


1Department of Dermatology, 2Department of imaging and pathology, Translational cell and tissue research, 3Department of Surgical Oncology and 4Department of General Medical Oncology, University Hospitals Leuven, Leuven, 5Department of Hematology and Oncology, CHR Verviers East Belgium, 6VIB Center for Cancer Biology, VIB, and 7Laboratory for Translational Genetics, Department of Human Genetics, KU Leuven, Leuven, Belgium
#These authors contributed equally.
The rising incidence of cutaneous melanoma and its stable high mortality rates despite innovative cancer care, require better prediction of the clinical outcome. In a large cutaneous melanoma population we explored whether the known clinical risk factors for melanoma susceptibility (naevus phenotype, phototype, family and personal history of melanoma and sun damage) affect melanoma outcomes. A total of 1,530 melanoma patients were included. Multivariable analysis adjusted for age, sex, melanoma stage, localization and subtype showed that familial melanoma, solar lentigines on head and neck, the back of hands, arms and shoulders were associated with a better relapse free survival. The presence of atypical naevi was associated with an increased risk of relapse. After Bonferroni correction, the correlation between presence of solar lentigines on the back of the hands and arms remained the most robust and significant prognostic factor for the relapse-free survival in cutaneous melanoma patients.
Key words: melanoma, clinical risk factors, melanoma susceptibility, outcome, chronic cumulative photodamage.
Accepted Jul 17, 2019; E-published Jul 17, 2019
Acta Derm Venereol
Corr: Marjan Garmyn, MD, PhD, Department of Dermatology, University Hospitals Leuven, Herestraat 49, BE-3000 Leuven, Belgium. E-mail: marjan.garmyn@uzleuven.be
This explorative study in a large carefully phenotyped melanoma population demonstrates that melanoma susceptibility risk factors, indicative of chronic photodamage, are correlated with clinical outcome. The presence of solar lentigines on the back of the hands and arms is associated with a better relapse free survival. This finding may offer clinicians an additional tool to risk stratify their melanoma patients.
Cutaneous melanoma (CM) is the most common lethal skin disease worldwide, affecting mainly Caucasians (1). The rising incidence and stable high mortality rates of CM, despite continuously improving therapies, calls for a better prediction of its clinical outcome.
The American Joint Committee on Cancer (AJCC) for melanoma staging identified clinico-histopathological risk factors that influence the melanoma outcome, including Breslow thickness, mitosis, ulceration, sentinel node status, regional macrometastatic disease and distant metastatic disease (2). Age, sex, localization and subtype have also been associated with the melanoma outcome, although these are not yet implemented in the staging criteria (3). In addition, several risk factors have been linked to melanoma susceptibility, including a high count of common naevi, presence of atypical naevi, sun exposure, low phototype, freckles, actinic damage, and personal and family history of melanoma (4–7).
Previous studies have investigated associations of individual melanoma susceptibility risk factors, including sun exposure (8–11), family (12) or personal history of melanoma (13), and naevus phenotype (14, 15) with melanoma outcome. Most of these studies are based on questionnaires and in-person interviews on sun exposure in relatively small populations. Two large studies with respect to the impact of naevus burden on melanoma outcome (14, 15), have reported conflicting results, while other susceptibility risk factors, including skin lesions representative of chronic sun exposure, lentigines and actinic keratosis, and phototype were poorly studied, if analyzed at all. Therefore, we set out to perform a comprehensive exploratory analysis of a large panel of known clinical risk factors for melanoma susceptibility in a large and well-phenotyped contemporary Belgian melanoma population and examined their effect on the melanoma outcome.
Data collection
The study was designed and approved by the local ethics committee of the University of Leuven in 2004. Patients with a histologically proven diagnosis of cutaneous melanoma who attended the outpatient clinic of the Dermatology Department at University Hospitals Leuven, Belgium, were phenotyped at the time of inclusion and prospectively followed for relapse till 2014. Patients with in situ, mucosal melanomas and unknown primary melanoma were excluded.
