


1School of Health Care Administration, College of Management, Taipei Medical University, 2Division of Nephrology, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, 3Division of Nephrology, Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, 4Department of Medical Research, Cardinal Tien Hospital, 5Department of Dermatology, Cardinal Tien Hospital, and 6School of Medicine, Fu-Jen Catholic University, New Taipei City, Taiwan
#These authors contributed equally and should be considered as first authors.
This study investigated the predominant skin cancer subtype among organ transplant recipients, patients on chronic dialysis, and patients with chronic kidney disease in Asian subjects. Among 23,644 patients with skin cancer, identified from Taiwan Cancer Registry Database, 53 were organ transplant recipients, 255 were on chronic dialysis, 1,792 had chronic kidney disease, and 21,544 were in the control group. The proportions of squamous cell carcinoma were 52.8%, 47.8%, 40.1%, and 33.5%, respectively. Compared with the control group, organ transplant recipients (1.99-fold) and patients on chronic dialysis (1.25-fold) were at higher risk of developing squamous cell carcinoma than other skin cancers after adjustment for potential confounders. Subgroups or covariates associated with increased squamous cell carcinoma compared with other skin cancer risk included patients with chronic kidney disease aged < 70 years (vs. control group; 1.3-fold), old age (vs. young age; 2.8-fold), male sex (vs. female sex; 1.1-fold), and south Taiwan residency (vs. north Taiwan residency; 1.1-fold). Organ transplant recipients and patients on chronic dialysis had immune dysregulation, resulting in increased risk of squamous cell carcinomas.
Key words: organ transplant recipient; dialysis; chronic kidney disease; squamous cell carcinoma; epidemiology.
Accepted Oct 15, 2019; E-published Oct 17, 2019
Acta Derm Venereol 2020; 100: XX–XX.
Corr: Chia-Chen Wang, Department of Dermatology, Cardinal Tien Hospital, and School of Medicine, Fu-Jen Catholic University, No. 362, Zhongzheng Rd, Xindian Dist., New Taipei City 231, Taiwan. E-mail: jamiewang@tma.tw
Organ transplant recipients, patients on chronic dialysis, and patients with chronic kidney disease have immune dysregulation and are at higher risk of skin cancers. However, the predominant skin cancer subtype in these populations has not been well-investigated among Asian subjects. The study revealed that organ transplant recipients, patients on chronic dialysis, older patients, males, and residents of south Taiwan (which has a high level of solar radiation) had a higher risk of developing squamous cell carcinoma than other skin cancer subtypes. The study provides aetiological insights into the development of squamous cell carcinoma and highlights that physicians should be aware of the increased risk of squamous cell carcinoma in these conditions.
Skin cancer is the most common cancer in Caucasians. Non-melanoma skin cancer (NMSC) accounts for the vast majority of skin cancers, and basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are the most common subtypes. The BCC to SCC ratio in the general population is 4:1 in the UK and 5:2 in Australia (1). The risk of NMSC increases with exposure to ultraviolet radiation, fair skin pigmentation, older age, and among people with certain medical conditions affecting the immune system. A greater increase in risk of SCC than BCC is observed in many immune-related conditions (2). Most notably, with the requirement for long-term immunosuppressant treatment to avoid graft rejection, organ transplant recipients (OTRs) of Caucasian ethnicity are at 65- to 250-fold and 10- to 16-fold risk of SCC and BCC, respectively, compared with the general population (3–5). The risk of SCC in OTRs is greatly increased compared with the risk of BCC, with a SCC to BCC ratio of 1.6:1 in the Netherlands (5) and 1:1 in Denmark (6). Compared with OTRs of Caucasian ethnicity, there is a much lower incidence of skin cancers among OTRs of Asian ethnicity. Among studies regarding the risk of cancer in OTRs from Japan (7, 8), Korea (9), China (10), Taiwan (11, 12) and Asian immigrations to the USA (13), the number of cases of skin cancers was quite small, and the proportion of histological subtypes was unclear.
Patients on chronic dialysis (14, 15) and those with pre-dialysis chronic kidney disease (CKD) (6, 16) are also at higher risk of NMSC, owing to the accumulation of uraemic toxins, further leading to chronic inflammation and oxidative DNA damage. Patients on chronic dialysis are at 5.3-fold risk of NMSC (excluding BCC) (14) in Denmark and 1.58-fold risk of NMSC (including all types of NMSC) (15) in Taiwan compared with the general population. Among patients with CKD in Denmark who are hospitalized and age < 70 years, there is a 4.8-fold risk of SCC and stationary risk of BCC compared with the general population (6). In Taiwan, the risk of NMSC (including all types of NMSC) in total CKD and stage 5 CKD patients is 1.14-fold and 1.48-fold, respectively, compared with the general population (16). Based on these studies, the increased risk of NMSC in patients on chronic dialysis and those with CKD appears to be more related to SCC than to BCC. Further studies are necessary to confirm this association, especially in subjects of Asian ethnicity.
The aim of this nationwide population-based study was to investigate the proportion of histological subtypes and clinical characteristics of skin cancers among OTRs, patients on chronic dialysis, and those with CKD, using the Taiwan Cancer Registry (TCR) database and Taiwan’s National Health Insurance Research Database (NHIRD).
Data source
This study obtained data recorded between 2007 and 2014 from the TCR database, and between 2001 and 2014 from the NHIRD. The population-based TCR was established in 1979. After the Cancer Control Act was promulgated in 2003, all hospitals were mandated to submit cancer data to the TCR, and the completeness achieved was 97% (17). The TCR database comprises information on demographic data, dates of cancer diagnosis, primary site, histopathology, and cancer treatments. Taiwan National Health Insurance was established in 1995 and includes 99% of the entire population of Taiwan (23.74 million). The NHIRD comprises information on demographic data, dates of clinical visits, diagnostic codes, prescription medications, and treatment procedures. Individual identifiers were encrypted in the TCR database and the NHIRD in order to protect privacy. The International Classification of Diseases for Oncology, 3rd revision (ICD-O-3) and the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) were used for diagnostic codes. The Institutional Review Board of Cardinal Tien Hospital approved this study (approval number CTH-106-3-5-046), and informed consent was waived because the personal information obtained from the TCR database and the NHIRD was de-identified.
Study participants
Patients with skin cancers (ICD-O-3: C44) were identified between 2007 and 2014 from the TCR database. The cancers included were: BCC, SCC, sarcomas, malignant tumours of skin appendages, Merkel cell carcinoma, and melanoma. Carcinoma in situ and lymphoma were not included. Exclusion criteria were: patients who had incomplete data, age < 20 years at skin cancer diagnosis, or who had had any previous cancer before enrolment.
Screened skin cancer data were linked to the NHIRD and patients with skin cancer were then classified into 3 study groups (OTRs, chronic dialysis, and CKD) and the control group. OTRs were defined by at least 3 outpatient diagnoses (ICD-9-CM 996.8, V42.0, V42.1, V42.6–V42.9) and at least 90-day immunosuppressant prescription before skin cancer diagnosis. Patients with diagnostic codes of organ transplantation and a less than 90-day immunosuppressant prescription were excluded. Patients on chronic dialysis were defined as follows: undergoing at least 3 months’ haemodialysis or peritoneal dialysis and not having received organ transplantation before skin cancer diagnosis. Patients with CKD were defined as follows: at least one inpatient discharge diagnosis or 3 outpatient diagnoses codes of the following: ICD-9-CM 250.4, 274.1, 283.11, 403, 404, 440.1, 442.1, 447.3, 572.4 and 580–588 (which includes diabetic nephropathy, gouty nephropathy, hypertensive nephropathy, atherosclerosis/aneurysm/hyperplasia of the renal artery, haemolytic uraemic syndrome, hepatorenal syndrome, nephrotic syndrome, glomerulonephritis and other nephritis, renal failure, and renal sclerosis) (16) and had not commenced dialysis or renal transplantation before the diagnosis of skin cancer. Patients who did not meet the diagnostic criteria of the aforementioned study groups were referred as the control group. The control group was defined as patients who did not have chronic renal disease and had never received organ transplantation.
