


1Dermatology Unit, and 3Pathology Unit, François Mitterrand Hospital, 4 boulevard Hauterive, FR-64000 Pau, 2Dermatology Unit, Saint Andre Hospital, CHU Bordeaux, and 4Radiation Unit, Pau, France. *E-mail: thomas.jouary@ch-pau.fr
Accepted Jul 9, 2019; E-published Jul 10, 2019
In some patients, radiotherapy causes onset of a new dermatitis or reactivation of a previously existent dermatitis. Radiation-induced lichen planus (LP) is a rare disorder; only a few cases have been described. We reported here a first case of bullous lichen planus triggered by radiotherapy.
An 82-year-old woman presented with a skin disorder with a severe bullous eruption localized in genital and gluteal friction areas. LP had been diagnosed one year earlier. Topical corticosteroids achieved good remission of the skin disease. While the LP worsened with onset of bullous lesions, a short-term oral corticosteroid therapy was initiated. The disease was in complete remission within 2 months. The corticosteroids were then tapered and stopped without recurrence of the LP. Four months later the patient developed breast cancer with bone metastases in the pelvic area. The patient declined systemic chemotherapy. When the bone metastases became painful, radiation beam therapy was initiated. The patient received 30 Gy, as 10 sessions of 3 Gy each. A bullous and painful dermatosis, localized to the pelvic and genital areas, appeared after 4 courses of radiation.
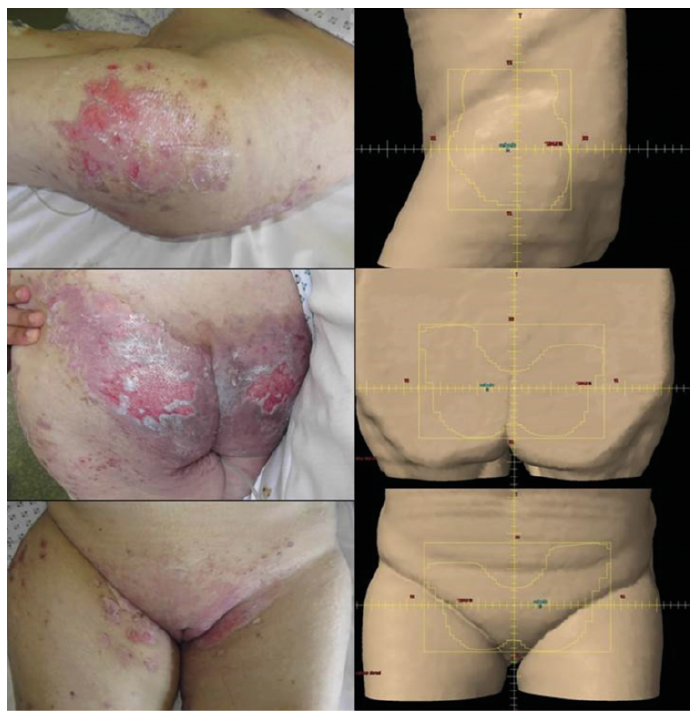
On examination, the patient had a poor performance status of 3 and pain localized to the pelvic skin areas. The skin lesions were plaques composed of coalescent violaceous papules with superficial and painful erosions (Fig. 1). Sampling for bacterial, fungal and viral (herpes simplex PCR) infection were negative. Pathological examination of a skin biopsy showed dyskeratotic hyperkeratosis, acanthosis, vacuolar alteration of the basal layer and presence of bandlike inflammatory cell infiltrate at the dermo-epidermal junction, consistent with a diagnosis of bullous LP (Fig. 2). Direct skin immunofluorescence and specific bullous pemphigoid antigens were negative. The dermatitis location was confined to the radiation fields (Fig. 1). The diagnosis of bullous LP triggered by radiation beam therapy was retained and a 1 mg/kg/day systemic corticosteroid therapy was initiated. The skin disorder rapidly improved in 2 weeks. Systemic corticosteroids were stopped after 3 months and remission was ongoing at 6 months.
Fig. 1. Bullous lichen planus located on the radiation therapy fields.
Fig. 2. Histology of a skin lesion with hyperkeratosis, vacuolar alteration of the basal layer and superficial bandlike infiltrate of lymphocytes and eosinophils (original magnification ×40).
Radiation beam therapy may cause various skin reactions. The most frequent adverse effect of radiotherapy is acute radiation-induced dermatitis. Radiation may cause the onset of a new dermatosis, named isoradiotopic effect by Shurman et al. (1) in 2004. Bullous pemphigoid and pemphigus are the most frequent isoradiotopic dermatoses. LP has been reported in association with radiation treatment in 15 patients since 2002 (1–6). LP may occur as an isoradiotopic response or as an isomorphic response, i.e. Koebner phenomenon. Radiation-induced LP occurred more frequently in patients with no history of previous LP. The lesions developed quickly after the start of radiotherapy and healed with topical steroids in most cases. The present case is considered as an isomorphic response with recurrence of a previous dermatosis at a site of local irritation and inflammation caused by radiation therapy. Indeed, the LP was present before the onset of radiotherapy. Interestingly, bullous LP recurred shortly after the onset of radiotherapy, with lesions confined to the radiation therapy fields. Patho-physiology of radiation-induced LP is poorly understood. Some authors have suggested that the radiation-induced skin injury may increase expression of proinflammatory molecules and cytokines. The local inflammatory effect may create a lymphocytic CD8+ response, responsible for the bandlike lymphocytic infiltrate of LP. To the best of our knowledge, the present report is the first case of radiation-induced LP with a bullous clinical presentation.


 Click to show fullsize
Click to show fullsize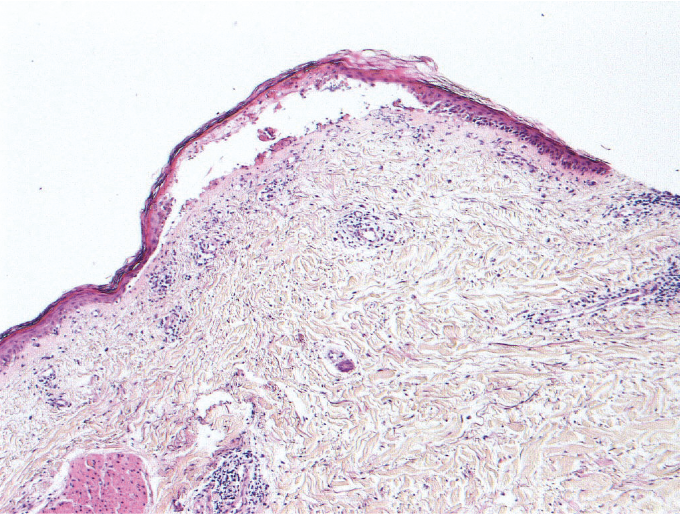 Click to show fullsize
Click to show fullsize