


Department of Dermatology, University Hospital Dresden, DE-01307 Dresden, Germany. E-mail: stefanie.heyne@uniklinikum-dresden.de
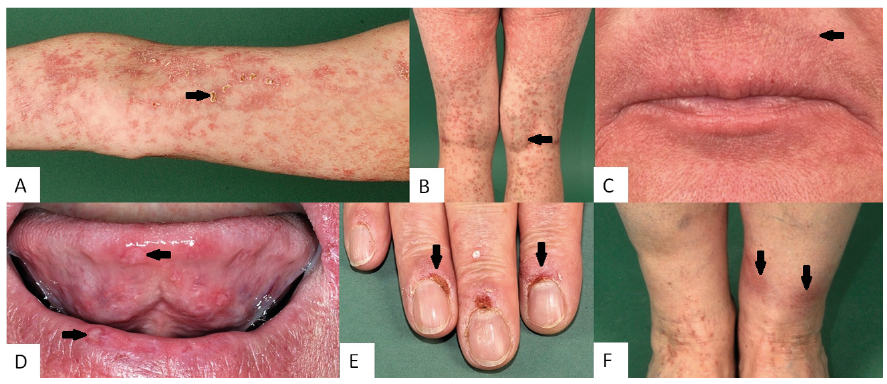
A 63-year-old woman presented with a 6-year history of a cutaneous eruption in a distinctive linear and reticular pattern. Hyperkeratotic dark erythematous papules with fine white scaling were spread mainly on the interior sides of her arms (Fig. 1A) and legs (Fig. 1B). Erythema and scaling was present on the perioral region (Fig. 1C). In addition, she had painful oral ulcers on the mucosal lips, buccal mucosa and tongue (Fig. 1D). Periungual erythema and swelling was present on the fingers (Fig. 1E). She had tender, erythematous subcutaneous nodules on the lower legs (Fig. 1F).
Skin biopsy from the linear hyperkeratotic plaques demonstrated a partially acanthotic and atrophic epidermis with parakeratosis, dyskeratosis and an underlying lichenoid interface dermatitis. The dermal infiltrate mainly contained lymphocytes and histiocytes (Fig. 2)
The patient had a history of signs reminiscent of sarcoidosis in the lung. Bilateral hilar shadowing was detected on X-ray 5 years previously. Treatment with methotrexate for 2 years led to complete regression of pulmonary infiltration. The cutaneous symptoms were not significantly ameliorated.
What is your diagnosis? See next page for answer.
Fig. 1. Erythematous papules with fine white scaling on: (A) arms and (B) legs. (C) Perioral erythema, (D) oral ulcers, (E) periungual erythema and swelling, and (F) erythematous subcutaneous nodules on the lower legs.
Fig. 2. Histology of skin biopsy: acanthotic and atrophic epidermis with parakeratosis (⇒), dyskeratosis (←) and an underlying lichenoid interface dermatitis (⬆), dermal infiltrate (⇩) mainly contained lymphocytes and histiocytes (HE staining ×100).
Acta Derm Venereol 2019; XX: XX–XX.
Diagnosis: Keratosis lichenoides chronica in combination with sarcoidosis.
Keratosis lichenoides chronica, also called Nekam’s disease, is a rare chronic progressive mucocutaneous disease. It was first described by Kaposi in 1895 as “lichen ruber moniliformis” (1). Nekam reassessed this case in 1938 and called the disease “Poroceratosis striate lichen” (2). Margolis et al. called it “Keratosis lichenoides chronica” in 1972 (3). The disease is characterized by hyperkeratotic, pruritic purple papules and plaques arranged symmetrically in a linear or reticular pattern. The lesions mainly occur on the face, extremities and trunk (4). Mucocutaneous or genital aphthous ulceration can accompany the cutaneous disease in half of the patients. Further symptoms are keratoconjunctivitis, uveitis or laryngitis (5). In approximately one-third of patients hyperkeratotic nail folds and periungual erythema can be observed (6–8). Every second patient additionally presents with palmoplantar keratoderma. As demonstrated in the current case, 75% of patients develop a perioral scaly erythematous inflammation reminiscent of rosacea or seborrhoeic-like dermatitis (6, 8). The aetiology of keratosis lichenoides is not known. It mainly manifests at between 20 and 50 years of age, with a slight preponderance in males (1.35:1) (6). The histological picture is characterized by a lichenoid reaction pattern combined with acanthosis, orthohyperkeratosis, and parakeratosis of the epidermis (3, 4).
Response to treatment is often limited. The case reported here received one cycle of ultraviolet A (UVA) irradiation upon topical application of methoxsalen. This therapy resulted in partial remission for the subsequent years (Fig. 3).
This therapeutic response is in line with literature describing effectivity of psoralen plus UVA (PUVA) or PUVA bath therapy (7, 9–11). If this is not sufficient patients can be treated with retinoids, such as acitretin with an initial dose of 0.5 mg/kg body weight/day (5). A combination of PUVA therapy and retinoids can also be used (8, 11, 12). One case also reported successful treatment with efalizumab (13).
There is one other report of erythematous subcutaneous nodules on the lower legs and pulmonary sarcoidosis associated with keratosis lichenoides chronica (14). There is currently no pathophysiological explanation for this coincidence. However, keratosis lichenoides chronica could be a reactive inflammatory skin disease following chronic immune stimulation.
Fig. 3. Partial remission of symptoms after ultraviolet A (UVA) irradiation with topical methoxsalen.


 Click to show fullsize
Click to show fullsize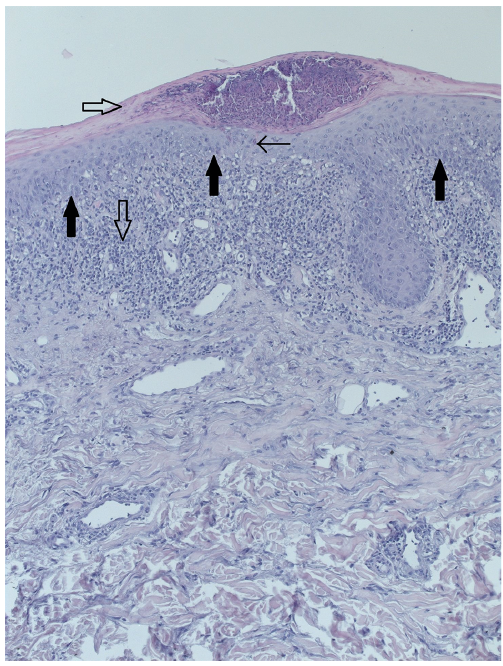 Click to show fullsize
Click to show fullsize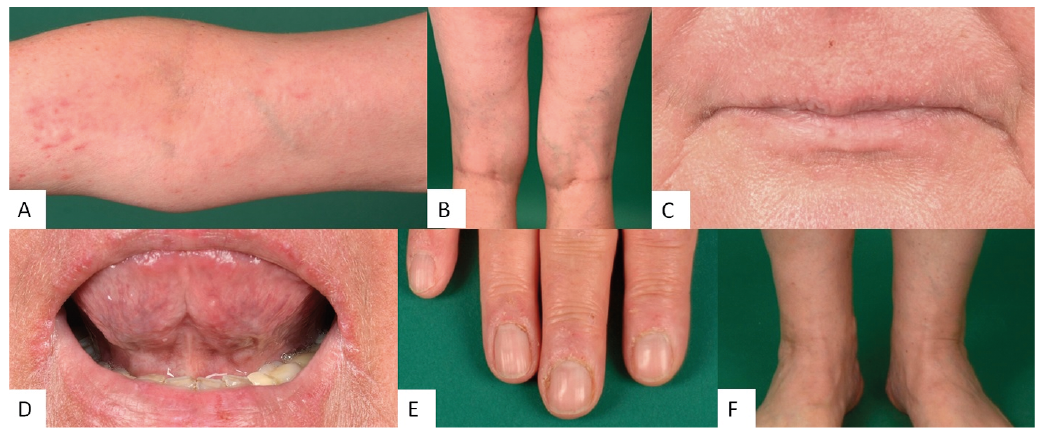 Click to show fullsize
Click to show fullsize