Trained dermatology residents performed a full skin examination for melanoma susceptibility risk factors. Sun damage signs (solar lentigines on the head and neck, the back of the hands, arms and shoulders, actinic keratosis, ephelides, idiopathic guttatea melanosis) were carefully annotated. Solar lentigines were classified as sharply defined, brown, round/polycyclic macular lesions. Ephelides were determined from a self-reported history of freckles during in-person interviews and through physical examination. Idiopathic guttatae hypomelanosis, preferentially occurring on the chronically sun-exposed sites was clinically assessed as small, asymptomatic round to oval hypopigmented macules. Childhood sunburn (sunburn before 18 years of age) was assessed through questioning. Sunburn was defined as a painful erythema, with or without blistering, peaking 24 h after sun exposure, was self-reported and verified by the medical doctor during history taking. Melanocytic naevi, defined as light/dark brown macular or elevated lesions ≥ 2 mm, were counted over the entire body and categorized into 2 groups: < 50 and ≥ 50. The presence and number of naevi on the dorsum of the feet, the scalp and the gluteal region were quantified and atypical naevi were defined according to the presence of at least ≥ 3 of the following parameters: ill-defined borders, diameter ≥ 5 mm, variable pigmentation, irregular border and erythema (16). Histologically proven atypical naevi were also included. Every patient’s phototype was ascertained according to the Fitzpatrick’s classification (17). Patients were categorized as having a positive family history if they reported at least one affected first- or second-degree relative with melanoma. Histopathological and relevant medical data were retrieved from the electronic hospital records. Melanomas were categorized into subtypes, i.e. superficial spreading melanoma (SSM), nodular melanoma (NM), lentigo malignant melanoma (LMM), and a group consisting of other rare subtypes (acrolentiginous melanoma (ALM), desmoplastic melanoma, spitzoid melanoma, and naevoid melanoma).
The following clinical and histopathological established prognostic factors for CM were recorded for further analysis: age at diagnosis, sex, Breslow thickness, mitosis, ulceration, stage at diagnosis (according to AJCC 7th edition), localization, subtype and the above-mentioned known clinical risk factors for melanoma susceptibility. In case of multiple melanomas, the most aggressive case was included for further analysis. Data on the relapse date, last follow-up and date of death were collected. End of study date was set at December 31, 2014. Relapse-free survival (RFS) was calculated from the time of melanoma diagnosis until date of relapse or end of the study date. Relapse was defined as any recurrence/relapse of the disease (most often locoregional recurrence of melanoma such as lymph node metastasis or in transit metastasis). Relapses were confirmed by histological analysis and/or imaging.
Statistics
Data analysis was performed using the SPSS statistical software (IBM SPSS Statistics 24; Chicago, IL). Missing data were excluded from the database, but in view of the extremely low number, no imputation was performed for that data. Descriptive statistics were calculated for the clinicopathological variables. Differences in the length of follow-up were taken into account using survival analysis technique, the Cox regression model (18). The median follow-up time was 6.2 years (IQR 3.1–9.5 years).
The low number of melanoma-related deaths precluded a sufficiently powered analysis of the effect of melanoma susceptibility risk factors on melanoma cancer deaths. Therefore, only RFS was analysed. The curves of probability of recurrence were conducted with the Kaplan–Meier method and intercategorical differences were assessed with the log rank test. Univariable Cox proportional hazards models (Cox PH) were conducted to assess the associations between each of the clinicopathological variables and RFS. The multivariable analyses consisted of two steps. In the first step, results were reported from a multivariable Cox proportional hazards model for RFS, with age, sex, stage, localization and subtype as predictors. In the second step, this model was extended with each of the variables (n = 16) referring to naevus phenotype (n = 5), phototype, family history, multiple primaries and sun damage (n = 8) separately. A Bonferroni correction was applied, controlling the familywise type-I error for the results of these variables (derived from the 16 different models, p = 0.003). Hazard ratios (HR) and associated 95% confidence intervals (CI) were also reported. All values are two-sided, and a p-value less than 0.05 was considered to be statistically significant. To simplify the interpretation of the Cox proportional hazards results, we reorganized the variables stage, atypical naevi, phototype and multiple primaries into a new subgroup including stage IA, IB, II, III and IV, atypical naevi (yes versus no), phototype (3,4 versus 1, 2) and multiple primaries (yes versus no), respectively.