Outcome measurement and potential confounding factors
The main outcomes of this study were the histological subtypes and clinical characteristics of skin cancers in the study groups and control group. Factors that might confound the results were adjusted in the statistical analysis. Sex, age, geographical regions, use of immunosuppressive agents, and Charlson Comorbidity Index (CCI) scores served as the confounding factors. Geogra-phical regions were divided into northern or southern Taiwan by the Tropic of Cancer, which runs through the centre of Taiwan; therefore, the northern and southern areas of Taiwan receive different amounts of ultraviolet radiation. Immunosuppressant users were defined as those with ≥ 30 days of use, and non-users were defined as those with no or < 30 days of use one year before skin cancer diagnosis. Romano-CCI scores (18) were used as a summary measure of health status (17 comorbidities included) for the adjustment of comorbidities that might confound the results. Many immune-related conditions, such as rheumatological disease, lymphoma, leukaemia, and AIDS, were included in the Romano-CCI scores. There were no patients with lymphoma or leukaemia in this study because patients with any previous cancer before enrollment were excluded. CCI scores were calculated using at least one inpatient diagnosis or 3 outpatient diagnoses one year before skin cancer diagnosis.
Statistical analysis
The χ2 test, Fisher’s exact test, and Student’s t-test, when appropriate, were used to compare the distribution of demographic characteristics, histological types, and anatomical sites of skin cancers between study and control groups. Generalized estimating equation (GEE) regression model was performed to assess the difference in the proportion of certain histological types in total skin cancers in each study group compared with that in the control group, and to assess the independent effects of potential confounding factors. Adjustment for potential confounding factors was performed in all models. Differences between the groups were considered significant if 2-sided p-values were < 0.05. All statistical analyses were performed using SAS statistical software (SAS System for Windows, version 9.3, SAS Institute, Cary, NC, USA).
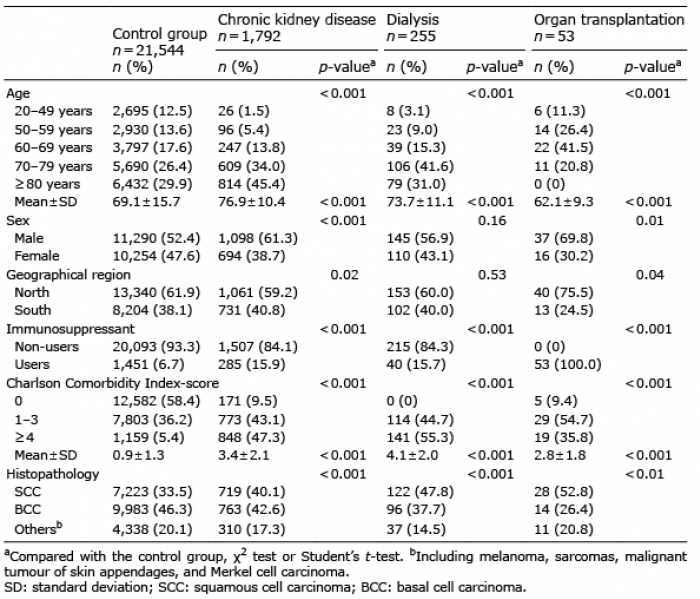
A total of 23,644 adult patients with skin cancer identified from the TCR database were enrolled in this study. Patients with skin cancer were divided into the following 4 groups: 53 OTRs (36 renal and 17 other organ (heart, lung and liver) transplant recipients), 255 patients on chronic dialysis (239 on haemodialysis and 16 on peritoneal dialysis), 1,792 patients with CKD, and 21,544 patients who served as the control group. The demographic characteristics of the study and control groups are listed in Table I. Among patients with skin cancer, OTRs were younger, and patients on chronic dialysis and those with CKD were older than the control group (all p < 0.001). Regarding histological subtypes, BCC and SCC were the first and second common subtypes in the control group and account for 46.3% and 33.5% of total skin cancers, respectively. The proportions of SCC in total skin cancers were elevated in all study groups, which were 52.8%, 47.8% and 40.1% in OTRs, chronic dialysis and patients with CKD, respectively. The SCC to BCC ratios were 2:1, 1.3:1, 1:1.1, and 1:1.4 in OTRs, patients on chronic dialysis, CKD patients, and the control group, respectively. Melanoma and NMSC other than BCC and SCC were combined in a group because the case numbers of each subtype were quite small.
