


1Department of Dermatology, Hôpital Saint-Eloi, University of Montpellier and INSERM U1058, 80 avenue Augustin Fliche, Montpellier Cedex 5, and 2Laboratory of Pathology, University of Montpellier, Montpellier, France. *E-mail: o-dereure@chu-montpellier.fr
Accepted Aug 12, 2019; E-published Aug 13, 2019
Epstein-Barr virus-related mucocutaneous ulcer (EBV+MCU) is a rare and recently individualized type of EBV-induced B-cell lymphoproliferative disorder, most often linked to immunosuppression. It presents mainly as unique or few mucosal and/or cutaneous ulceration(s), initially reported with an indolent, usually self-resolving course unlike other EBV-driven lymphoproliferative conditions. However, more recent reports emphasized its possible clinical heterogeneity, including multisite lesions along with a relatively more aggressive outcome in some cases. We hereby report a further observation of this rare disease that might enlarge its clinical spectrum owing to an unprecedented pattern of atypical and disseminated lesions.
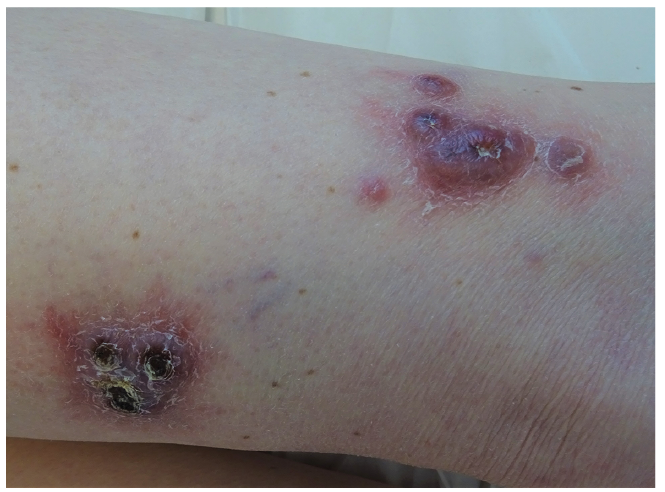
A 72-year-old male patient with no significant medical background was referred for evaluation of multiple purplish, ulcerated nodular lesions of the left thigh of 2-months duration, rapidly followed by the occurrence on similar elements on the left knee (Fig. 1) and of subcutaneous nodules located on the left shoulder, left ankle and lower back. Apart from these skin lesions, the size of which ranged from 5 to 20 mm in diameter at initial evaluation, physical examination was otherwise unremarkable with a conserved general status and no palpable lymphadenopathy. Standard biological tests showed an isolated moderate lymphopaenia (910/mm3) and monoclonal IgM kappa. Magnetic resonance imaging (MRI) of the left thigh revealed multiple cutaneous and subcutaneous hypersignals with peripheral enhancement and deep fascia invasion, whereas computed tomography (CT)-18F fluorodeoxyglucose positron emission tomography (PET) identified several hyper-metabolic subcutaneous and muscle foci of the lower limbs, the majority of which did not correspond to clinically relevant elements. Biopsies of left thigh ulceration and left ankle subcutaneous nodule both revealed a heavy dermal infiltrate, consisting of epithelioid histiocytes and polymorphonuclear leukocytes associated with atypical large Hodgkin-like, sometimes mummified cells, displaying irregular and often nucleolated nuclei along with a vastly ulcerated overlying epidermis for the thigh lesion (Fig. 2a). Plasmacytoid apoptotic cells and areas of tissue necrosis were also present. Immunostaining showed that Hodgkin-like cells were CD3– CD5– PAX5+ OCT2+ CD20– CD15+ (Fig. 2b). CD30 was highly expressed (Fig. 2c) and EBER was also strongly positive by in situ hybridization (ISH) (Fig. 2d). KI-67 expression in EBER+ cells was moderate (25–30%). Molecular biology analysis of skin lesions identified a discrete monoclonal T-cell population on a conserved polyclonal background but no significant B-cell clone. Although the clinical presentation was markedly atypical especially owing to the lack of obvious ulceration on mucous membranes, EBV+MCU was first considered on the basis of highly consistent morphological and immunophenotypical features, particularly since EBV blood PCR was positive (699 IU/ml or 2.84 log IU/ml). No relevant clinical or biological clue for an underlying immunosuppression was identified on medical history or through biological investigations (lymphocytes total count and immunophenotyping, Ig subsets dosage, HIV status). Owing to the disseminated and rapidly progressing clinical pattern, the patient received 8 courses of pegylated liposomal doxorubicin with complete clinical regression of cutaneous and subcutaneous lesions replaced by atrophic scars. The treatment was well-tolerated. Subsequent PET scan revealed complete metabolic remission of all previously hypermetabolic sites (Lugano score I), whereas EBV blood PCR remained positive at 907 IU/ml. A localized relapse occurred on the left thigh 4 months after completion of chemotherapy, efficiently treated with low-dose superficial electron-therapy. The patient was still in complete clinical remission one year after this relapse.
Fig. 1. Multiple purplish ulcerated nodular lesions on the left thigh.
Fig. 2. (a) Thigh skin biopsy (haematoxylin and eosin staining, ×20 magnification; ×40 magnification for the highly magnified inset): heterogeneous admixed dermal infiltrate of large atypical lymphocytes with occasional Reed-Sternberg-like cells, small lymphocytes, and histiocytes. (b) Strong expression of CD30 by Reed-Sternberg-like cells (×10 original magnification). (c) Expression of OCT 2 by Hodgkin-like cells (×20 original magnification). (d) Highly positive in situ hybridization for EBER (×40 original magnification).
EBV+MCU, a rare subset of EBV-related B-cell lym-phoma, initially described in 2010, displays a specific histological, phenotypic and virological pattern (1–3). It typically presents with a unique, well-limited ulcer of the oral cavity, gastrointestinal tract or skin in patients with a background of immunosuppression either iatro-genic or related to ageing that allows EBV-infected cells to proliferate at sites rich in such cells (1, 4, 5). The histopathological pattern is dominated by a superficial epithelial ulceration overlying a polymorphous infiltrate composed of atypical large cells, sometimes with Hodgkin cell-like morphology, immunoblasts and plasmacytoid apoptotic cells along with tissue necrosis. Atypical large immunoblasts and Hodgkin-like cells are PAX5+ OCT2+ MUM1+ BOB1+ CD30+ and characterized by co-expression of CD15 by a significant proportion of cells. Conversely, CD20 expression is reduced or absent in 33% of cases. All cases express EBER on ISH. Clonal rearrangement of B- and T-cell receptors genes is reported in 39% and 38% of cases, respectively (2). Differential diagnoses include cutaneous and/or mucous involvement by Hodgkin’s lymphoma, lymphomatoid granulomatosis and, most notably, age-related EBV+ diffuse large B-cell lymphoma (6). However, according to the current classification of the spectrum of age-related EBV-driven lym-phoproliferative B-cell disorders, the clinical (no visceral involvement; overall favourable outcome), histological, immunological and molecular (presence of T-cell clone and lack of massive B cell-clone) characteristics of our patient were much more consistent with the spectrum of MCU. Unlike the initial description of unilesional lesions, a multifocal pattern was subsequently, although seldom, observed in 17% of all reported cases with lesions clustered on the same anatomical region in all such patients, while mucous membranes were also involved in approximately 70% of all reports (3, 5). In contrast to a typical histological and immunohistochemical pattern, the clinical profile of our observation is unprecedented to date, with multiple, rarely ulcerated and merely cutaneous and sub-cutaneous nodules either clinically detectable or identified by PET scan only and disseminated on several anatomical areas on the trunk and the limbs with no associated involvement of mucous membranes. A relatively similar pattern with isolated multiple skin violaceous nodules or infiltrated plaques with no mucous lesions was recently reported, located on the same anatomical area as in previous observation (7). The unusual disease dynamics with rapidly enlarging lesions and the lack of iatrogenic immunosuppression amenable to drug reduction or withdrawal led to the use of monochemotherapy by pegylated liposomal doxorubicin with complete initial response and a good tolerance. Interestingly, systemic treatment was implemented in only 3 previous reports of EBV+MCU secondary to ageing-associated immunosenescence and used polychemotherapy by R-CHOP in all cases whereas other patients were treated by surgery, radiotherapy or did not receive any specific treatment owing to self-regression of lesions. According to our observation, the clinical and outcome spectrum of EBV+MCU might therefore be more extensive than reported previously and systemic monochemotherapy may be considered in multisite cases.


 Click to show fullsize
Click to show fullsize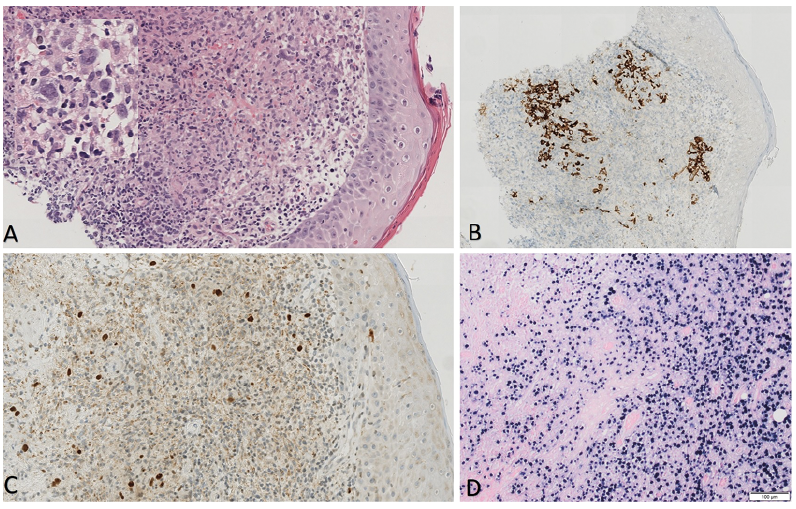 Click to show fullsize
Click to show fullsize