


1Department of Dermatology, University of Montpellier & Montpellier University Hospital, 80 avenue Augustin Fliche, Montpellier Cedex 5, and 2Department of Medicine, Saint Louis University Hospital, Saint Pierre, Réunion, France. E-mail: e-schwob@chu-montpellier.fr
A woman in her 40s with no significant medical history was referred for recurrent itchy and erythematous plaques on her trunk and the outer side of her arms and thighs, exclusively occurring after scuba diving (Fig. 1). She had been diving for 20 years and had experienced these symptoms for 8 years. The episodes resolved spontaneously within a few hours of finishing a dive. She usually ate wheat-based food before diving. After an initial diagnosis of symptomatic dermographism, she noticed a partial improvement if she took H1-antihistamines before diving. She had reported a single episode of dizziness, characterized by blurred vision, headache and marbled flanks, 5 years previously. On physical examination, no skin lesion was visible. Testing for dermographism with a FricTest® was positive 2+.
What is your diagnosis? See next page for answer.
Fig. 1. Erythematous plaques of the peri-umbilical area occurring immediately after scuba diving.
Acta Derm Venereol 2020; 100: adv00130.
Diagnosis: Skin decompression sickness
Blood count, thyroid stimulating hormone (TSH), anti-thyroid antibodies, antinuclear factors, basal tryptasemia and omega-5-gliadin-specific IgE were normal or negative. Provocation tests for inducible urticarias (delayed pressure urticaria, cholinergic urticaria, cold contact urticaria, etc.), and skin-prick tests with a piece of her diving suit, were all negative. Brain magnetic resonance imaging (MRI) revealed a sequel of a left cerebellar stroke, and a transoesophageal echocardiography revealed the presence of a patent foramen ovale (Fig. 2). Scuba diving was therefore contraindicated because of the risk of neurological decompression accident.
Decompression sickness is a result of gaseous bubble formation in tissues, or in venous or arterial circulation, during or after a reduction in environmental pressure (decompression), generating ischaemic tissue accident and endothelial dysfunction. Symptoms depend on the anatomical area in which bubbles block the circulation and on the degree with which the tissue reacts to this ischaemia and inflammation (1). Skin decompression sickness is rare (9–10% of all cases of decompression sickness), cutaneous manifestations are poorly reported and often considered benign, and are neglected by recreational divers, whereas some of these manifestations may be due to arterial decompression sickness. Skin lesions may present as: “fleas”, erysipelas, scarlatiniform exanthema, emphysema, and sometimes present as red-bluish spots, often itchy or painful and associated with a sensation of swelling, evolving to a cutis marmorata (skin mottling) located in the peri-umbilical area, shoulders and buttocks (2). Their physiopathology may be explained by either vascular occlusion of skin vessels by bubbles entering the arterial circulation through a right-to-left shunt (3, 4) for cutis marmorata or bubble formation due to saturated subcutaneous tissue for the other subsets, during decompression (5). The partial improvement of symptoms with H1-antihistamine, which has not been reported previously, may have represented only the positive effect on dermographism in this patient, thus it could dangerously mask the cutaneous signs of decompression sickness. Cutis marmorata skin decompression sickness should no longer be considered a mild, innocuous form, since it is often associated with a neurological complication, and should therefore be treated accordingly. It is recommended to investigate for a right-to-left shunt by a transcranial Doppler in case of skin manifestation of decompression and a brain MRI should be performed if a malaise (characterized by hypotension, headache, blurred vision and sometimes fainting) has occurred. Dermatologists should be able to recognize skin decompression sickness, as skin manifestations are sometimes the first and only sign of this condition.
Fig. 2. Transoesophageal echocardiography with and without bubble injection revealing patent foramen ovale in the patient. FO: foramen ovale; LA: left atrium; LR: right atrium.


 Click to show fullsize
Click to show fullsize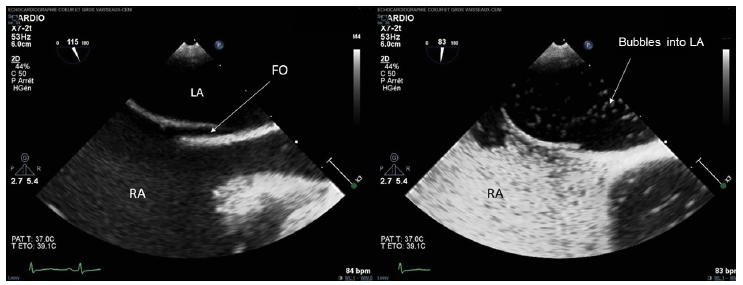 Click to show fullsize
Click to show fullsize