


1Department of Dermatology, Second Xiangya Hospital of Central South University, Changsha, 410011, and 2Department of Dermatology, Hainan Provincial Dermatology Disease Hospital, Haikou 570206, China. *E-mail: annymilk@126.com; xiaorong65@csu.edu.cn
Accepted Oct 14, 2019; E-published Oct 14, 2019
Rosai-Dorfman disease (RDD) is an uncommon, benign non-Langerhans’ cell histiocytic disorder, typically involving bilateral painless cervical lymphadenopathy. RDD only rarely affects extranodal sites, such as the skin, orbit, respiratory tract, central nervous system and soft tissues (1). RDD occurs most commonly in children or young adults, with no obvious difference according to sex. With no specific laboratory data, diagnosis of RDD is usually based on pathology, characterized by proliferation of histiocytes (S-100 and CD68-positive, CD1a-negative) evidently displaying phagocytosis, an inflammatory setting of lymphocytes, and a mass of plasma cells.
We report here a rare case of a patient with RDD with combined bilateral macular damage and systemic extensive skin lesions, accompanied by elevated interleukin (IL)-6 in the blood.
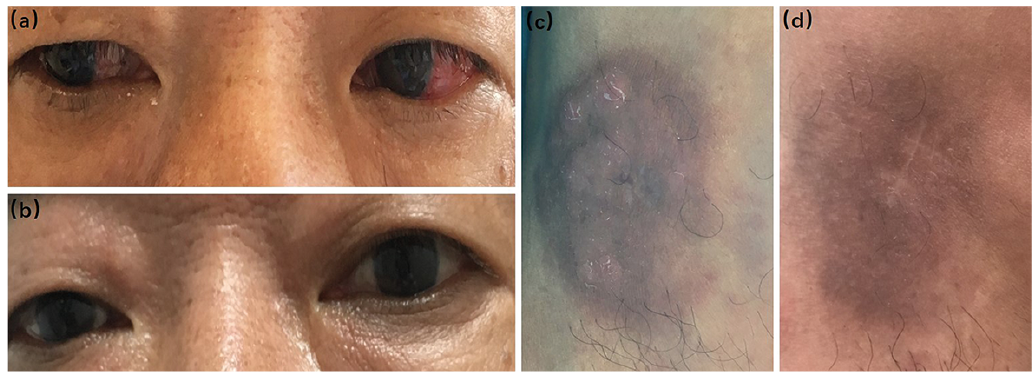
A 54-year-old man initially presented with a 1.5-year history of painless red nodules and masses on the left cheek and both legs. Six months later, he developed congestion, oedema, photophobia and itching in both eyes, which ophthalmologists considered to be conjunctivitis or scleritis (Fig. 1a, c). In order to confirm the diagnosis, he presented to a clinic at a local hospital, where he underwent a skin biopsy and immunohistochemistry. The results suggested primary skin CD4-positive T-cell proliferative disease. However, the lesions were still in progress after intramuscular injection of interferon-2α (3 million IU, every other day) and local corticosteroid injection (compound betamethasone injection 1 ml once a month).
Fig. 1. Clinical images. (a) Mild conjunctival edema and eye congestion before treatment; (b) Eye symptoms disappeared after treatment; (c)Red nodules and masses on the legs before treatment; (d) Skin lesions resolved after treatment, leaving some pigmentation.