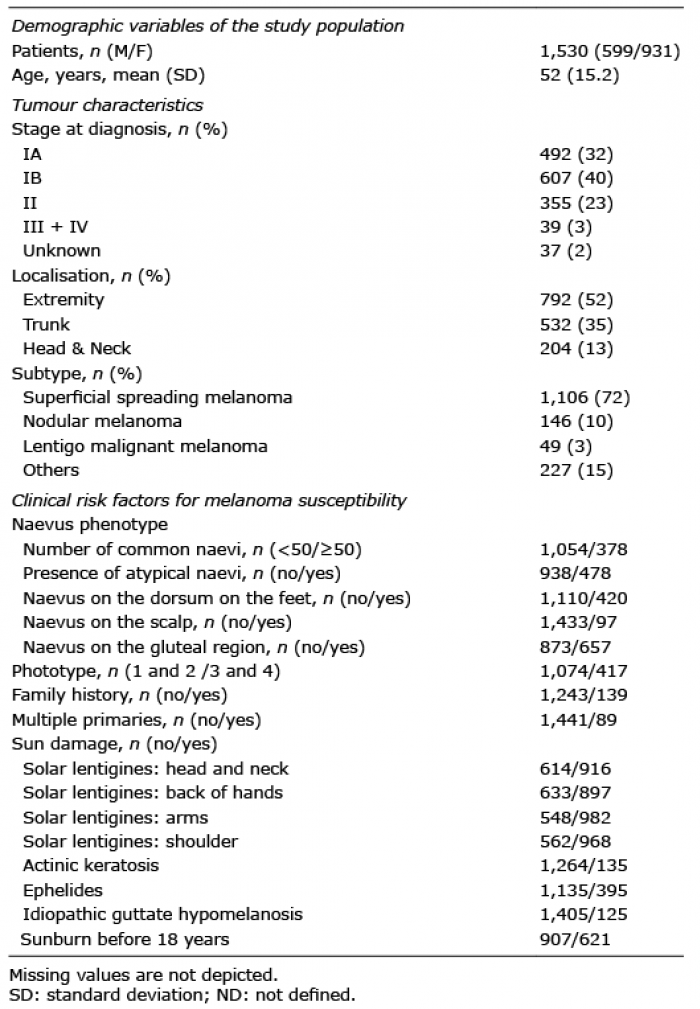
In total, 1,530 patients were included into the study (931 females and 599 males). Demographic and clinicopathological characteristics of the study population are depicted in Table I. During the follow-up period of the study, 230 melanoma patients had a relapse and 169 patients died, but only 89 patients died from the melanoma. Univariable analysis of the clinicopathological associations with RFS is shown in Table II.
Table I. Clinical and histopathological parameters of all patients
Table II. Survival association result from univariate and multivariable Cox proportional hazards models
Multivariable analysis of the prognostic factors for melanoma outcome
In the multivariable analysis, we adjusted for age, sex, stage, localization and subtype of melanoma for each predictor variables (Table II). We observed that family history of melanoma was associated with a better RFS (HR 0.61, p = 0.048), while the presence of atypical naevi was associated with an increased risk of relapse (HR 1.34, p = 0.04). The presence of solar lentigines on the back of hands (HR 0.64, p = 0.002), on arms (HR 0.66, p = 0.002) and on shoulders (HR 0.70, p = 0.005), was associated with improved RFS (Table II). After Bonferroni correction, the correlation between presence of solar lentigines on the back of hands and arms remained the most robust and significant prognostic factor for RFS in CM patients. Fig. 1 illustrates the effect of lentigines by showing the Kaplan Meyer estimates in some strata defined by age and/or stage. Note that this figure suggests that the effect of solar lentigines was stronger at a younger age. Further exploration within the multivariable Cox regression model indeed confirmed a significant interaction between solar lentigines on the back of the hands and age (p = 0.036), but not with the stage (p = 0.35) (results not shown).
