


1Department of Twin Research, King’s College London, London and 2Mount Vernon Cancer Centre, Middlesex, UK
This decade has brought significantly improved outcomes for patients with advanced melanoma with immunotherapies and targeted treatments offering utility in a variety of settings. In 2020, we can hope for durable long-term responses, and complete remission in a subset of patients with metastatic disease. In the adjuvant setting, approximately 50% improvements in recurrence-free survival are seen both with targeted and immuno-therapies. Early data from neoadjuvant immuno-therapy clinical trials are very promising. However, responses to treatment are heterogeneous and not always durable; further advances are required, and several emerging strategies are of particular interest. We review the systemic treatment of melanoma, discus-sing the treatment of unresectable stage III–IV and recurrent disease, outlining curative treatment of cutaneous melanoma in the adjuvant setting and briefly
discussing neoadjuvant systemic therapies for advanced melanoma.
Key words: melanoma; systemic therapy; targeted therapy; immunotherapy.
Accepted Apr 27, 2020; Epub ahead of print Apr 28, 2020
Acta Derm Venereol 2020; 100: adv00141.
Corr: Dr Karla Lee, St. Department of Twin Research, King’s College London, SE1 9RT London, UK. E-mail: karlalee@nhs.net
Melanoma is an aggressive and rare skin cancer that can threaten the lives of patients it affects. New treatments have been introduced over the past decade which have dramatically changed the way in which patients with advanced melanoma are managed. Here we review the treatments currently available to patients with advanced melanoma, focusing firstly on patients with stage IV melanoma. We also review treatments available to reduce the risk of a melanoma returning – these treatments can be given either before (“neoadjuvantly”) or after (“adjuvantly”) a melanoma is surgically removed, but only the latter is currently approved.
Accounting for only 1% of all skin malignancies, melanoma represents the most aggressive and deadly form of skin cancer (1). Melanoma is predominantly a disease of Caucasian populations and affects men and women in equal measure. With a propensity to migrate to draining lymph nodes and any visceral organ, metastatic melanoma carries a poor prognosis.
Prior to 2011, outcomes were poor, with treatment for metastatic disease limited to palliative therapies that offered little or no survival benefit. In 2020, we can hope for durable long-term responses, and complete remission in a subset of patients. The use of immunotherapies and targeted therapies for melanoma in the metastatic, adjuvant and neoadjuvant settings will be reviewed here; the initial management of cutaneous melanoma is discussed separately. This review will cover the systemic treatment of melanoma, starting with a description of therapeutic agents. We will discuss the treatment of unresectable stage III–IV and recurrent disease, outline curative treatment of cutaneous melanoma in the adjuvant setting and briefly discuss neoadjuvant systemic therapies for advanced melanoma.
Immunotherapy
Immune checkpoint inhibitors. Immune checkpoint inhibitors (CPIs) are a form of immunotherapy designed to target key regulators of the immune system. Immune checkpoints provide stimulatory or inhibitory control of immunity. Tumours can use the inhibitory pathways to protect themselves from being targeted by the immune system. CPIs currently in clinical use act to block these negative pathways enabling T-cells to recognise cancer cells more efficiently. Agonists for stimulatory pathways are also in clinical development. CPIs were the first class of therapy shown to improve the overall survival (OS) for patients with advanced melanoma and provide hope of durable, long-term responses in a subset of patients. The most extensively studied immune checkpoint receptors are cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) and programmed cell death protein-1 (PD-1). CTLA-4 and PD-1 induce T-cell suppression through non-overlapping mechanisms and likely impact different populations of T-cells during different phases of the immune response (CTLA-4 during priming and PD-1 during the effector phase), providing a mechanistic rationale for the combination of CTLA-4 and PD-1 blockade.
CTLA-4. Based on promising antitumour activity in preclinical cancer models (2), CTLA-4-blocking antibodies have been developed. Ipilimumab is a fully human monoclonal antibody of the IgG1 isotype that inhibits CTLA-4 leading to enhanced T-cell activation. For T-cell activation to occur, two sequential signals are required (3–5). Firstly, antigens presented in context with the major histocompatibility complex (MHC) I or II on specialised antigen-presenting cells (APCs) must bind with T-cell receptors (TCRs). Following this, there is a translation of TCR stimulation into T-cell activation which requires a costimulatory signal, occurring when B7 surface molecules on the APC bind with CD28 T-cell-surface receptors. Subsequently, T-cell surface expression of CTLA-4 occurs, competitively inhibiting the binding of B7 to CD28, preventing the costimulatory signal and dampening down T-cell activation and proliferation. Treatment can be associated with mechanism-based, immune-related adverse events more frequently than anti-PD-1 treatment.
A second CTLA-4-blocking antibody, tremelimumab, has been developed. Tremelimumab is a fully human anti-CTLA-4 monoclonal antibody of the IgG2 isotype. However, tremelimumab failed to reach its primary endpoint of improved OS compared to standard-of-care chemotherapy for patients with previously untreated, unresectable stage III or IV melanoma (6). Clinical development of tremelimumab is ongoing in a number of non-melanoma cancers.
PD-1. Like CTLA-4, PD-1 inhibits T-cell activity and is expressed by activated T-cells. However, instead of competitively inhibiting co-stimulation by interfering with CD28/B7 ligand interaction, PD-1 negatively regulates TCR-signalling events. While CTLA-4 inhibits T-cells during the priming phase of immune responses, PD-1 is thought to inhibit activated T-cells at a later stage in peripheral tissues, playing a critical role in the maintenance of peripheral T-cell tolerance.
The first anti-PD-1 blocking antibody developed was nivolumab, a fully human monoclonal antibody of the IgG4 isotype that binds to PD-1, preventing it from interacting with its ligands. Pembrolizumab was the second anti-PD-1 blocking antibody to be used in advanced melanoma; like nivolumab, pembrolizumab is a fully human monoclonal antibody of the IgG4 isotype that binds to human PD-1 preventing ligand interaction. Nivolumab and pembrolizumab are clinically comparable in terms of efficacy and toxicity as monotherapy for inoperable melanoma (despite the absence of any head-to-head comparison), but only nivolumab is licensed for delivery as a combination with ipilimumab. The subtle preclinical and molecular differences between these two agents have been described by Fessas et al. (7). Compared with ipilimumab, anti-PD-1 blockade with pembrolizumab has been shown to have a superior clinical efficacy and improved toxicity profile with fewer SAEs and fewer patients requiring early treatment withdrawal (8).
Oncolytic virus therapy. Oncolytic viruses are a novel class of intratumoural immunotherapies that show promise for treating solid tumours. Talimogene laherparepvec (T-VEC) is a first-in-class, genetically modified, herpes simplex virus type 1-based oncolytic immuno-therapy approved for the local treatment of unresectable cutaneous, subcutaneous and nodal lesions in patients with melanoma recurrent after initial surgery. The mechanism of action and clinical applications of T-VEC are described in detail by Raman et al. (9). The key study to note in the context of advanced melanoma is the OPTiM study which randomised 436 participants in a 2:1 ratio to receive intratumoural T-VEC or subcutaneous recombinant granulocyte macrophage colony-stimulating factor (GM-CSF). OPTiM first reported positive findings in late 2015 (10), and recently published final analyses confirmed T-VEC’s association with durable complete responses that were associated with prolonged survival (11).
Targeted therapy
The vast majority of cutaneous melanomas harbour mutations in genes of key signalling pathways. Yet, only a small number of these are considered to be driver mutations due to their active role(s) in cancer development and progression; the others are seen as coincidental passenger mutations that are dispensable for cancer cell viability and develop over the course of tumour evolution (12, 13). The mitogen-activated protein kinase (MAPK) pathway is a complex cascade requiring sequential phosphorylation of the different pathway components. In normal cells, when MAPK activation occurs, it leads to cell growth and differentiation. In cells harbouring BRAFV600E mutations, the normal process of negative feedback does not occur and this results in permanent MAPK pathway activation, leading to uncontrolled proliferation. This path-way offers various points at which the protein cascade can be blocked. Mutant BRAF is a “driver oncogene” as mutant BRAF inactivation can induce cancer cell toxicity due to an acquired dependency of cancer cells on oncogenic, mutant forms of BRAF (14). Targeted inactivation of BRAF by pharmacologic inhibitors is an archetypal example of targeted therapy in cancer (14, 15). The recognition of key molecular mutation, BRAFV600E mutation, provided new therapeutic opportunities and facilitated the development of promising small molecule inhibitory compounds later on. Approximately 40% of melanomas harbour a BRAF mutation (16, 17), the most common being BRAFV600E, followed by BRAFV600K and rarer genotypes (18).
MEK is the next kinase down from BRAF on the MAPK cascade. BRAF inhibition is the most established form of targeted therapy in melanoma and produces rapid, but often short-lived, tumour regression in the majority of patients. When MEK inhibition is added to BRAF inhibition, increased efficacy and reduced toxicity are seen. Indeed, the combination of BRAF and MEK inhibition offer greater inhibition of MAPK signalling and result in longer durations of response, higher rates of tumour response, and less cutaneous toxicity often observed from paradoxical MAPK pathway activation with BRAF inhibitor monotherapy (19). The development of acquired resistance to combination BRAF and MEK inhibitor therapy, along with tumour heterogeneity, are formidable obstacles in the treatment of patients with advanced melanoma.
BRAF inhibitors. The first BRAF inhibiting tyrosine kinase inhibitor (TKI) approved by the US Food and Drug Administration (FDA) for melanoma treatment was vemurafenib in 2011 (20). The success of vemurafenib in phase I and II settings (21, 22) and then in the BRIM-3 study (23) encouraged intensive investigation of the molecular mechanisms of pathogenesis in melanoma and development of new therapeutic strategies targeting specific molecules in the MAPK pathway. Dabrafenib followed vemurafenib and is another small molecule agent inhibiting BRAFV600 mutation-positive melanoma cell growth, demonstrating efficacy as a monotherapy in the BREAK-3 study (24). Encorafenib is a second generation BRAF inhibitor, characterised by a substantially prolonged dissociation half-life (25), and in the phase III COLUMBUS trial demonstrated superior efficacy over vemurafenib monotherapy (26).
MEK inhibitors. Preclinical and early studies demonstrated that the addition of a MEK inhibitor to a BRAF inhibitor decreased tumour growth, delaying the development of resistance and reducing occurrence of skin lesions in metastatic melanoma (27). As a results, there has been considerable interest in various combinations of BRAF and MEK inhibition. Trametinib was the first MEK inhibitor approved for the treatment of BRAF-mutated metastatic melanoma naïve to BRAF-inhibition. Trametinib is approved for use in combination with dabrafenib showing efficacy both as a monotherapy when compared to investigator’s choice chemotherapy (28), and when combined with dabrafenib (29, 30). Cobimetinib is another MEK inhibitor which demonstrated efficacy while used in combination with vemurafenib in the CoBRIM study (31), while bimetinib is the most recently-introduced of the MEK inhibitors and has demonstrated efficacy in the COLUMBUS study (26).
Chemotherapy
Prior to recent advances, chemotherapy was the backbone of treatment for metastatic melanoma. Studies reported responses in 10–15% of patients with 5 year survival in only 2–6% of patients (32). Despite the poor survival statistics, agents such as dacarbazine or the combination of a platinum agent and a taxol were the standard of care for many years, due to a paucity of other useful therapeutic options. Currently chemotherapy is used infrequently, and primarily when immunotherapy and targeted therapy options have either failed or cannot be used.
Systemic therapy is indicated for patients with stage III–IV melanoma in whom surgical metastasectomy is not appropriate. Patients with oligometastatic disease should be evaluated for possible metastasectomy, as complete resection of metastatic disease can achieve cure (33, 34). In such cases, adjuvant therapy would then be recommended following complete resection to reduce recurrence risk (discussed later). This section will focus on systemic therapy for inoperable melanoma.
The primary systemic therapy options for patients with metastatic melanoma are CPIs, and, where a BRAF mutation is the driver mutation, MAPK targeted therapies. The presence or absence of a BRAF mutation is currently the only reliable predictive biomarker that can influence the treatment of advanced melanoma and must promptly and accurately be determined. Many different methods for BRAF testing are currently in use internationally (35–37), but a discussion of these is beyond the scope of this review. Targeted MAPK therapy is not indicated in patients without a characteristic BRAF mutation and may indeed be harmful to this patient group.
Whether patients with BRAFV600 mutant melanoma should receive CPIs or MAPK targeted therapy as first line therapy is not always straightforward and prospective head-to-head comparative trials of MAPK inhibitors and CPIs are lacking. A 2019 update of survival in metastatic melanoma reported exploratory analysis of survival data from selected CPI and TKI clinical trials (38). In first line therapy, mean 3-year OS proportions were 41.3% for BRAF plus MEK inhibition, 49.9% for PD-1 inhibition and 58.4% for CTLA-4 plus PD-1 inhibition. Comparison of the mean progression free survival (PFS) and OS curves of kinase inhibition and checkpoint blockade revealed a superiority of combined BRAF plus MEK inhibition within the first 12 months, later changing to a superiority of PD-1 blockers alone or in combination with CTLA-4 blockade. In second-line or higher, BRAF plus MEK inhibition was superior to anti-PD-1 monotherapy throughout the first 3 years; mean 3-year OS proportions were 42.4% for BRAF plus MEK inhibition, and 40.1% for PD-1 inhibition.
Checkpoint inhibitors
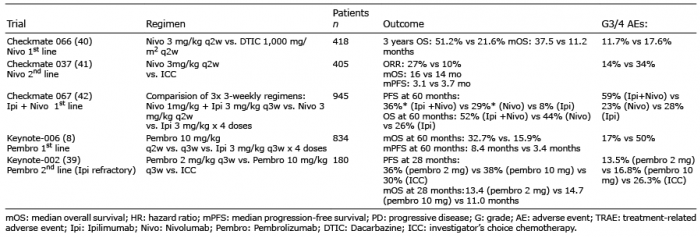
Table I outlines key phase III CPI studies in melanoma. Nivolumab (39) and pembrolizumab (40, 41) have been established as preferred monotherapy options for inoperable melanoma given their efficacy over standard of care chemotherapies and acceptable toxicity profiles. Checkmate-067 compared nivolumab and ipilimimab as a combination with nivolumab and ipilimumab monotherapies, recently demonstrating an OS of 52% for the combination group at 5 years. This exceptional survival was associated with 59% of patients receiving the combination suffering grade 3 or 4 adverse events (42). As such, combination PD-1 and CTLA-4 blockade is usually considered only for those patients with a very good performance status, with some institutions and oncologists preferring CPI monotherapy for metastatic disease. Untreated brain metastases represent one particular clinical scenario in which combination CPI offers particular advantage and may be preferred in this instance (43).
Table I. Landmark checkpoint inhibitor (CPI) trials in metastatic melanoma
MAPK pathway inhibition
Overall response rates to vemurafenib, dabrafenib and encorafenib monotherapies are 45%, 51% and 60%, respecively (29, 44, 45). A number of studies have presented clear evidence that the combination of these agents with a MEK inhibitor provide increased efficacy with a reduction in toxicity (Table II). In the COLUMBUS study, encorafenib plus bimetinib showed favourable efficacy compared with encorafenib or vemurafenib monotherapy, with the combination associated with an improved tolerability profile compared with either monotherapies (26). The CoBRIM study showed improved survival of vemurafenib and cobimetinib compared with vemurafenib alone, with no significant difference in toxicity (31). Robert et al. recently analysed pooled extended survival data from COMBI-d and COMBI-v trials (n = 563) which compared dabrafenib and trametinib with dabrafenib and vemurafenib monotherapies, respectively, reporting complete responses in 19% of patients and improved long-term outcomes, with OS rates of 71% and less toxicity seen with the combination of BRAF and MEK inhibition (29).
Table II. Landmark mitogen-activated protein kinase (MAPK) targeted therapy trials in metastatic melanoma
Checkpoint and MAPK inhibition combinations
Increasing evidence suggests that BRAF and MEK inhibition has an immune-modulating effect, enhancing anti-tumour immunity (47–49). Early evidence from treatment of advanced melanoma with BRAF inhibition demonstrated increased expression of PD-1 and its ligand, PD-L1 (50), suggesting there may be a therapeutic benefit in combing BRAF inhibition with CPI. A phase 1 study showed vemurafenib and ipilimumab to have an unacceptable rate of hepatic toxicity, leading to its discontinuation (51). A preclinical study demonstrated that treatment with BRAF and MEK inhibition, in the presence of the oncogenic BRAFV600 mutation, improved CPI anti-cancer effect without any negative impact on immune cell function (47), as had previously been thought may be the case (52). It is believed that MEK inhibition has a protective effect on CD8+ T-cells due to chronic TCR stimulation (53). Such toxicity in the context of BRAF inhibition may be related to the paradoxical activation of MAPK in BRAF wild-type cells and can be ameliorated by the addition of a MEK inhibitor (54).
Preclinical data provide rationale to support testing of a triple combination of BRAF inhibition, MEK inhibition and PD-1 blockade (47, 53). A number of trials have reported relatively initial results with some 1- and 2-year data available, indicating that the combination of CPI and TKI may have a role as standard of care within the next numbers of years (Table III).
Table III. Landmark check-point/tyrosine kinase inhibitor (CPI-TKI) targeted therapy trials in metastatic melanoma
The role of adjuvant therapy in patients with resected stage III melanoma is a rapidly evolving field. Interferon was the first agent shown to have utility in this space, however, advances in both targeted therapies and immuno-therapies have led to a number of practice-changing adjuvant trials in resected stage III and IV disease. By eliminating the micrometastatic disease that remains after surgery, adjuvant systemic therapy aims to reduce disease recurrence and ultimately improve rates of cure following surgical resection of locoregional or stage IV disease. Patients with resected stage III or IV disease have significant differences in predicted survival at 5 years ranging from approximately 80% for stage IIIa disease to less than 20% for resected stage IIId disease (58). Adjuvant treatment with either CPI or MAPK targeted therapy have dramatically changed outcomes for this patient group, with approximately 50% increased recurrence-free survival (RFS) for both treatment approaches (59–62). CPIs and MAPK targeted therapies have not been directly compared in phase III studies and there is currently no clear consensus on choice of approach for patients with a BRAFV600 mutation in the adjuvant setting.
For patients with stage I and II primary tumours and a negative sentinel lymph node biopsy, there is presently no indication for adjuvant therapy (63). It is worth noting that patients with high risk (primary tumour > 4 mm, or > 2 mm with ulceration) but node negative tumours were excluded from the phase III clinical trials that evaluated nivolumab, ipilimumab and the targeted therapy doublet of dabrafenib and trametinib (62, 64, 65). As such, data on adjuvant therapy in this cohort of patients is not avail-able and is currently under investigation.
Adjuvant checkpoint inhibitors
As already discussed, CPI represents an important advance in the treatment of patients with inoperable melanoma. These results led to the evaluation of these agents in the adjuvant setting for patients at high risk of recurrence following initial surgery. Adjuvant treatment with ipilimumab at 10 mg/kg dosing was shown to have a 10% absolute improvement in OS and RFS, but toxicity and high treatment-related death rates limited its widespread use and it was never licensed for this indication in Europe (66). Only 13.4% of patients completed the full planned course of treatment, and nearly 40% of patients discontinued treatment after the first 4 doses due to treatment-related side effects. Adjuvant anti-PD-1 therapy has been tested in two large phase III studies, Checkmate 238 and Keynote 054, which have established nivolumab and pembrolizumab as the CPIs of choice for the adjuvant treatment of resected melanoma (60, 67). Table IV summarises the key trials in this setting.
Table IV. Summary of randomised controlled trials of adjuvant therapy for patients with cutaneous melanoma
Adjuvant targeted therapy
A key study in this context is COMBI-AD, a study of 870 Stage III BRAF mutant melanoma patients in the adjuvant setting following excision and lymphadenectomy (61, 64). They were randomised to the combination arm of dabrafenib and trametinib, or to matching placebos for one year. The primary endpoint, RFS, was longer with dabrafenib and trametinib than with placebo (4-year rate: 54% vs 38%; hazard ratio [HR] 0.49, 95% CI 0.40–0.59), with treatment benefits observed irrespective of baseline factors, according to subgroup analysis (61). Vemurafenib was compared to placebo in the adjuvant BRIM8 study demonstrating efficacy but high rates of grade 3/4 toxicity (68).
Given the success of immunotherapies and targeted therapies for the treatment of advanced melanoma, the natural extension is to identify the role of these therapies in the neoadjuvant setting, with a wealth of clinical trials currently underway. Patients with clinically detectable stage III melanoma represent a high-risk population with poor outcomes when treated with upfront surgery alone and are obvious candidates for investigation of neoadjuvant therapy. However, the clear need to carefully evaluate short-term clinical endpoints such as RFS, and long-term endpoints of neoadjuvant therapy against those of adjuvant therapy remains. Neoadjuvant therapy for melanoma is not presently standard-of-care but represents an active area of research with a large number of completed and recruiting trials with differing designs, endpoints, and methods of analysis under investigation. Table V illustrates those neoadjuvant (preoperative therapy) trials which have reported data.
One study of note is OPACIN-NEO study which reported in 2018 (69). OPACIN-NEO examined neoadjuvant combination CPI with 3 different regimens of ipilimumab and nivolumab. A combination of ipilimumab at 1 mg/kg combined with nivolumab at 3 mg/kg given 3-weekly for two cycles was chosen to take forward into later phase studies, as this combination had a response rate of 77%, with responders experiencing excellent outcomes to date. If more mature data confirm these early observations, this schedule will be tested in randomised phase 3 studies versus adjuvant therapies, which are the current standard-of-care systemic therapy for patients with stage III melanoma.
Table V. Neoadjuvant trials with available data
The investigation of new immunotherapy and/or targeted therapy combinations, such as anti-PD-1/anti-CTLA-4 CPIs with other immunotherapies (e.g. indoleamine 2,3 dioxygenase inhibitors, antilymphocyte activation 3, histone deacetylase inhibitors, Toll-like receptor 9 agonists, anti-glucocorticoid-induced tumour necrosis factor receptor, pegylated interleukin-2), combination targeted therapies (e.g. MEK and CDK4/6 co-inhibition), and the combined use of immunotherapy and continued research on targeted therapy (e.g. the triplet combination of BRAF/MEK inhibition with anti–PD-1s) are keys for the future of systemic therapy for advanced melanoma. The identification of novel therapeutic targets in the MAPK pathway provides opportunity to improve outcomes by overcoming de novo and acquired resistance to BRAF/MEK inhibition. Adoptive cell transfer may have a potential role in patients whose disease has progressed following CPI. Altogether, these new approaches offer potential to build upon past advances and improve long-term survival outcomes for patients with melanoma.
This decade has brought significantly improved outcomes for patients with advanced melanoma with the advent of immunotherapies and targeted treatments that have utility in a variety of settings. However, responses to treatment are heterogeneous and not always durable. Further advances are required, and several emerging strategies are of particular interest.
Conflicts of interest: KAL has no conflicts of interest to report. PN reports personal fees from AstraZeneca, BMS, Merck, Immunocore, Pfizer, Ipsen, 4SC, Pierre Fabre and Roche.


 Click to show fullsize
Click to show fullsize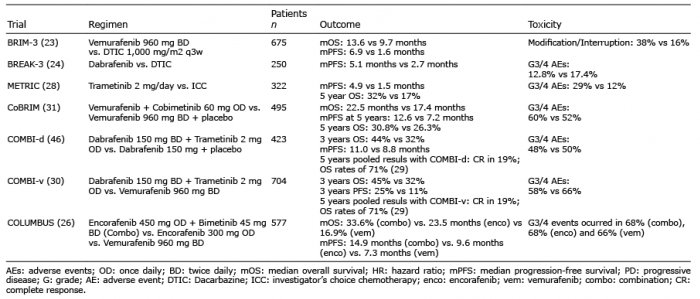 Click to show fullsize
Click to show fullsize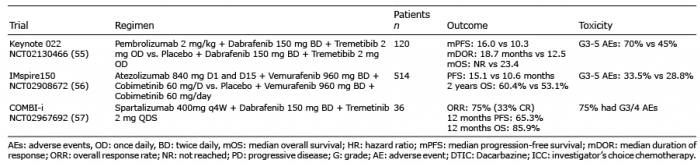 Click to show fullsize
Click to show fullsize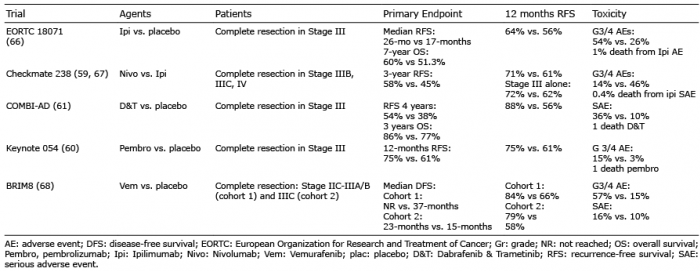 Click to show fullsize
Click to show fullsize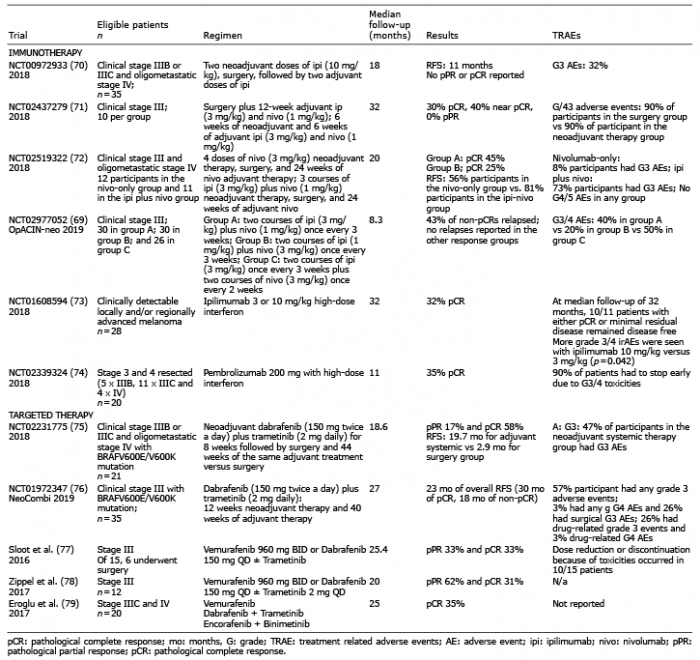 Click to show fullsize
Click to show fullsize