The patient was admitted to our hospital for diagnosis and treatment. Laboratory data revealed increased erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and IL-6 levels. The following tests were normal: body temperature, liver and renal function test, microorganisms, autoimmune antibody (e.g. antinuclear antibody and rheumatoid related antibody), bone marrow cytology, albumin, serum IgG4, IgA, IgM, IgG, IgE, alpha-globulin, beta-globulin and gamma-globulin. Enhanced computed tomography (CT) revealed enlarged mediastinal lymph nodes. Magnetic resonance imaging (MRI) indicated right popliteal nodules, which may be the enlarged lymph nodes. Colour Doppler ultrasound showed vitreous opacity of the eyes and enlargement of lymph nodes in the neck, axilla, and groin. Corneal confocal microscopy revealed a normal epithelial and stromal layer of the right eye, and a large number of hypo-reflective keratic precipitates (KPs), hyper-reflective KPs and inflammatory cells deposited on the endothelium as well as founded in the anterior chamber. Optical coherence tomography of both eyes showed the partial thickness of retinal pigment epithelium became thinner and hyper-reflective bulges were observed. Anterior chamber puncture found that both IL-6 and IL-10 were increased in the aqueous humour. Another skin biopsy was performed of the same lesion on the right knee. Haematoxylin and eosin (HE) stains showed perivascular infiltration of many small lymphocytes mixed with histiocyte and plasma cells in the superficial and deep dermis. Hemosiderin was also seen in the dermis (Fig. S1). IgG4 (+)/IgG (+)>40%. This indicated that the skin lesions had probably been caused by IgG4-related disease. The rearrangement of T cell receptor was negative. Furthermore, immunohistochemical test revealed that the large histiocytes were positive for S100, and the histiocytic marker CD68. The cells were negative for Langerhans’ histiocytic marker CD1a. The histiocytes were also focally positive for IgG, IgG4 (+) /IgG (+) >40% (Fig. S2). A diagnosis of RDD was made based on the clinical presentation and pathology results.
Oral prednisone (20 mg daily, reduced by 5 mg each month) was added to the treatment. The patient then remained on a maintenance dose of 5 mg prednisone. The follow-up period was 18 months. During this time, the patient achieved clinical remission of the skin and eye lesions (Fig. 1 b, d), with no recurrence of the symptoms described above. ESR, CRP, IL-6, and colour Doppler ultrasound of the eyes were all normal. The enlarged lymph nodes in other parts of the body returned to normal, and enhanced CT scan revealed that the enlarged mediastinal lymph nodes had reduced in size.
The patient was admitted to our hospital for diagnosis and treatment. Laboratory data revealed increased erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and IL-6 levels. The following tests were normal: body temperature, liver and renal function test, microorganisms, autoimmune antibody (e.g. antinuclear antibody and rheumatoid related antibody), bone marrow cytology, albumin, serum IgG4, IgA, IgM, IgG, IgE, alpha-globulin, beta-globulin and gamma-globulin. Enhanced computed tomography (CT) revealed enlarged mediastinal lymph nodes. Magnetic resonance imaging (MRI) indicated right popliteal nodules, which may be the enlarged lymph nodes. Colour Doppler ultrasound showed vitreous opacity of the eyes and enlargement of lymph nodes in the neck, axilla, and groin. Corneal confocal microscopy revealed a normal epithelial and stromal layer of the right eye, and a large number of hypo-reflective keratic precipitates (KPs), hyper-reflective KPs and inflammatory cells deposited on the endothelium as well as founded in the anterior chamber. Optical coherence tomography of both eyes showed the partial thickness of retinal pigment epithelium became thinner and hyper-reflective bulges were observed. Anterior chamber puncture found that both IL-6 and IL-10 were increased in the aqueous humour. Another skin biopsy was performed of the same lesion on the right knee. Haematoxylin and eosin (HE) stains showed perivascular infiltration of many small lymphocytes mixed with histiocyte and plasma cells in the superficial and deep dermis. Hemosiderin was also seen in the dermis (Fig. S1). IgG4 (+)/IgG (+)>40%. This indicated that the skin lesions had probably been caused by IgG4-related disease. The rearrangement of T cell receptor was negative. Furthermore, immunohistochemical test revealed that the large histiocytes were positive for S100, and the histiocytic marker CD68. The cells were negative for Langerhans’ histiocytic marker CD1a. The histiocytes were also focally positive for IgG, IgG4 (+) /IgG (+) >40% (Fig. S2). A diagnosis of RDD was made based on the clinical presentation and pathology results.
Oral prednisone (20 mg daily, reduced by 5 mg each month) was added to the treatment. The patient then remained on a maintenance dose of 5 mg prednisone. The follow-up period was 18 months. During this time, the patient achieved clinical remission of the skin and eye lesions (Fig. 1 b, d), with no recurrence of the symptoms described above. ESR, CRP, IL-6, and colour Doppler ultrasound of the eyes were all normal. The enlarged lymph nodes in other parts of the body returned to normal, and enhanced CT scan revealed that the enlarged mediastinal lymph nodes had reduced in size.
RDD can be a general disorder, often affecting the lymph nodes. Unlike nodal disease, extranodal disease could involve any site on the patient’s anatomy. Head and neck lesions are the most common extranodal lesions, ophthalmic lesions have been reported in only 10–11% of patients (usually manifesting as lymphoproliferation in the soft tissues of the orbit and eyelid) (2, 3), and multiple system involvement is less common. The patient described here had macular involvement, bilateral ocular vasculitis, extensive body lesions, and mediastinal lymph node enlargement, which are rarely reported.
Diagnosis of RDD is usually based on its pathological manifestations (4). The usual microscopic features are that lymph node structure was partially or incompletely destroyed and lymphoid follicles had disappeared. There may be interstitial fibrosis. The most prominent shape was that of the dilated lymphatic sinuses, which were filled with tissue cells, small lymphocytes, plasma cells, and neutrophils. Histiocytes, occasionally undergoing mitosis, appeared large and foamy, containing abundant cytoplasm, either granular or vacuolated, with vesicular nuclei round-to-oval in shape. Significantly, large histiocytes with emperipolesis and positive staining for S-100 and CD68, but negative staining for CD1a, were observed (5, 6). Clinically, the typical symptoms of RDD are painless enlargement of bilateral cervical lymph nodes with fever, elevated neutrophils, increased ESR, and hyperglobulinaemia (7). Although it is a self-limiting disease, the prognosis of RDD may be life-threatening if vital organs are involved. The efficacy of treatment is not clear. Various treatment modalities exist, including steroid therapy, chemotherapeutic regimens, radiotherapy, surgery, and combinations of the above (3, 5). The choice of glucocorticoid treatment in the current case showed good results in long-term follow-up.
IL-6 levels in the blood and aqueous humour of our patient were elevated, which was also mentioned in other reports (8). Further studies have shown that IL-6 is associated with vasculitis (9). Consistent with these findings, our patient’s eyes manifested vasculitis. In subsequent observations, the IL-6 titre returned to normal after recovery. We consider that IL-6 plays a role in this disease. RDD cells are also known as S-100-positive, CD1a-negative activated macrophages (10), and macro-phages can enhance the production of proinflammatory cytokines, such as IL-6, IL-1β, and TNF-α, through the PI3K/AKT/mTOR signalling pathway (11). T lymphocytes and B lymphocytes can also produce IL-6. IL-6 can assist recruitment from neutrophils to monocytes, and IL-6, TNF-α, and IL-1β can also promote the production of macrophage colony-stimulating factor by monocytes (6). IL-6 can induce monocyte differentiation. Thus, more macrophages and cytokines were produced, which sustained the development of RDD. In conclusion, IL-6 plays a pivotal role in the development of this rare disease.
IL-6 is a prototypical cytokine with multiple cellular effects, including facilitation of cell-to-cell communication in immune responses. It can induce the differentiation of activated B cells into immunoglobulin-producing plasma cells and cause antibody production (12). Previous research has mentioned that IL-6 is associated with production of IgG4 (6). Here, the patient’s skin biopsy manifested plasma cell infiltration, and immunohistochemistry revealed IgG4 (+)/IgG (+)>40%.
The report shows that RDD and IgG4-related diseases (IgG4-RD) are connected (13). Furthermore, a subset of RDD has the same features as IgG4-RD (14). However, we can distinguish these 2 diseases using their pathological and clinical features. The characteristic manifestation of RDD is large histiocytes with emperipolesis and positive staining for S-100 and CD68, negative staining for CD1a, while IgG4-RD has no cell emperipolesis phenomenon, but often involves the pancreas and lacrimal/salivary glands (15), and serum IgG4 is often increased. To date, the pathogenesis of RDD disease has been unknown. Further research is required to determine whether there is overlap between these 2 diseases, or if they interact with each other in some way.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize