


1LEO Innovation Lab, Silkegade 8, DK-1113 Copenhagen, 2Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, Hellerup, and 3Clinic of Gynaecology Taastrup, Taastrup, Denmark. E-mail: anders.schultz@yahoo.dk
Accepted Nov 27, 2019; E-published Nov 27, 2019
Acta Derm Venereol 2020; 100: adv00021
Psoriasis is a chronic inflammatory and hyperproliferative skin disorder with a prevalence of approximately 2–3% in the western world (1). Insulin levels are influenced by factors such as diet and lifestyle, and since insulin possesses both pro-inflammatory and hyperproliferative effects, it may play a role in the pathogenesis of psoriasis (2–4). It has been shown that weight loss in obese patients with psoriasis may positively affect the severity of the skin disease (5). A study including women with polycystic ovary syndrome showed that a high protein-to-carbohydrate (HP) diet, with protein accounted for at least 40% of the energy, 30% was derived from fat, and the rest from carbohydrates, resulted in greater weight loss and reduced insulin production compared with a normal control diet (6). The HP group reduced their weight and C-peptide levels (indicative of pancreatic insulin production) (7). Based on these studies, the balanced protein-to-fat-to-carbohydrate ratio (PFC) diet, was developed. The PFC diet is an insulin-lowering iso-caloric, ad libitum, diet in which protein accounts for 33% of the total energy, 33% of the total energy is derived from carbohydrates, and 33% from fat.
The aim of this study was to investigate the effects of a PFC diet on the severity of psoriasis.
The study was a 24-week prospective, investigator blinded, randomized controlled study with 2 parallel arms. Inclusion criteria were: patients with psoriasis who were at least 18 years old and able to speak and read Danish. The participants needed to have at least 2 palms of psoriasis and were allowed to use topical anti-psoriatic treatment. However, individuals who received systemic anti-psoriatic treatments (biologics, methotrexate, etc.), and those with diabetes were excluded. Study participants were recruited via Facebook and pre-screened for eligibility using online questionnaires (at www.kopso.dk, Studies & Me, Copenhagen, Denmark). All consultations and study meetings were held at the Department of Dermatology, Gentofte Hospital, University of Copenhagen, Denmark.
Participants were randomized using the rank-minimization method (8), and allocated to either the PFC diet or a control group (continuing their usual diet).
Because of the dietary changes required of the participants in the PFC group, they were expected to attend 2 group sessions with the study dietician. The participants received a book (9) explaining the principles of the PFC diet, as well as tips, and recipes. The first visit took place at baseline, while the second was held 14 days later, allowing for elaboration, and clarifications, if necessary.
The primary endpoint was the Psoriasis Area and Severity Index (PASI) assessed by the study dermatologist at baseline, week 12, and finally at week 24. Secondary endpoints were body mass index (BMI), and selected blood markers, including glycated haemoglobin (Hba1c), C-peptide, total cholesterol (TC), high- (HDL), low- (LDL), and very low-density lipoproteins (VLDL), triglycerides (Department of Clinical Biochemistry, Herlev and Gentofte Hospital, Gentofte, Denmark).
Sample size was calculated to 60 participants when anticipating a 10% dropout. Dichotomous and continuous data on baseline characteristics were analysed using χ2 and unpaired t-test, respectively. Similarly, an unpaired t-test was used for group comparisons of changes in blood markers at 12 and 24 weeks, respectively. To test the changes in PASI over time, 1-way analysis of variance (ANOVA). was used. The study was approved by the Danish Capital Region Ethical Committee (study ID: H-16036835), and by the Danish Data Protection Agency. The study was performed in accordance with the Declaration of Helsinki II. Each participant signed an informed consent document before the start of the study.
After pre-screening, 115 people were eligible for participation in the study. However, some people lived a long way from the hospital and therefore declined to participate (n = 21), and others did not attend or declined to participate (n = 32), while others were excluded for having too mild psoriasis (n = 37). A final total of 25 people remained for inclusion and randomization. Of these, 13 were allocated to the PFC diet (Table I).
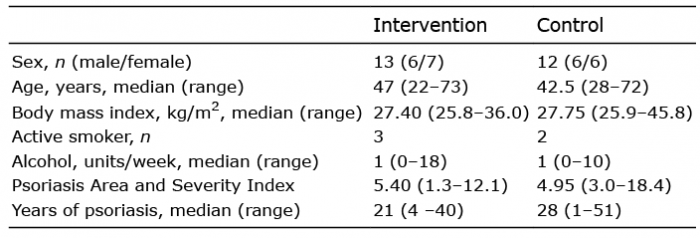
Table I. Demographics at baseline
Participants in the PFC group were comparable with those in the control group with regards to demographics and other baseline measurements.