Fig. 1. Kaplan-Meier plots of relapse free survival based on the presence or absence of solar lentigines back of the hands, divided by age (<50 and ≥ 50 years) and stage (IB and II).
This explorative study in a large Belgian contemporary and carefully phenotyped cutaneous melanoma population investigated the association between known clinical risk factors for melanoma susceptibility and melanoma outcome. In a multivariable analysis, with correction for age, sex, melanoma stage, location and subtype, we observed a better RFS in patients with solar lentigines. These findings indicate that within a group of patients with the same age and sex and similar melanoma characteristics, those with solar lentigines have a better melanoma outcome compared to patients without the solar lentigines. The absence of such correlation in a univariable analysis is not surprising, because of the tight positive relation between age and presence of solar lentigines, confounding the correlation with the clinical melanoma outcome. This confounding effect of age on protection associated with solar lentigines is also revealed in the Kaplan-Meier survival stratified by age and stage.
Solar lentigines are signs of chronic photodamage and typical for photoaging (19, 20). Our observations of a salutary effect on the RFS in a large melanoma population are consistent with other studies reporting a possible association between melanoma survival and elastosis, another sign of chronic photodamage (21, 22). Berwick et al. (9) also reported an inverse association between solar elastosis and melanoma-related death, independent of the strong association of melanoma-related death with melanoma site, lesion thickness and mitosis, which, however, could not be confirmed in a later study (23). A possible association between sun exposure and melanoma outcome is further supported by epidemiological studies demonstrating a beneficial effect of sun exposure or sunny holidays on melanoma outcome (10, 11) and an inverse association between mean annual sunlight in different countries and melanoma mortality (8).
Our observations of solar lentigines associated protection against relapse rate raise the intriguing question on the biological significance and potential mechanisms, whereby chronic sun damage affects the melanoma outcome. Several molecular pathways may contribute to a better melanoma prognosis following chronic sun exposure. First, the sun is an important source of vitamin D (VD) and active VD has pleiotropic anticancer effects, also on melanoma (24). Previous observational studies have shown that increased levels of VD at diagnosis predict a better outcome, and that metastatic melanoma and its poor prognosis are associated with decreased VD levels (25, 26). Second, human skin possesses different photoadaptive mechanisms, which may counteract melanoma-associated mutations resulting in less aggressive melanomas (27). Finally, sun exposure may be associated with a healthier lifestyle and higher socioeconomic status. Another potential mechanism for the observed relationship between solar lentigines and survival are shown in studies conducted on a melanoma variant; the melanocortin 1 receptor (MC1R). MC1R variants have been associated not only with increased melanoma risk and melanoma risk factors such as freckling and solar lentigines but also with a better melanoma survival. It has been postulated that although MC1R variants are at increased melanoma risk through decreased (UV) DNA damage repair, MC1R variants also confer increased susceptibility to apoptosis and decrease cell proliferation, leading to better a survival (28–30).
In addition to solar lentigines, we also investigated the association of family history and naevus phenotype, two other well-known melanoma susceptibility risk factors, with melanoma outcome.
