


1Department of Dermatology, Sheba Medical Center, Tel-Hashomer, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, 2Medical Corps, Israel Defense Forces, Tel-Hashomer, 3Department of Military Medicine, Hebrew university of Jerusalem, Faculty of Medicine, Jerusalem, 4Department of Medicine and the Dr Pinchas Bornstein Talpiot Medical Leadership Program, Sheba Medical Center, Tel Hashomer, 5Department of Dermatology, Tel-Aviv Sourasky Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, and 6Department of Dermatology, Hadassah-Hebrew University Medical Center, Jerusalem, Israel
#These authors contributed equally to this study.
Few studies have reported an association between psoriasis and atopic comorbidity in adults. A population-based cross-sectional study was performed to investigate the possible association of psoriasis with allergic rhinitis or asthma among adolescents. Adole-scents (16–18 years of age) medically evaluated for military service between 1999 and 2014 were included. Medical records were obtained from the database of the Israeli Defense Forces. Of the 887,765 adolescents studied, 3,112 patients had psoriasis (56.1% mild; 43.9% moderate-to-severe). Psoriasis was significantly associated with allergic rhinitis (adjusted odds ratio (aOR) 1.3; 95% con?dence interval (CI) 1.2–1.5) and asthma (aOR 1.2; 95% CI 1.0–1.3), compared with controls without psoriasis. Moderate-to-severe psoriasis was associated with allergic rhinitis (aOR 1.3; 95% CI 1.1–1.5) and asthma (aOR 1.5; 95% CI 1.2–1.7), while mild psoriasis was only associated with allergic rhinitis (aOR 1.4; 95% CI 1.2–1.6). In conclusion, amongst adolescents, psoriasis was found to be associated with allergic rhinitis and asthma.
Key words: psoriasis; adolescents; atopic comorbidity; allergic rhinitis; asthma.
Accepted Apr 21, 2020; Epub ahead of print Apr 21, 2020
Acta Derm Venereol 2020; 100: adv00133.
Corr: Eran Galili, Department of Dermatology, Sheba Medical Center, Tel-Hashomer, Ramat Gan, Israel. E-mail: egalily@gmail.com
In a population-based cross-sectional study among adole-scents, psoriasis was shown to be significantly associated with allergic rhinitis and asthma. The association between psoriasis and asthma was found only in moderate-to-severe psoriasis, while the association with allergic rhinitis was not dependent on psoriasis severity.
The pathophysiology of psoriasis involves a T helper (Th)1 and a Th17 inflammatory response, while atopic diseases, including allergic rhinitis and asthma, have strong Th2 inflammatory responses (1, 2). Recent research on both conditions suggests complex inflammatory responses involving additional mediators. These mediators include Th22-cells and T-helper subtypes that express distinct immunological phenotypes (2–8).
There are limited data regarding the clinical linkage between psoriasis and allergic rhinitis and asthma. Only a few studies have reported an association between psoriasis and asthma among adults (9–11). Whether allergic rhinitis is associated with psoriasis is unknown, as data is lacking. Extrapolating findings from adult studies onto children and adolescents would be inaccurate, since both childhood psoriasis, allergic rhinitis, and asthma have been shown to differ substantially from their adult type, with differences in disease prevalence and immunological phenotype (3, 7, 12–14).
In adolescents, allergic rhinitis and asthma are common (15, 16). Moving from adolescence to early adulthood, allergic rhinitis remains highly prevalent, while asthma gradually declines (15). In adolescent years, the prevalence of allergic rhinitis ranges between 8% and 14%, and asthma ranges between 8% and 10% (17, 18).
Although allergic rhinitis and asthma are widely prevalent among children and adolescents and decline in adulthood, data regarding the diseases’ association with psoriasis for these age groups was evaluated only in a single retrospective study (19).
The current study sought to examine the relationship between psoriasis and allergic rhinitis and asthma in adolescents in a large population-based study.
Characteristics of study participants and study design
This is a population-based cross-sectional study. In Israel, military service is mandatory. Prior to military service, all eligible male and female adolescents undergo medical assessment by a general physician specifically trained for evaluating candidates’ fitness for military service (20). This medical assessment is performed at the recruitment office and includes a medical interview, a comprehensive review of medical records obtained from the candidate’s civilian primary care physician, and a systematic physical examination, including an examination of the skin. Examinees with a known diagnosis of psoriasis, allergic rhinitis, or asthma are obliged to provide a documented diagnosis made by a relevant specialist (dermatologist, pulmonologist, otolaryngologist or allergist) stating their current disease status and their current medical treatment. Examinees suspected of having an undiagnosed medical condition at the time of medical assessment are referred for further medical evaluation by the relevant specialist.
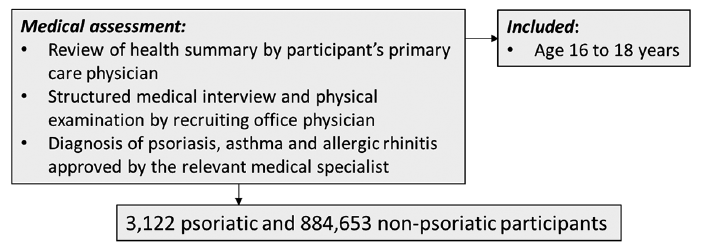
The database of the Israel Defense Force (IDF) was used to identify examinees with psoriasis. Of the 877,765 adolescents examined between 1 January1999 and 1 January 2014, a total of 3,112 examinees were diagnosed with psoriasis. Recruits without a diagnosis of psoriasis were assigned to the comparison group (n = 884,653). Participants’ assessment and designation is summarized in Fig. 1. In previously published studies by our research group, the same study population was used to investigate the association between psoriasis and metabolic and neuro-psychiatric comorbidity (21, 22). The inclusion criterion for the current study was age 16–18 years at the time of medical assessment. Detailed baseline characteristics retrieved from the medical assessment included age, sex, country of origin, number of siblings, body mass index (BMI) and socioeconomic status (SES) (20). Country of origin was classified by the father’s or grandfather’s country of birth. SES was drawn from records of the Israeli Ministry of the Interior based on the recruit’s place of residence on a scale of 1 (lowest) to 10 (highest) (23). Ethical approval for this study was obtained from the IDF Institutional Review Board.
Fig. 1. Participant assessment and designation.
Psoriasis: diagnosis and classification
The diagnosis of psoriasis was based on a clinical examination made by a dermatologist. Mild psoriasis and moderate-to-severe psoriasis were determined according to the subject’s status, as specified in Table I. This severity classification is based on the use of topical or systemic therapy, as was recently validated and in common use in registry-based studies (24).
Table I. Diseases diagnosis and classification
Allergic rhinitis and asthma: diagnosis and classification
Allergic rhinitis and asthma were diagnosed as shown in Table I. For allergic rhinitis, the diagnosis was determined by an otolaryngologist or an allergist. This diagnosis was for cases of chronic disease with a documented active episode during the last year. For asthma, the diagnosis was determined by a pulmonologist based on a clinical evaluation and diagnostic spirometry and challenge test examinations, as previously reported (25). Asthma was further sub-classified by severity according to the Global Initiative for Asthma (GINA) classification (26): non-persistent asthma included mild disease or disease in remission, and persistent asthma included moderate-to-severe disease.
Statistical analysis
The values in this study are presented as mean (standard deviation; SD) or number (percentage). Categorical variables were compared using a χ2 test and continuous variables were tested using an independent samples t-test. Univariate and multivariate logistic regression were used to describe the association of allergic rhinitis and asthma to psoriasis. The multivariate analysis included variables that were associated with the study outcome at a significance level of p-value < 0.05. Examinees with missing baseline characteristic data (10.3%) were excluded from the multivariate analysis. Additional multivariate models were calculated, adjusted for age and sex (0.0% excluded) and adjusted for age, sex, SES and BMI (0.7% excluded). The models with few or no excluded examinees resulted in significant associations similar to those of the full model (see Table V), thus demonstrating that the missing data had only marginal effect. Odds ratios (ORs) are reported with 95% confidence intervals (95% CIs). All statistical tests were 2-sided, and p-value < 0.05 was considered statistically significant. All analyses were performed using SPSS 21.0 (SPSS, Chicago, IL, USA).
Baseline characteristics of the study participants are shown in Table II, as previously described by our group (21, 22). The mean age (SD) of the psoriatic group and the comparison group was 17.32 (0.49) years and 17.45 (0.56) years, respectively. Psoriasis lifetime prevalence among the study population was 0.35%. The psoriatic group included 3,112 patients (56.1% mild disease; 43.9% moderate-to-severe disease) and the comparison group included 884,653 patients. Associations of psoriasis with allergic rhinitis and asthma were evaluated using multivariate analysis adjusted for age, sex, country of origin, SES, number of siblings and BMI.
Table II. Characteristics of the study population
The prevalence of allergic rhinitis and asthma were compared between the psoriatic group and the comparison group. The resulting prevalence was 10.99% vs. 7.17% for allergic rhinitis and 11.08% vs. 7.95% for asthma, respectively. Allergic rhinitis (aOR 1.31; 95% CI 1.16–1.49) and asthma (aOR 1.17; 95% CI 1.03–1.33) were found to be significantly associated with psoriasis compared with the comparison group, as shown in Table III.
Table III. Comparison of allergic rhinitis and asthma between psoriatic group and comparison group
The association of psoriasis with allergic rhinitis and asthma was further assessed separately for mild psoriasis and moderate-to-severe psoriasis, as shown in Table IV. Allergic rhinitis was found to be associated with mild psoriasis (aOR 1.37; 95% CI 1.15–1.63, respectively) as well as with moderate-to-severe psoriasis (aOR 1.26; 95% CI 1.05–1.51, respectively) compared with the comparison group. In contrast, the association between psoriasis and asthma exhibited dependency on psoriasis severity. Asthma was not significantly associated with mild psoriasis (aOR 0.96; 95% CI 0.80–1.16, respectively), but only with moderate-to-severe psoriasis (aOR 1.45; 95% CI 1.22–1.72, respectively), vs. the comparison group. Additional multivariate models, shown in Table V, have shown similar significant associations.
Moreover, the severity of asthma did not differ significantly between the psoriatic group and the comparison group. Persistent asthma was identified in 55.9% of the asthmatic cases in the psoriatic group and in 53.1% of the asthmatic cases in the comparison group (OR 1.12; 95% CI 0.91–1.39).
Table IV. Association between mild and moderate-to-severe psoriasis and allergic rhinitis and asthma (vs. comparison group)
Table V. Comparison of allergic rhinitis and asthma prevalence among psoriatic group (any severity), mild psoriasis and moderate-to-severe psoriasis with comparison group by different multivariate models
The present study showed an association between adole-scent psoriasis and allergic rhinitis and asthma. This association was seen for allergic rhinitis irrespective of psoriasis severity, while for asthma, only moderate-to-severe psoriasis was associated.
To the best of our knowledge, only Augustin et al. (19) performed a similar study among German children with psoriasis, using a cross-sectional study to compare 1,313 children with psoriasis with controls without psoriasis. Similarly to our study, Augustin et al. reported higher odds of allergic rhinitis, asthma and atopic dermatitis among psoriatic patients. However, the findings of this study may only be extrapolated to a limited degree because of enrollment of a mixed age group (younger than 18 years) and lack of severity stratification and standardization of the baseline characteristics.
Few studies among adults have investigated the association between psoriasis and asthma, but no studies have included allergic rhinitis and atopic dermatitis. Consistent with the present study, Fang at el. (9) reported a 1.38-fold higher risk of asthma among a cohort of Taiwanese adults (age ≥ 20 years) with psoriasis, compared with controls without psoriasis. Another study also carried out among adult Taiwanese patients (age ≥18 years) showed that psoriasis patients were more likely to have asthma, compared with controls without psoriasis (10). Similar to our findings, this association was dependent on psoriasis severity. In line with our findings, a study of Danish twins (age ≥ 20 years) (11), based on examinees’ self-reported morbidities, found higher odds of asthma among 1,385 psoriasis patients, compared with controls without psoriasis. Contrary to our findings, this association was observed only for adult onset asthma (age at onset ≥18 years). Of note, substantial differences might be seen between adult and childhood onset asthma. Adult onset asthma is more likely to be related to occupation (12), more often occurs in non-atopic individuals and carries a poorer prognosis (13). In addition, it might overlap or be misdiagnosed as chronic obstructive pulmonary disease (COPD) (27).
The clinical linkage of psoriasis to allergic rhinitis and asthma observed in this study might be supported by recent evidence, characterizing a possible shared immunological phenotype between these conditions. Psoriasis is considered to have a uniform immunological profile, driven by Th17 and Th1 cells (1), but also, a varying degree of Th22 activation (2, 7). Allergic rhinitis, asthma and atopic dermatitis were once considered purely Th2-mediated, but are, in fact, heterogeneous disorders; for each, multiple immunological phenotypes are observed. These phenotypes may feature distinct immunological signatures, including a Th2/Th17 reaction in allergic rhinitis and asthma (4–6, 8) and a Th2/Th17/Th22 reaction in atopic dermatitis (2). Recently, it has been proposed that psoriasis and atopic dermatitis can be viewed as diseases occurring across a spectrum, with certain subtypes having overlapping characteristics (2). These include the paediatric subtype, in which Th1/Th17/Th22 psoriasis and Th2/Th17/Th22 atopic dermatitis seem to be common (2, 7). In addition, Th17 asthma is also seen among children, while higher serum IL-17 is correlated with severe disease (5). Furthermore, a recent comprehensive study held by Östling et al. (28) has shown that nearly 25% of asthmatics express high levels of IL-17. In pathway analysis, the differentially expressed genes in IL-17-high asthma were shared with altered genes in psoriasis lesions.
These findings might suggest that psoriasis and atopic comorbidity among children and adolescents may be linked through a common Th17 or, less likely, through a Th22 pathogenic pathway.
The current study has strengths and limitations. The main strengths of the study are its large sample size, the systematic nationwide data collection and the specialist-proven diagnoses of the investigated diseases. Another strength of our study is that we were able to stratify psoriasis severity. This stratification enabled us to show the severity-dependent association between psoriasis and asthma, further supporting the reliability of our findings. Regarding limitations, being a cross-sectional study eliminates the ability to prove a causal link between psoriasis and allergic rhinitis and asthma. The present study found a lower lifetime prevalence of psoriasis, allergic rhinitis and asthma than previously reported among European and North-American adolescents. The findings regarding psoriasis might be explained by the populations’ diversity, as supported by measurements of a consistently lower lifetime prevalence of childhood psoriasis (younger than 18 years) among Asians compared with Europeans (29). To the best of our knowledge, a specific measurement of the lifetime prevalence of psoriasis among adolescents has not been obtained for Asians. Regarding the prevalence of allergic rhinitis and asthma, wide variations exist globally. This variation was shown in one of the most reliable studies carried out to compare variations in childhood allergic rhinitis and asthma at the population level, the International Study of Asthma and Allergies in Childhood (ISAAC) collaborative project (30, 31). It relied on a patient self-completed questionnaire. As in our study, a large-scale ISAAC-based study of 13- to 14-year-old Israelis have reported a lower than global average of allergic rhinitis and asthma, of 11% and 7%, respectively (32).
Future research is needed to define whether concurrence of psoriasis with allergic rhinitis and asthma reflects a unique immunological profile. A common inflammatory pathway of psoriasis, allergic rhinitis, and asthma may be an intriguing therapeutic target in this subset of patients. In this regard, in an allergic rhinitis and asthma murine model, the inhibition of IL-17 might be promising, as administration of anti-IL-17 antibodies have been reported to suppress allergic rhinitis symptoms and decrease pulmonary inflammation (33, 34).
In conclusion, the present study demonstrates that allergic rhinitis and asthma are common among adolescents with psoriasis. Allergic rhinitis and asthma had not, until now, been fully recognized to be associated with psoriasis in adolescents. Further research is needed to determine whether psoriatic individuals with allergic rhinitis or asthma possess a distinct immunological profile that can be therapeutically targeted.
The authors thank Dr Ron Kedem and Dr Tomer Ziv-Baran for their assistance in statistical analysis.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize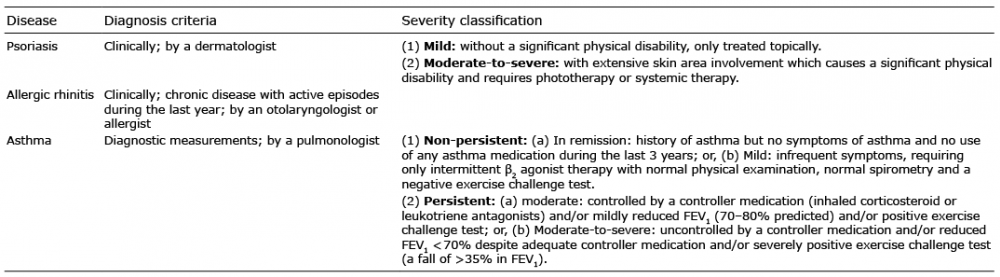 Click to show fullsize
Click to show fullsize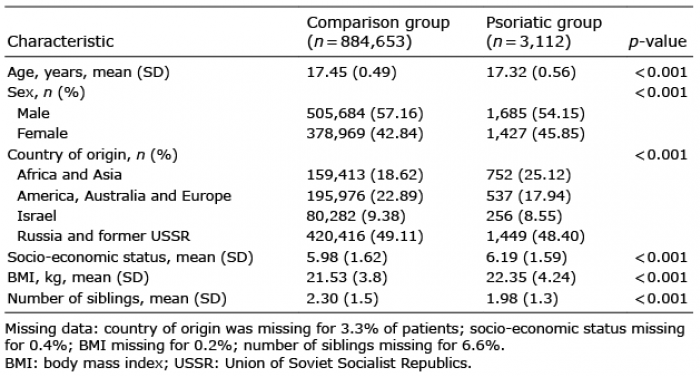 Click to show fullsize
Click to show fullsize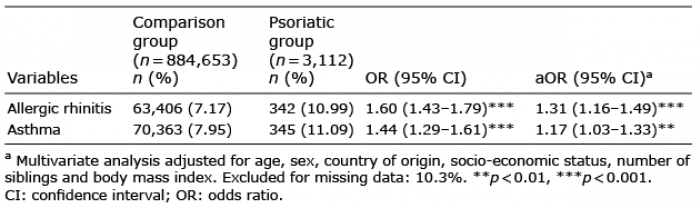 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize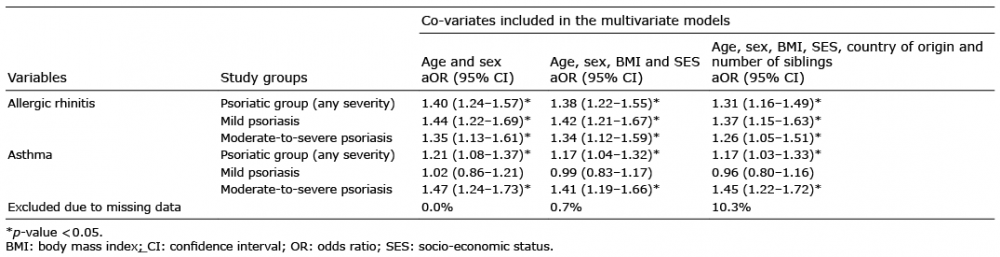 Click to show fullsize
Click to show fullsize