


1Unit of Dermatology, Department of Medicine - DIMED, University of Padova, and 2OUC of Histopathology, University of Padova, Padova, Italy. E-mail: gloriaorlando@gmail.com
Accepted Aug 22, 2019; E-published Aug 22, 2019
Osteoma cutis (OC) is a rare disorder whose main feature is the extra-skeletal bone formation with dermal deposition of hydroxyapatite crystals (1). OC can be an isolated condition or associated with Albright’s hereditary osteodystrophy or progressive osseous heteroplasia (1). Four clinical patterns of presentation have been described: single, widespread, plate-like, and multiple miliary osteomas cutis (MMOC). Single osteoma can occur anywhere on the skin as a solitary nodule. Widespread variant displays multiple generalized osteomas that arise in neonatal period (1). Plate-like osteoma is a bony plate, usually present at birth or growing during the first years of life (2). MMOC is characterized by numerous punctate foci of bone tissue inside the skin (1). In 15% of cases OC develops in the skin without any pre-existing lesion as a primary form. The remaining 85% is secondary to trauma or scars, cutaneous tumours or inflammatory skin diseases (1, 3).
Lichen planopilaris (LPP) is a primary lymphocytic cicatricial alopecia of unknown aetiology. It presents as focal or diffuse patches of alopecia that can occur anywhere on the scalp associated with pruritus or pain. Dermoscopy shows inflammatory signs such as perifollicular erythema, follicular hyperkeratosis associated with loss of follicular ostia, white fibrotic patches and sometimes tufted hairs (4).
Herein we report the case of a female patient who developed a MMOC on the scalp affected by a patch of cicatricial alopecia with clinical and histological features of LPP.
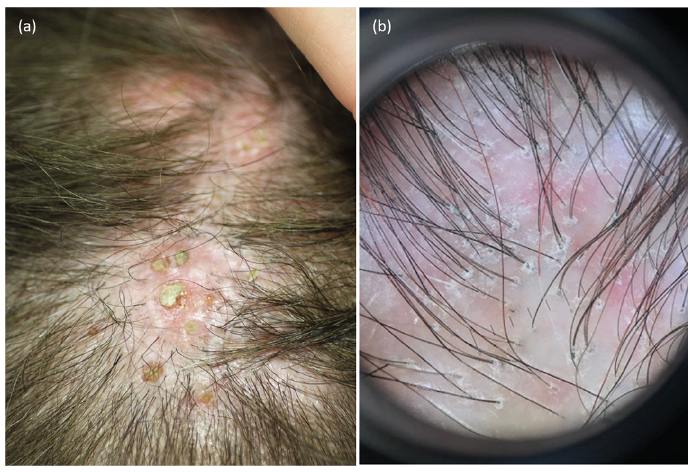
A 47-year-old woman came to our Dermatology Unit with a 10-month history of alopecia affecting the vertex, frontal and parietal areas associated with pruritus. The clinical examination showed a very hard plaque of scarring alopecia with numerous small brownish-yellow, solid, round lesions (Fig. 1a). At the margins of the plaque, dermoscopy showed perifollicular erythema and perifollicular hyperkeratosis (Fig. 1b). She suffered from migraine during the last 4 years, treated with propranolol and on-demand NSAIDs. There were no other relevant anamnestic data to report.
Serum calcium and phosphate, 24 h urine calcium, parathyroid hormone, vitamin D level and renal function were normal. The soft tissue ultrasound examination revealed the presence of multiple hyperechogenic spots measuring around 2 mm of diameter associated with hypoechogenic shadowing. Head computed tomography confirmed the evidence of punctiform cutaneous lesions with a high attenuation, suggesting the presence of osseous deposits.
Our patient underwent a 6 mm punch biopsy of the lesion that showed a lymphocytic infiltrate of the hair follicle epithelium and the perifollicular region associated with perifollicular fibrosis and sclerotic collagen. The lymphocytic infiltrate mainly involved the isthmus and the infundibular region. In addition, histopathology evidenced multiple punctate ossification foci with bone marrow and mature bone tissue originating inside some residual hair follicles (Fig. 2). Clinical and histological features led to the final diagnosis of MMOC secondary to LPP.
The treatment with hydroxychloroquine 400 mg/day associated with topical clobetasol propionate 0.05% ointment improved the patient’s symptoms and stopped further progression of the ossification process. The patient refused any invasive procedure to remove the osteomas.
Fig. 1. (a) Multiple, brownish, stone-hard structures measuring around 3 mm of diameter inside a scarring alopecia patch of the vertex. (b) Dermoscopy at the periphery of the lesion: perifollicular erythema and hyperkeratosis, white areas and loss of follicular ostia.
Fig. 2. Histological features: (a) Multiple puntacte ossification foci in the papillary and reticular layers of the skin (hematoxylin-eosin (H&E) 1.5x); (b) lymphocytic infiltrate involving perifollicular and follicular regions, perifollicular fibrosis and sclerotic collagen associated with osteomas (H&E 10x); (c) an osteoma showing mature lamellar bone (H&E 20x); (d) an osteoma with numerous osteocytes and Haversian canals (H&E 40x).
First described in 1864 by Virchow, MMOC is defined by multiple, normochromic and hard papular skin lesions that mainly affect female patients usually on the face. An extra-facial presentation is described in only 15% of patients principally involving shoulders, neck and back (5). So far, 70 cases of MMOC have been reported. In a recent radiological study, Kim et al. (6) described facial calcified nodules compatible with miliary osteomas as a very common finding in routine CT images of the head, suggesting that MMOC is probably underdiagnosed. In 1928 Hopkins first suggested the association with acne and afterwards a previous history of acne has been described in 55% of cases of MMOC (5). Lesions acquire a bluish coloration in patients who used tetracycline (7). The pathogenesis is still unknown. In 2010, Myllylä et al. (3) demonstrated that mesenchymal cells present in the dermis, such as fibroblasts, have the ability to differentiate into osteoblasts leading to an osteoblastic metaplasia. Diagnosis is based on clinical, radiological and histological features but only the latter allows to differentiate OC from calcinosis cutis that shows calcium deposition within the dermis instead of true bone formation (8).
Literature reports two cases of primary MMOC of the scalp (5, 9) and one case of MMOC secondary to folliculitis decalvans (10). To our knowledge, this is the first reported case of OC originating from a previous LPP. LPP is a cicatricial disorder and therefore it could possibly trigger an osteoblastic metaplasia of fibroblasts, causing a secondary MMOC. Our case suggests that LPP can be included among scarring and inflammatory processes that can induce OC.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize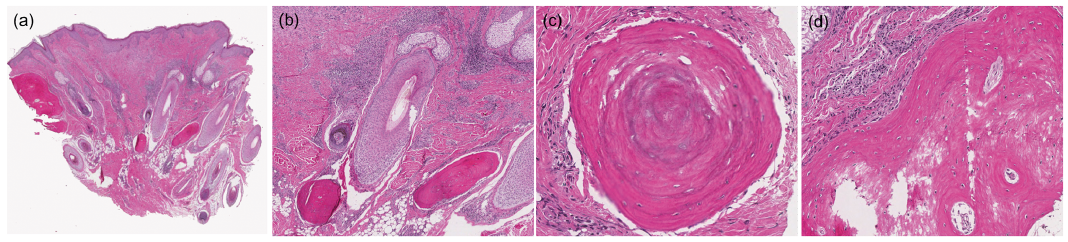 Click to show fullsize
Click to show fullsize