


1DDL Diagnostic Laboratory, Rijswijk, 2Centre for Human Drug Research, Zernikedreef 8, NL-2333CL Leiden, 3Department of Dermatology, Erasmus Medical Center, Rotterdam, 4Leiden Academic Center for Drug Research, Leiden University, 5Leiden University Medical Center, 6Department of Medical Microbiology, Alrijne Hospital, Leiden, The Netherlands, and 7Cutanea Life Science, Wayne, Pennsylvania, USA, The Netherlands. E-mail: rrissmann@chdr.nl
#These authors contributed equally to this work.
Accepted Nov 19, 2019; E-published Nov 19, 2019
Acta Derm Venereol 2020; 100: adv00018.
Atopic dermatitis (AD) is a common chronic, inflammatory skin disorder associated with Staphylococcus aureus colonization and reduced microbiota diversity (1–3). New treatments are being evaluated using clinical AD scores and skin microbiota composition (4–8). Most study designs include the collection of a single sample before and after treatment. The aim of the current evaluation was to analyse inter- and intra-patient variability of the skin microbiota of patients with AD over time to determine whether limited sampling is sufficient to capture the full extent of variability in the skin microbiota.
Microbiological test results of skin swabs and clinical data from the placebo group of 2 phase 2 clinical trials were used in this evaluation (see Appendix S1 for details). Briefly, lesional and non-lesional skin microbiota of patients with AD were analysed weekly over a period of 42 days. Data from 20 patients with a mean ± standard deviation age of 24 ± 5 years and clinical AD score (objective-SCORing Atopic Dermatitis: oSCORAD) of 21.1 ± 5.6 in the initial clinical trial (ClinicalTrials.gov: NCT03091426) were used to determine the variability in skin microbiota.
The coefficient of variation (CoV) represents the extent of variability in relation to the mean of the population. The CoV was calculated for microbial diversity (Shannon diversity index), relative abundance of Staphylococcus spp. and S. aureus concentration (culture and qPCR). A CoV ≤ 25% has been considered as an acceptable level of variation (9, 10). To quantify the extent of inter-patient variability of the skin microbiota, the CoV was calculated at each time-point for all test results. For lesional skin, high CoVs were observed, in the range 35.5–45.9% for microbial diversity, 46.9–57.3% for relative abundance of Staphylococcus spp., and 45.3–94.1% for S. aureus concentration. For microbial diversity of non-lesional skin, low CoVs, in the range 16.3–28.0%, were found. These data strongly indicate that there was considerable variation in lesional skin microbiota between patients.
To analyse the skin microbiota variability within an individual patient over time, the CoV for microbial diversity, relative abundance of Staphylococcus spp. and S. aureus concentration was calculated per patient. For all test results of lesional skin, CoVs ranging between 7.1% and 173% were observed. For microbial diversity of non-lesional skin, low CoVs, ranging between 3.5% and 29.3%, were found. These data indicate that there was a wide range of intra-patient variability in lesional skin microbiota.
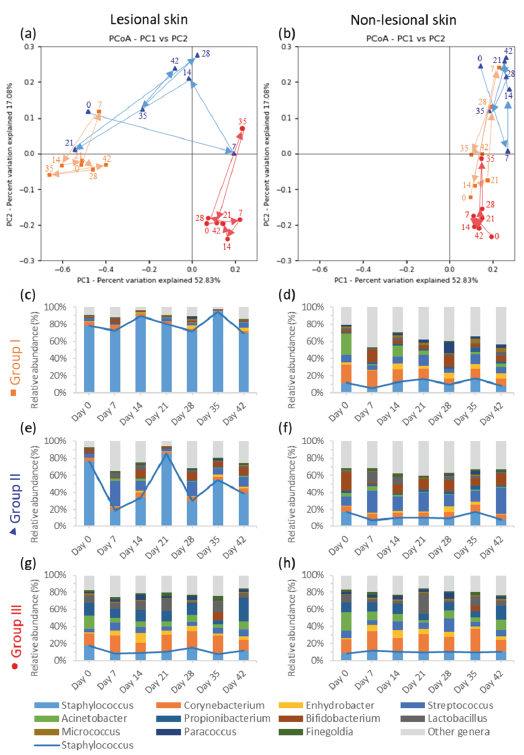
The patient population could be divided into 3 groups with different microbiological phenotypes, as shown by 3 representative patients in Fig. 1. The lesional skin microbiota of group I (orange) and II (blue) were dominated by Staphylococcus spp., resulting in a different profile compared with their non-lesional skin microbiota. These groups differed in variability, as the lesional skin microbiota of group II was relatively unstable (Fig. S1). The lesional skin microbiota of group III (red) was not dominated by Staphylococcus spp. Its composition and variability were similar to their non-lesional skin microbiota. This group had significantly higher microbial diversity (p < 0.001), lower relative abundance of Staphylococcus spp. (p < 0.001), lower S. aureus concentration (p < 0.001) and lower oSCORAD (p = 0.032) compared with groups I and II.