Table I. Demographic characteristics of patients with skin cancers
A GEE model was used to assess the difference in the proportion of SCC in total skin cancers in each study group compared with that in the control group, and to identify the independent risk factors. Multivariate GEE analysis showed a higher proportion of SCC in OTRs (relative risk (RR) 1.99; 95% confidence interval (CI) 1.33–2.85; p < 0.001) and in patients on chronic dialysis (RR 1.25; 95% CI 1.03–1.50; p = 0.02) compared with the control group, after adjustment for age, sex, geographical regions, immunosuppressant users or not, and CCI scores. The proportion of SCC was stable in patients with CKD compared with the control group, after adjustment for potential confounding factors. In addition, other risk factors associated with a higher proportion of SCC in total skin cancers included old age (age ≥80 years vs. age 20–49 years, 2.77–2.82-fold risk), male sex (male vs. female, 1.09–1.10-fold risk), and south Taiwan residency (south vs. north, 1.11–1.12-fold risk). These findings were consistent in the 3 multivariate models. However, in the univariate models, immunosuppressant users and patients with high CCI scores were associated with a higher proportion of SCC in total skin cancers compared with non-users and those with low CCI scores. These effects were not significant in the multivariate models (Table II).
Table II. Relative risk (RR) and 95% confidence interval (95% CI) for the factors associated with the proportion of squamous cell carcinoma (SCC) in total skin cancers among each study group and the control group using generalized estimating equation (GEE) regression model
Fig. 1 shows the adjusted RR for the proportion of SCC in each study group compared with the control group after stratifying by sex, age group, geographical regions, immunosuppressant users or not, and CCI scores. In OTRs, all subgroups showed a higher proportion of SCC compared with the control group, except for patients aged ≥ 70 years and CCI score ≥ 4. In patients on chronic dialysis, half of the subgroups showed a higher proportion of SCC compared with the control group. Patients aged < 70 years had a greater increased risk of SCC (1.59-fold) compared with the control group of the same age. Although the proportion of SCC in patients with CKD was similar to that in the control group, a higher proportion of SCC was noted in patients with CKD aged < 70 years (1.30-fold) and of immunosuppressant users (1.23-fold). Interactions between study groups and clinical parameters were estimated, and significant interaction was observed only with age (p = 0.02 in patients on chronic dialysis and p < 0.001 in patients with CKD).
Fig. 1. Adjusted relative risk (RR) and 95% confidence interval (CI) for proportion of squamous cell carcinoma (SCC) in total skin cancers stratified by clinical covariates in (A) organ transplant recipients, (B) patients on chronic dialysis, and (C) those with chronic kidney disease compared with the control group. CCI: Charlson Comorbidity Index. aAll organ transplant recipients are immunosuppressant users.
Table III shows the anatomical site distribution of SCC in study groups and in the control group. The head and neck were the most common anatomical sites of SCC in all groups. Compared with the control group, in OTRs SCCs were located more frequently on the head, neck and trunk, and less frequently on the limbs, although the difference was not statistically significant.
Table III. Anatomical site distribution in different groups among patients with squamous cell carcinoma (SCC)
The key finding of this study is a higher risk of SCC in OTRs and patients on chronic dialysis compared with the control group. To the best of our knowledge, this is the first study to show a greater increase in risk of SCC than BCC and other skin cancers in OTRs and patients on chronic dialysis in Asian populations. An increased risk of developing SCC than BCC and other skin cancers was also noted in patients with CKD age < 70 years compared with the control group, although it was not noted in total patients with CKD. This study also found that patients who were older (compared with younger patients), male (compared with female), and those residing in south Taiwan (compared with those residing in north Taiwan) had a higher risk of developing SCC than BCC and other skin cancer subtypes.
Many immune-related conditions are associated with greater increases in risk of SCC than BCC, suggesting that reduced immune surveillance may be especially important in the aetiology of SCC (2). The population of OTRs is the best-investigated population with respect to this topic. Caucasian OTRs are associated with a 65- to 250-fold risk of SCC and 10- to 16-fold risk of BCC (3, 4). Although the risk of skin cancer in OTRs has been well-studied in Caucasians, it is not completely understood in individuals of Asian ethnicity. Several hospital-based studies from Japan (7), Korea (9), China (10) and the USA (Asian immigrants) (13) show very few (0–6) cases of skin cancers in their series. Population-based studies from Taiwan reported that OTRs are at 2.14-fold increased risk of total skin cancers (11) and 2.3-fold increased risk of NMSC (12), respectively, compared with the general population, but information about the histological subtype of skin cancers is unavailable in these studies. A Japanese national questionnaire survey reported that 29 of 9,210 OTRs developed skin cancers (including carcinoma in situ); however, the histological subtype of skin cancers is also unknown in this study (8). In Taiwan, the SCC to BCC ratio in the general population is approximately 1:1.6 based on the TCR reports (19). The present study included 53 OTRs with skin cancers (excluding carcinoma in situ), and an elevated SCC to BCC ratio of 2:1 is observed. After adjustment for confounding factors, the proportion of SCC in total skin cancers in OTRs was 1.99-fold higher than in the control group.
The pathogenesis of SCC in OTRs involves a complex interaction of ultraviolet susceptibility and exposure, oncogenic human papillomavirus, and long-term utilization of immunosuppressants. Photocarcinogenesis is the result of both immunomodulatory and mutagenic effects of ultraviolet radiation. A high prevalence of ultraviolet light-associated mutations is detected in cutaneous SCC in OTRs. OTRs are more susceptible to oncogenic viruses than are the general population. Up to 90% of cutaneous SCCs in OTRs contain human papillomavirus DNA, compared with 11–32% in normal skin. Although human papillomavirus is the pathogenesis for SCC, it is not associated with BCC. Many immunosuppressive agents are potentially carcinogenic. Azathioprine has been found to sensitize cells to ultraviolet light-induced damage through the incorporation of a metabolite into DNA that generates reactive oxygen species on exposure to ultraviolet light. Cyclosporine has been shown to suppress p53-mediated cell death and result in carcinogenesis (3, 4, 20, 21).
In addition to OTRs, other immune-related conditions associated with increased SCC than BCC risk include haematological malignancies (2), primary immunodeficiencies (2), HIV infection with low CD4 counts (22), and immune-mediated inflammatory disorders, such as inflammatory bowel disease (23) and psoriasis (24). The present study found a higher
risk of SCC than BCC and other skin cancers in patients on chronic dialysis compared with the control group. In patients with CKD, the increased risk of SCC compared with that of BCC and other skin cancers is confined to patients age < 70 years. The higher risk of SCC in these populations is thought to be due to the uraemia itself, not related to their treatments such as ultraviolet phototherapy for uraemic pruritus (15, 16). The pathogenesis of SCC in patients on chronic dialysis and those with CKD is thought to be due to the accumulation of uraemic toxins, resulting in low-grade chronic inflammation. The intensity of chronic inflammation is positively associated with the stage of CKD and is maximum in patients on chronic dialysis (15, 16, 25, 26). Chronic inflammation produces reactive oxygen species that cause DNA damage and is involved at different stages of tumour development; that is, initiation, promotion, malignant conversion, invasion, and metastasis (27, 28). The studies regarding chemoprevention for skin cancers, showing that non-steroidal anti-inflammatory drugs are more effective in preventing SCC than BCC, also provide evidence that inflammatory conditions appear to be more closely linked to SCC than BCC (29, 30).
The present study also found that older patients, males, and those residing in south Taiwan (i.e. at lower latitudes) had a higher risk of developing SCC than BCC and other skin cancers in comparison with younger patients, female patients, and those residing in north Taiwan (i.e. at higher latitudes). The immune system in elderly healthy individuals and patients with renal failure shares many characteristics, such as preferential loss of cells belonging to the lymphoid cell lineage, non-resolving chronic inflammation (inflammaging), and DNA damage (26, 31, 32). The stronger relationship between inflammation and SCC than BCC might explain the greater risk of SCC than BCC in old age. The similarity of the immune system in old age and uraemic patients might also explain why the difference in risk of SCC between uraemic patients and the control group is greater in young age and less in old age. The sex-specific difference in the immune system might demonstrate the greater risk of SCC than BCC in men compared with women. Males generally experience higher rates of chronic inflammatory disease and greater ultraviolet radiation-induced immunosuppression. Sex hormones, genes encoded on the sex chromosomes, and sex-specific behaviours probably contribute to these differences (33, 34). The effect of geographical location (difference in solar radiation) has a stronger impact on the risk of SCC than the risk of BCC. As solar radiation is stronger in Australia than in the UK, Australians are more likely to develop SCC (SCC:BCC=1:2.5) than people in the UK (SCC:BCC=1:4) (1). Qureshi et al. indicated that the risk of SCC is greater for women in the USA who live in states with high levels of ultraviolet radiation than those in states with low levels of ultraviolet radiation. The gradient of risk is weaker for BCC (35).