First, family history is a risk factor for the development of primary melanoma and associated with inherited mutations in melanoma susceptibility genes, such as CDKN2A (31). Previous studies have demonstrated that germline CDKN2A status is not only associated with melanoma susceptibility, but also seems to be important for the prognosis (32). Consistent with these earlier findings a positive family history appears also to have a favourable impact on the melanoma outcome in our population. Lead time bias whereby family members of melanoma patients may seek help earlier, and may therefore be diagnosed at an earlier stage, might be an explanation but needs to be confirmed. Although in our study a favourable outcome of familial melanoma remained significant in multivariable analysis, the association was weaker than in the univariable setting (33, 34), emphasizing the need for follow-up studies.
Second, previous studies have investigated the impact of naevus phenotype (more specifically naevus count) on the melanoma outcome. In our study, not only did we investigate the naevus count, but also the other characteristics of naevus phenotype (i.e. presence of atypical naevi and localisation of the naevi) and their relation with the melanoma outcome. We observed that some characteristics of the atypical mole syndrome (16), have a better outcome in the univariable model, while in the multivariable model, patients with atypical naevi have a higher risk for relapse. A recent study by Taylor et al. (15) showed similar results, while Berwick et al. (9) did not find a significant association between nevus count and melanoma-related death. In contrast, Ribero et al. (14) reported a beneficial association between high naevus count and survival in melanoma patients. The discrepant results may be attributable to different methodologies and study populations.
Limitations