Data from a separate clinical trial (ClinicalTrials.gov: NCT02456480) with a comparable study population, consisting of 12 patients with an age of 25 ± 11 years and oSCORAD of 19.0 ± 7.4, was used for verification purposes. This second sample set confirmed the large inter- and intra-patient variability for lesional skin (Tables SI–SIII, Fig. S2).
Fig. 1. Lesional and non-lesional skin microbiota of 3 selected patients representing 3 groups of patients with different microbiological phenotypes shown in (a, b) principal coordinates analysis (PCoA) plots and (c–h) bar charts. In the PCoA plots, the arrows combined with the day numbers show how the microbiota composition changed over time.
To our knowledge, this is the first longitudinal analysis of inter- and intra-patient variability of skin microbiota of patients with AD. While the sampling method was strictly standardized, large inter- and intra-patient variability for lesional skin microbiota were found. The large inter-patient variability originated from variable S. aureus abundance and environmental factors that vary significantly among humans (11, 12). The wide range of intra-patient variability indicated that the skin microbiota of some individuals varied more than others. Three patient groups with different microbiological phenotypes were defined. Groups I and II could be described as high Staphylococcal bioburden, low microbial diversity and either microbiologically stable, or unstable, respectively. The observation that the variability within each of these 2 groups is consistent within subjects across longitudinal samples, as well as concordant in multiple microbiological assessments, suggests that this difference is not caused by variable sample quality. This difference might be caused by the same unidentified individual (genetic) factors that determine the degree of variability of healthy skin microbiota (13, 14). Group III was characterized by a significantly different lesional microbiota compared with groups I and II. It could be described as low Staphylococcal bioburden and high microbial diversity. The relative lack of dysbiosis was associated with lower oSCORAD.
Because the variability over time can be high, limited sampling may not be sufficient to determine the effect of the treatment on an individual’s lesional skin microbiota. High sample frequency and statistical analyses methods, which utilize repeated measures across more than one end-of-study time-point, may reduce the effect of the variability in the analyses of clinical trials. The ability to objectively classify subjects to the microbiological phenotypes could be useful in the analyses and interpretation of microbiota data in future clinical trials with larger sample sizes.
The limitation of the presented evaluation is that the patients administered a vehicle gel on the lesions. This could have had an influence on the lesional skin microbiota as it contains the preservative sodium benzoate. However, this was considered to be minimal because the concentration was far below the minimal inhibitory concentration for S. aureus. Another limitation is the small patient group and the omission of including patients of younger age. A larger and more diverse population is required to study the microbiological phenotype classifications and generalize more broadly.
In conclusion, this evaluation shows that lesional skin microbiota of patients with AD is characterized by large inter- and intra-patient variability, reflecting a highly individual profile. A high sample frequency, e.g. once weekly, yields excellent time-dependent insight into the changes in the variable skin microbiota, which can be used to determine the treatment effect on the lesional skin microbiota in clinical trials.
The authors are grateful to Esmeralda Bosman, Angela Hoogenboom, Michiel Weber and Anne Hout of DDL Diagnostic Laboratory, and Dr Karen Broekhuizen of Centre for Human Drug Research for their contribution. The clinical trials were sponsored by Cutanea Life Sciences, Inc.
Conflicts of interest: LJD and WQ are shareholders of DDL Diagnostic Laboratory. GF was an employee of Cutanea Life Sciences at the time the investigations were conducted. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize