


Department of Dermatology, University Hospital of Brest, FR-29200 Brest, France. *E-mail: laurent.misery@chu-brest.fr
Accepted Oct 17, 2019; Epub ahead of print Oct 18, 2019
Acta Derm Venereol 2020; 100: adv00036
Acne fulminans is a difficult condition to manage, and there is an absence of large-scale randomized controlled trials evaluating treatment for this condition. In addition, there is an absence of large-scale randomized controlled trials evaluating treatment for acne fulminans. A review of case series, individual reports, and case analyses supports the use of systemic corticosteroids in combination with isotretinoin for treating acne fulminans (1). However, other treatments are needed, especially when acne fulminans is induced by isotretinoin. We report here a case of isotretinoin-induced acne fulminans without systemic symptoms (IIAF-WOSS), which was treated successfully with oral dapsone.
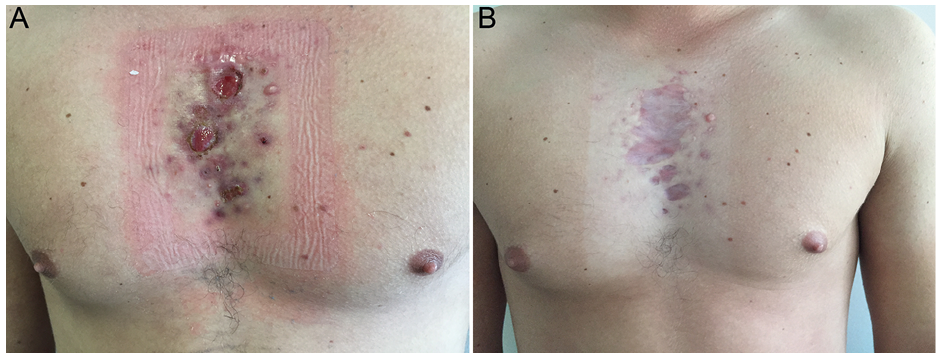
An 18-year-old man with nodulocystic acne affecting only his back was treated with isotretinoin, 30 mg daily, for 11 months. Nonetheless, he presented with an abrupt flare of inflammatory acne on his chest and back, with erosions and haemorrhagic nodules, which spared his face (Fig. 1A). There was no triggering factor other than the use of isotretinoin (in particular, the patient had not used testosterone or other anabolic steroids). There was no evidence to support diagnoses of the following syndromes: (i) pyoderma gangrenosum, acne and hidradenitis suppurativa (PASH); (ii) pyogenic arthritis, pyoderma gangrenosum and acne (PAPA); (iii) pyogenic arthritis, pyoderma gangrenosum, acne and hidradenitis suppurativa (PAPASH); or (iv) synovitis, acne, pustulosis, hyperostosis and osteitis (SAPHO). The diagnosis of IIAF-WOSS was retained. The dosage of isotretinoin was decreased to 10 mg daily and oral corticosteroids (prednisone) were started at 20 mg daily (0.5 mg/kg/day), with no success after 3 months.
Then the patient was reffered to our department, and we decided to discontinue isotretinoin and start oral dapsone, 100 mg daily, (allowed by the absence of no glucose-6-phosphate-dehydrogenase deficiency). Oral corticosteroids were decreased gradually, and then stopped 1 month later. Less than 2 months after starting treatment with oral dapsone, the patient felt very tired and a little short of breath. The patient’s methaemoglobinaemia level was too high (4%) and treatment was stopped. After rapid normalization of both methaemoglobinaemia and clinical symptoms, and because the lesions had clearly improved with treatment, the oral dapsone was recommenced at a lower dose, 50 mg daily, with no new adverse events. Complete remission was achieved after 8 months of treatment (Fig. 1B). Oral dapsone treatment was continued for 3 months at 50 mg daily. There was no relapse 2 years after stopping treatment.
Hence, in the current patient, treatment with oral dapsone resulted in complete remission with no relapse. The high level of methaemoglobinaemia probably occurred because the dosage of dapsone was not adjusted for the patient’s low weight (approximately 50 kg).
The current patient presented with sudden late-onset IIAF-WOSS. As described previously (2), such patients have skin lesions like those in the current case, with no biological or systemic manifestations.
Fig. 1. (A) Lesions on the torso before treatment with dapsone. (B) Healing of acne fulminans, with residual scars, after 6 months of treatment with dapsone.
Oral dapsone is not commonly used in the treatment of acne, but this case shows it could be effective in the treatment of severe acne recalcitrant to other systemic drugs. The 2 major adverse effects are haemolytic anaemia and methaemoglobinaemia, which are dose-dependent. However, because of its anti-inflammatory action, oral dapsone is used in some inflammatory dermatosis, such as pyoderma gangrenosum and hidradenitis suppurativa.
There are a few published case reports of acne fulminans responding to oral dapsone. In other cases, dapsone was given in association with oral corticosteroids (3, 4), isotretinoin (5) or prednisone and cyclosporine (6). In Japan, where systemic isotretinoin is not authorized because of its teratogenicity, there are reports of 4 cases of severe acne being treated successfully with oral dapsone, 50 mg daily (7). A case of nodulocystic acne that did not improve with oral isotretinoin, but which responded to oral dapsone, 300 mg daily (which is an unusually high dosage) was also reported (8).
Evidence-based recommendations for the management of acne fulminans and its variants have been published recently (1). Because oral dapsone has been used successfully in a small number of cases, dapsone is proposed as an alternative treatment when acne fulminans is not sufficiently improved with isotretinoin and oral cortico-steroids (1); however, there is a need to report new cases to support this alternative use.


 Click to show fullsize
Click to show fullsize