First, we used a broad definition of family history and only a limited number of events were present for the survival analysis in this population. Family history was self-reported and was not histopathologically or genealogically confirmed. Second, the lack of sentinel node data in the majority of the patients might have lead to a potential underreporting of stage III cases. Only 10% (n = 162) of our study population had undergone a sentinel lymph node biopsy which had been implemented only since the end of 2012 in our institution and a positive sentinel was observed in 15 patients (9.3%) only. Third, systemic melanoma treatments, administered predominantly for stage IV disease, were not taken into account. Finally, no adjustments were made for the residual confounders including healthy lifestyle factors, socio-economic status and other causes of death such as cardiovascular disease. Despite all the above, the large number of participants followed in a single centre, the uniform study procedures and detailed clinical annotation of melanoma susceptibility risk factors validates the major findings of this comprehensive analysis.
Conclusion
In this exploratory study we report that clinical signs of cumulative photodamage are inversely associated with melanoma outcome after adjustment for clinical and histopathological prognostic factors. This observation, however, does not prove a causal relationship between sun exposure and melanoma outcome, but may offer clinicians an additional tool to better risk stratify their melanoma patients. Further analyses are necessary to understand the biological, molecular and genetic mechanisms that account for these correlations.
We gratefully acknowledge Steffen Fieuws from Leuven Biostatistics and Statistical Bioinformatics Center (L-BioStat) for the advice and guidance in the statistical analysis. On behalf of the patients and their families, we gratefully recognize the contributions of all medical personnel and residents towards this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize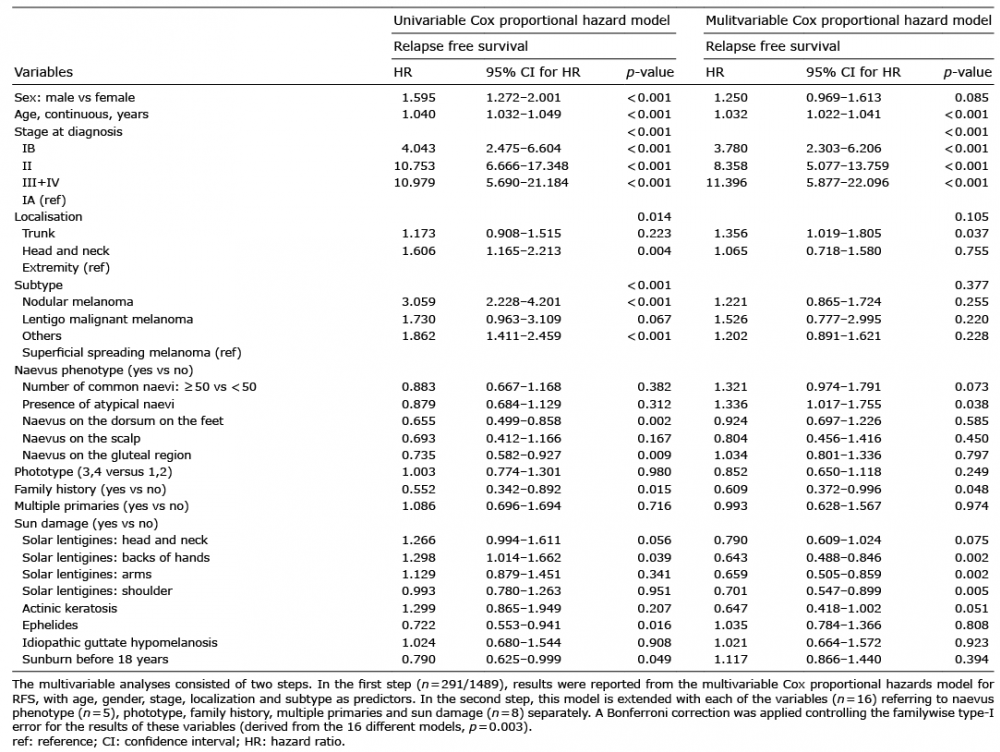 Click to show fullsize
Click to show fullsize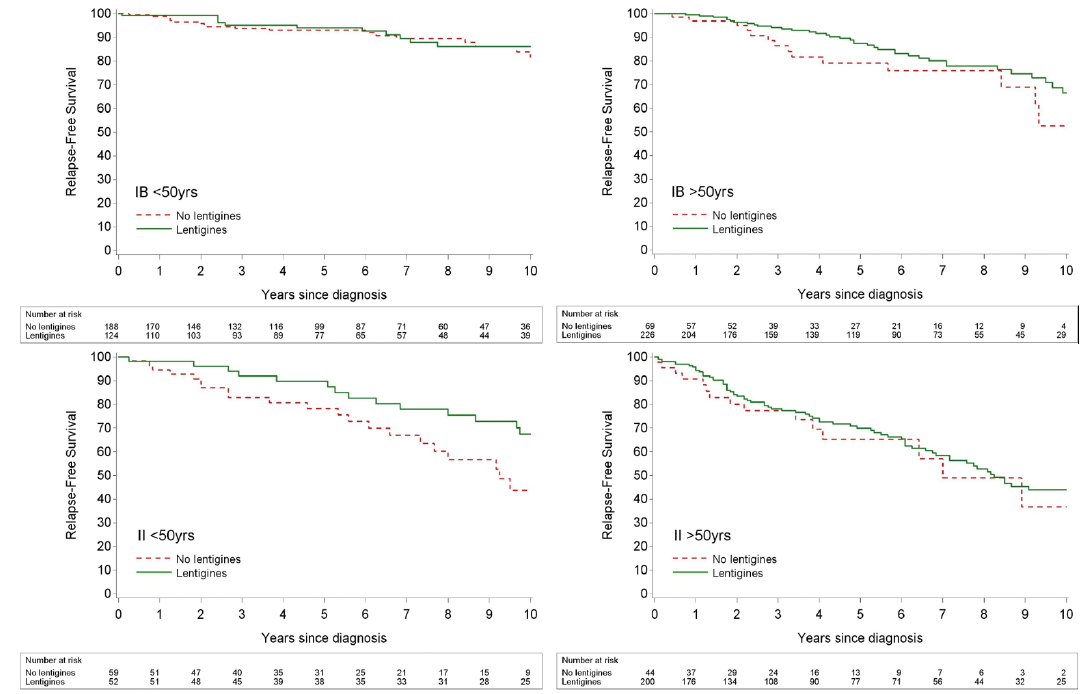 Click to show fullsize
Click to show fullsize