After 12 weeks, 7 participants had dropped out of each group. After 24 weeks, only 4 participants remained; 2 in each group. Of these, only 3 had a complete set of blood samples for analysis (Fig. 1). There were no adverse effects during the study. Due to the high rate of dropout the trial was stopped.
Fig. 1. Consort diagram.
PASI was identical in the groups at weeks 12 and 24. No difference in PASI from baseline to 12 weeks or end-of-study was found in either group. In the PFC group, 1 of the 2 completers went from a PASI of 5.8 (baseline), to 5.6 and 3.6 at weeks 12 and 24, respectively, while the other remained the same during the study (PASI 2.6). In the control group, one completer showed an improvement in PASI during the study, from 7.3 at baseline to 6.3 and 0.4 after 12 and 24 weeks, respectively, while the other remained the same during the study (PASI 18.4).
Due to the low number of participants completing the 24 weeks follow-up, only the results at week 12 could be analysed. At week 12 there were no differences between the groups with regards to HbA1c, C-peptide, TC, HDL, LDL, VLDL, triglycerides, TC:HDL ratio or triglycerides:HDL ratio.
This study showed that patients with psoriasis can be recruited using digital recruitment strategies. Due to an excessive dropout rate, the study lost all statistical power, thus no meaningful conclusions could be drawn about the effect of the PFC diet on the severity of psoriasis. None-theless, using a similar HP diet, others have shown that such a diet may have a positive effect with a potential to reduce weight and lower circulating insulin levels (6). With regard to retention rate, one could hypothesize that the high dropout rate was due to the mildness of the skin disease; however, in the study by Jensen et al. (5), the participants had similar mean PASI at baseline, but the retention rate after more than 60 weeks remained high, at 50. Jensen et al. (5), however, primarily recruited patients from their outpatient clinic, which might have made participation more convenient. The study showed that weight reduction may have an effect on the severity of psoriasis, and that such an effect may be maintained in the long-term.
The dropout rate emphasizes the need for a different study design in order to maximize the retention rate. Haste et al. (10) have shown that a digital weight loss intervention over a 12-month period including 20 digital consultations with a dietitian as well as digital interaction with other participants improved the retention rate in men with type 2 diabetes compared with conventional care. The present study also lost a lot of pre-screened individuals. Katz et al. (11) have recently shown that digital patient recruitment could save recruitment time, and hence decrease the overall study duration if investigators engage patients within 24 h. In the current study, the sub-investigator response time lasted up to 2 months.
In conclusion, future studies may benefit from digital recruitment; however, the time from online sign-up to first visit at site must be as short as possible. Regarding retention, digital solutions enabling the participants to participate remotely may be of interest. Due to the high rate of dropout in the current study, no meaningful conclusions could be drawn about the effect of the PFC diet on the severity of psoriasis.
Conflicts of interest: ANØS, JRZ and MM-M are employed by LEO Innovation Lab, an independent unit under LEO Pharma A/S. None of the authors received any payment, the study expenses were cover by LEO Innovation Lab.


 Click to show fullsize
Click to show fullsize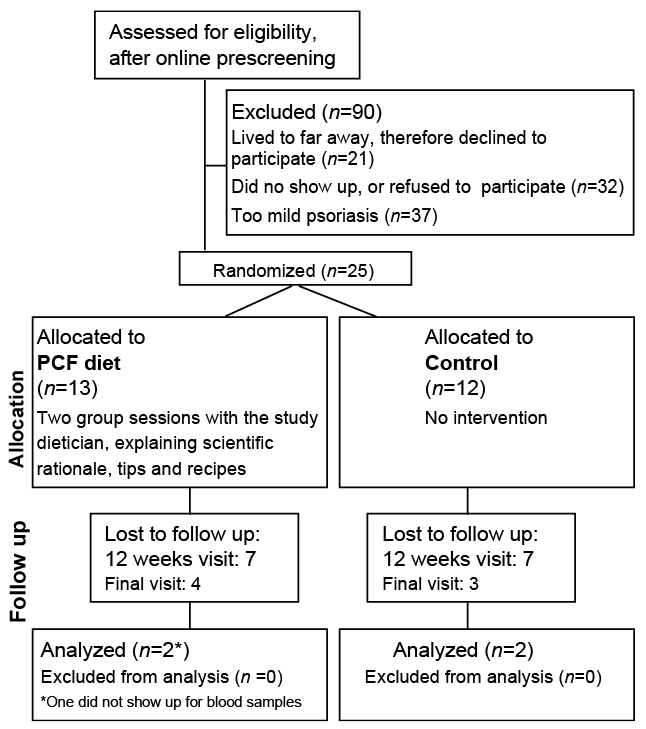 Click to show fullsize
Click to show fullsize