This study found that, in OTRs, SCCs are more commonly located on the head, neck and trunk and less commonly located on the extremities compared with the control group, although the difference is not statistically significant. A Swedish study by Lindelöf et al. (36) reported that the head and neck were the predominant sites of SCC in male OTRs, and the trunk was the predominant site of SCC in female OTRs. The most common site in younger OTRs was the chest and, in older OTRs, the face. Hartevelt et al. (5) found that 97% of SCCs in Dutch OTRs were located on the sun-exposed areas, with a preference for the back of the hands and face. The difference in anatomical locations of SCC between different studies might be an interaction among genetics, sun exposure habits, human papillomavirus infection, and types of immunosuppressant used.
The strength of this study is that the completeness of the TCR from 2007 to 2011 is 97% and is increasing (17), and the Taiwanese NHIRD covers 99% of Taiwanese residents, thus enabling a true population-based design and avoiding selection bias and referral bias. The study has several limitations that should be considered. First, OTRs and uraemic patients may receive more medical surveillance than the general population. Under strict skin surveillance, the detection of skin cancers of all histological subtypes would be increased equally. Therefore, the increased risk of SCC compared with risk of other skin cancers observed in this study could not be caused by medical surveillance. Secondly, the number of skin cancers in OTRs is small, which might reduce the power of statistical analysis. Thirdly, although CCI scores for comorbidities were adjusted in the multivariate models, certain immune-related conditions might be unadjusted and confound the results. Finally, the external validity of our findings may be a concern, because almost all of the enrolees were Taiwanese (of Asian race). The generalizability of the current results to other non-Asian racial groups requires further verification.
In conclusion, this study reveals that OTRs, patients on chronic dialysis, older patients, males, and residents of south Taiwan (which has a high level of solar radiation) have a higher risk of developing SCC than other skin cancer subtypes.The study provides aetiological insights into the development of SCC, and highlights that physicians should be aware of the higher risk of SCC in these conditions.
This work was financially supported by research grants provided by Cardinal Tien Hospital, New Taipei City, Taiwan (grant CTH107A-2A08); and Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan (grant 108-wf-eva-12).


 Click to show fullsize
Click to show fullsize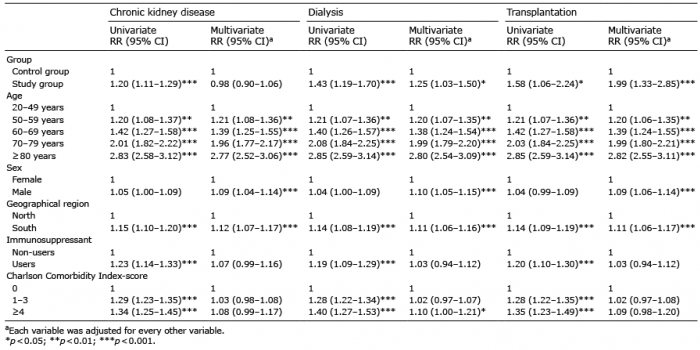 Click to show fullsize
Click to show fullsize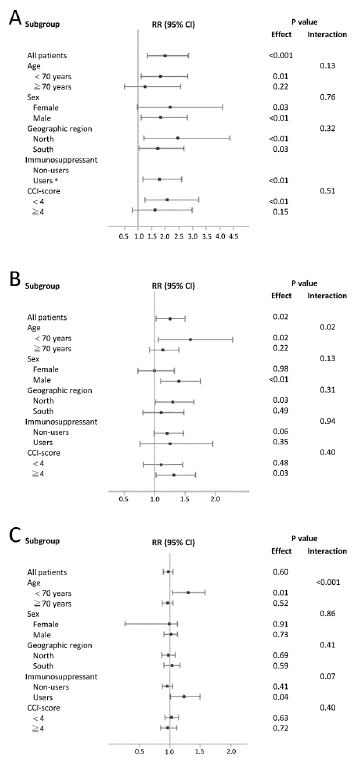 Click to show fullsize
Click to show fullsize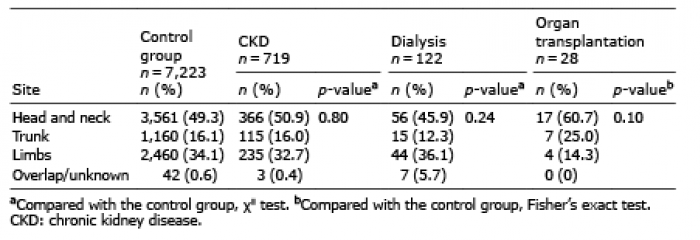 Click to show fullsize
Click to show fullsize