


Department of Dermatology, Kosin University College of Medicine, 262 Gamcheon-ro, Seo-gu, Busan, 602-702, Korea. *E-mail: ksderm77@unitel.co.kr
Accepted Oct 15, 2019; E-published Oct 17, 2019
Rosacea is a common chronic inflammatory skin disease that almost exclusively affects the central facial skin in a symmetrical pattern. Granulomatous rosacea (GR) is the only variant of rosacea characterized by its unique histopatho-logical findings (1). As with non-granulomatous rosacea (NGR), the pathogenesis of GR remains unclear. It has been shown that exposure of skin to ultraviolet radiation (UVR) upregulates matrix metalloproteinases (MMPs), mast cell, and transient receptor potential vanilloid type 1 (TRPV1) expression, and that these factors are involved in the pathogenesis of rosacea (2, 3). However, immunohistochemical expression of TRPV1 and CD117, which are key markers of neurovascular dysregulation, in GR has not been reported. This study compared the immuno-histochemical expression of MMP-1, MMP-9, TRPV1 and CD117, and the grade of inflammation in GR lesions with those of NGR lesions, and attempted to identify the relationship between GR and neurovascular dysregulation.
This study included 22 patients clinically and histopathologically diagnosed with rosacea at the Department of Dermatology, Kosin University Gospel Hospital, Busan, Korea.
Haematoxylin and eosin (H&E) staining was used to confirm the histopathological diagnosis of GR and NGR. In addition, the degree of epidermal and dermal inflammation was evaluated. Two dermatologists scored the samples using a 5-point semi-quantitative scale (0=normal with no inflammation, to 4=widespread inflammation).
Paraffin-embedded tissue sections were stained using monoclonal antibodies against CD117, MMP-1, MMP-9 and TRPV1. For quantitative evaluation of CD117 immunoreactivity, the number of positive cells was counted manually in 3 different fields at a magnification of ×200, and the mean calculated. In addition, expression of MMP-1, MMP-9 and TRPV1 was evaluated by digital morphometry with an image analysis program (ImageJ, NIH, Bethesda, MD, USA). Images were evaluated and the selected pixels representing positive cells were expressed as the percentage of the total area. Expression of immunoreactivity was graded on a 5-point semi-quantitative scale (0 = 0%, 1 = < 10%, 2 = 10–50%, 3 = 50–90%, 4 = > 90%).
Student’s t-test was used to compare staining patterns between groups using the Statistical Package for the Social Sciences, version 17.0 for Windows (SPSS Inc., Chicago, IL, USA). Results were considered statistically significant at a p-value < 0.05. Data are expressed as the mean ± standard deviation.
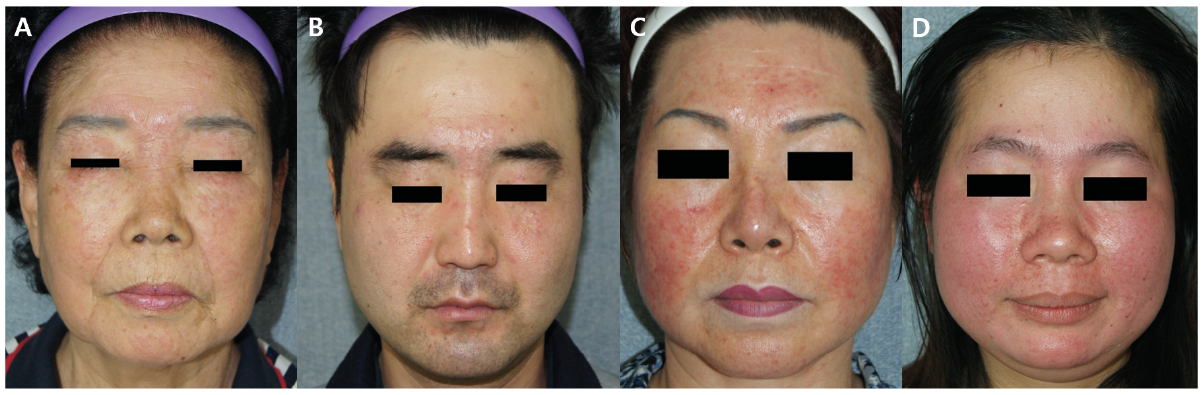
The 11 patients with GR comprised 5 males and 6 females, while 4 patients in the NGR group were male and 7 were female. The mean age was 49.8 years (range 22–71 years) in the GR group, and 49.9 years (range 30–73 years) in the NGR group. The mean duration of disease was 9.9 months in the GR group and 17.3 months in the NGR group (Fig. 1A–D).
Fig. 1. (A, B) Patients with granulomatous rosacea (GR) had periocular lesions and showed an asymmetrical distribution. (C, D) Patients with non-granulomatous rosacea (NGR) spared the periocular area and showed a symmetrical distribution. Permission is given to publish these photos. For complete details, see Fig. S1.
The mean degree of inflammation evaluated by a 5-point semi-quantitative scale was 3.09 (range 2–4) in the GR lesions, and 2.27 (range 2–3) in the NGR lesions. The mean score in GR lesions was significantly higher than in the NGR lesions (p = 0.01) (Tables SI and SII).
The mean number of CD117+ cells was 29.61 (range 22.67–39.0) in the GR lesions, and 24 (range 10.33–39.33) in the NGR lesions. However, there were no statistically significant differences in the mean number of CD117+ cells between the 2 groups (p = 0.127). The mean score for MMP-1 was 1.91 ± 0.3 in the GR lesions and 1.45 ± 0.52 in the NGR lesions. MMP-1 expression in GR lesions was statistically higher than in NGR lesions (p = 0.024), especially in the area of the granuloma. The mean score for MMP-9 was 2 ± 0.45 in the GR lesions and 1 ± 0 in the NGR lesions. MMP-9 expression in GR lesions was significantly higher than in NGR lesions and, again, expression in the area of the granuloma was especially high (p < 0.001) The mean score of a 5-point semi-quantitative scale for TRPV1 was 1.91 ± 0.3 in the GR lesions and 1.36 ± 0.5 in the NGR lesions. TRPV1 expression in GR lesions was statistically higher than in NGR lesions (p = 0.007), especially in the area of the granuloma (Fig. S1E–L1, Tables SI and SII).
GR is a variant of rosacea with histopathological findings of granulomatous infiltration (1). Recruitment of inflammatory cells, such as lymphocytes and histiocytes, are required for granuloma (4). In this regard, we hypothesized that inflammatory cell infiltration may be more prominent in GR lesions than NGR lesions. The current study showed that the degree of inflammation in the epidermis and dermis evaluated on a 5-point semi-quantitative scale was significantly more prominent in the GR lesions compared with the NGR lesions, supporting our hypothesis.
Increased expression of MMPs causes dermal matrix damage, and the damaged dermal matrix may induce leakage and accumulation of inflammatory mediators and prolonged retention of inflammatory cells, which could lead to granuloma formation (1, 5). Jang et al. (1) reported that MMP-9 expression was significantly higher in GR lesions compared with NGR lesions. Consistent with Jang et al. (1), we found significantly higher MMP-1 and MMP-9 expression in GR lesions compared with NGR lesions, especially in the area of the granulomas.
Muto et al. (6) suggested that after LL-37 is released from the epidermis in a rosacea patient’s skin, it in turn activates mast cells to release proteases, such as chymase, tryptase and MMPs. These proteases can induce dermal inflammation, inflammatory cell recruitment, and tissue remodelling (6, 7). From this perspective, therefore, mast cell activation may be important for granuloma formation in GR. In this study, however, we could not find the statistically significant differences in expression of CD117 between the 2 groups.
Overexpression of TRPV1, resulting in neuropeptide release, is associated with the pathogenesis of rosacea (8). Lee et al. (3) suggested that TRPV1, activated by UVR and heat, increased MMP-1 expression through a calcium-dependent protein kinase C signalling pathway, and the increased MMP-1 expression can induce collagen degradation and tissue remodelling. In this study, TRPV1 expression was significantly higher in GR lesions compared with NGR lesions, especially in the area of the granulomas. These findings suggest that neurovascular dysregulation may be involved in the pathophysiology of GR, and TRPV1 may play an important role in the development of granuloma by recruitment of inflammatory cells and tissue remodelling that is necessary for granuloma formation.
In conclusion, MMP-1, MMP-9 and TRPV1 may play an important role in granuloma formation in GR. Furthermore, the results of the current study suggest that neurovascular dysregulation may also be involved in the pathophysiology of GR, especially in the process of granuloma formation. However, there were several limitations to the current study. A previous study suggested that the increased expression of MMPs may participate in granuloma formation of GR in association with UVR (1). However, we did not directly evaluate the role of UVR in association with GR and NGR. In addition, we investigated the expression of several factors using only immunohistochemical staining. Thus, further studies are needed to overcome the limitations of this retrospective study, to evaluate the role of UVR in GR and NGR, and to understand the molecular mechanisms underlying how mast cells, TRPV1, MMP-1 and MMP-9 induce granuloma formation in GR. A better understanding of the molecular mechanisms of GR may provide a guide to prevention and treatment.


 Click to show fullsize
Click to show fullsize