


Institute of Dermatology, Jiangsu Key Laboratory of Molecular Biology for Skin Disease and STIs, Chinese Academy of Medical Sciences & Peking Union Medical College, 12 JiangWangMiao Street, Nanjing Jiangsu, 210042, China. *E-mails: ifmtjoel@163.com; kunchen181@aliyun.com
#These authors contributed equally.
Accepted Aug 26, 2019; E-published Aug 27, 2019
Glomus tumours are benign vascular hamartomas arising from the glomus body in the reticular dermis. They can be classified as solitary or multiple forms, with the latter being subdivided into regional and disseminated types. Glomangiomyomas are the least common histological type of glomus tumour (1). We describe here a case of acquired regional multiple plaque-like glomangiomyoma.
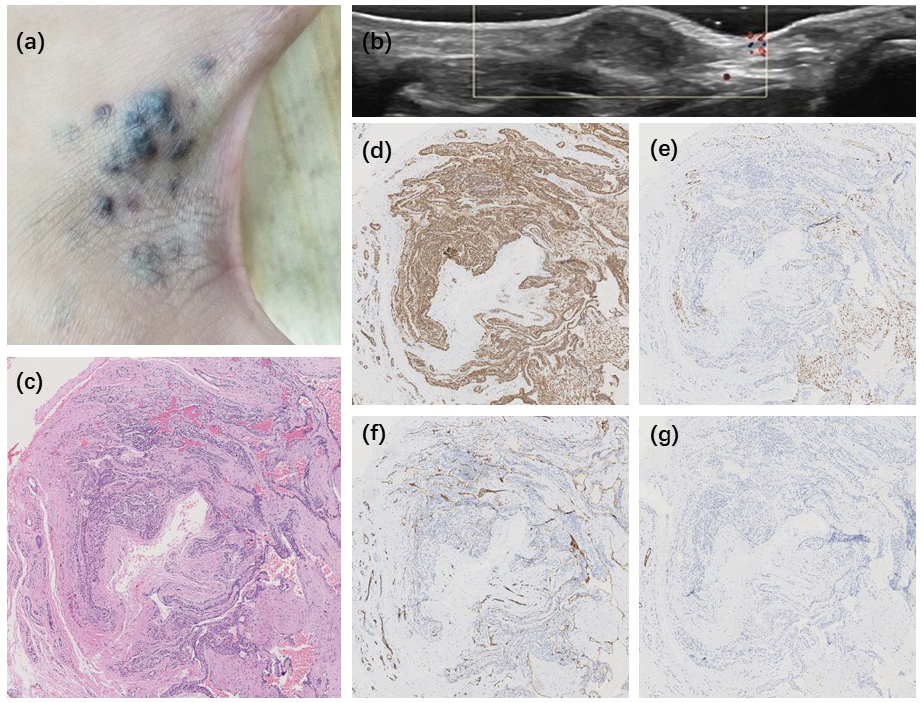
A 20-year-old Chinese man presented with an 8-year history of multiple progressively asymptomatic nodules on his left hand. Physical examination revealed a plaque-like, bluish lesion, with overlying coalescent, point to horsebean-sized, ranging from 2 mm to 20 mm, dull red-to-tan papules and nodules on the first web space of the left hand (Fig. 1a). Ultrasound scans revealed hypoechoic solid masses in the subcutaneous region, with no obvious blood flow signal (Fig. 1b). A skin biopsy specimen revealed a well-demarcated tumour in the dermis, which comprised uniform eosinophilic cytoplasmic cells, with round, large hyperchromatic nuclei. Around large vessels there was a gradual transition from glomus cells to spindle-shaped smooth muscle cells with long blunt-ended nuclei (Fig. 1c). Immunohistochemical examination revealed intensely positive reactions for smooth muscle actin (SMA) in glomus cells (Fig. 1d), desmin in muscle bundles (Fig. 1e) and CD31 in blood vessels (Fig. 1f). The homogeneous glomus cells stained negative for desmin and P63 (Fig. 1g). Given the clinical and histopathological findings, a diagnosis of glomangio-myoma was made.
Fig. 1. (a) Multiple grouped dull red-to-tan papules and nodules coalescing into bluish plaques on the first web space of the patient’s left hand. (b) The hypoechoic mass without obvious blood flow signal. (c) A gradual transition from glomus cells to spindle-shaped smooth muscle cells with long blunt-ended nuclei around vascular spaces (haematoxylin-eosin (HE); ×40). (d) The homogeneous eosinophilic cytoplasmic glomus cells stained positive for smooth muscle actin (SMA) (×40). (e) Some muscle bundles stained positive for desmin, but negative in glomus cells (×40). (f) Some blood vessels stained positive for CD31 (×40). (g) The homogeneous eosinophilic cytoplasmic cells stained negative for P63 (×40).
Glomus tumours occur in solitary or multiple forms. Solitary glomus tumours typically represent as a nodule accompanied by a faint bluish discoloration beneath the nail, with pain, tenderness and temperature sensitivity, and a significant female predominance. Only 10% of cases present as multiple lesions and they mainly occur in male adolescents (2). Multiple glomus tumours are subdivided into regional, when limited to one area of the body, and disseminated, when multiple lesions are scattered over the body. Within the group of multiple glomus tumours, congenital plaque-like variant, first reported by Landthaler et al. (1) in 1990, is present at birth and enlarges with age. It is characterized by numerous reddish-blue papules coalesced into solitary or multiple bluish plaques.
Histologically, glomus tumours are categorized into solid glomus tumour, glomangioma and glomangio-myoma according to the predominant component. The solid form chiefly includes rounded uniform glomus cells surrounding the vascular lumina and small vascular spaces. Glomangioma has larger and more irregular vascular spaces coated with a few layers of glomus cells and is less well circumscribed; it is usually seen in multiple or familial cases including congenital multiple plaque-like type. Glomangiomyoma consists of prominent smooth muscle cells and a gradual transition from glomus cells to elongated mature smooth muscle cells surrounding large vessels (3).
We report here a rare case of glomangiomyoma located in the first web space of the left hand. The features of the lesions closely resembled those of congenital multiple plaque-like glomus tumours. There is one previous report of a congenital multiple plaque-like glomangiomyoma (4). An acquired variant of the plaque-like glomangio-myoma was also reported, but this was disseminated (5). To our knowledge, this is the first report of regional multiple plaque-like glomangiomyoma.
This study was supported by CAMS Innovation Fund for Medical Sciences (CIFMS-2017-12M-1-017) and The Introduction Project of Clinical Expert Team in Suzhou (SZYJTD201811).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize