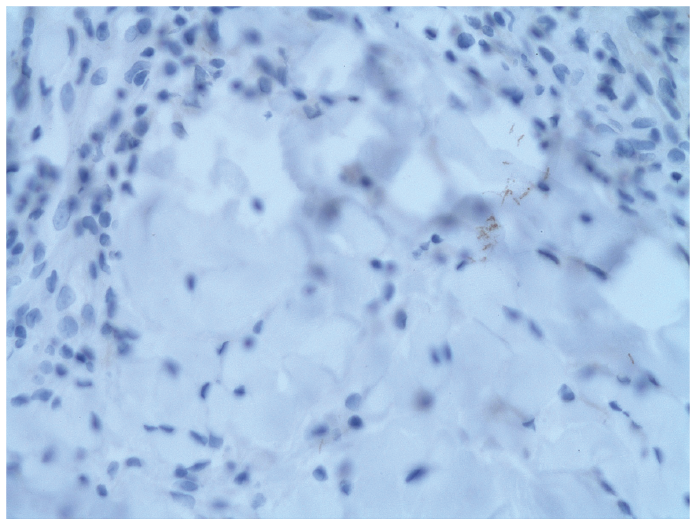 Click to show fullsize
Click to show fullsize