


1Department of Dermatology, Haukeland University Hospital, 2Department of Clinical Science, University of Bergen, 3Department of Heart Disease, Haukeland University Hospital, Bergen, 4Arctic Nutrition AS, Ørsta, 5Smerud Medical Research International AS, Oslo, and 6Department of Sport, Food and Natural Sciences, Western Norway University of Applied Sciences, Bergen, Norway
The effect of omega-3 polyunsaturated fatty acid supplements in patients with psoriasis vulgaris has previously been investigated, but interventions varied in source, composition, dose, administration route and duration of treatment. The observed beneficial effects in patients with psoriasis vulgaris using herring roe oil as a dietary supplement prompted this investigation. This randomised, double-blind and placebo-controlled study was designed and performed to explore the efficacy and safety of herring roe oil supplementation in 64 patients with plaque psoriasis (ClinicalTrials.gov: NCT03359577). The primary end-point was comparing the change in mean Psoriasis Area Severity Index (PASI) scores in the herring roe oil treatment group and the placebo group from baseline to week 26. In the intention-to-treat population, a statistically significant improvement in the mean PASI score was observed with herring roe oil compared to placebo at 26 weeks. In the recruited patient group, the measured improvement was greatest in patients with a PASI score
from 5.5–9.9 at baseline.
Key words: herring roe oil; psoriasis; omega-3; phospholipids.
Accepted May 4, 2020; Epub ahead of print May 7, 2020
Acta Derm Venereol 2020; 100: adv00154.
Corr: Kåre Steinar Tveit, Department of Dermatology, Haukeland University Hospital, Jonas Lies vei 75, NO-5021 Bergen, Norway. E-mail: kare.steinar.tveit@helse-bergen.no
The effect of herring roe oil capsules was tested in patients with psoriasis. This study demonstrates a positive effect on psoriasis. Disease severity is important when determining the appropriate treatment of psoriasis patients. In recent years, several new drugs have become available for the treatment of severe psoriasis whereas there have been few treatment advances for patients with milder psoriasis. This study demonstrates promise for herring roe oil as a safe treatment option in patients with non-severe psoriasis.
Psoriasis can be divided into mild, moderate or severe psoriasis based on the extent of body surface area (BSA) covered by psoriasis (1), and into mild and moderate to severe based on Psoriasis Area Severity Index (PASI). For the treatment of patients with a PASI score above 10, a growing armamentarium of systemic biological medicines has become available during the past decade. For patients with psoriasis with BSA< 10% and/or PASI < 10 there have been few treatment advances in recent years.
Several studies have investigated the effects of omega-3 fatty acids in the treatment of psoriasis (2–4). A systematic review by Upala et al. (5) stated that no conclusions could be drawn regarding the use of n-3 polyunsaturated fatty acids (PUFAs) and improvement in psoriasis. This review found 12 eligible clinical studies where ω-3 PUFA interventions varied in source, composition, dose, administration route and duration of treatment. In 10 out of the 12 reviewed studies, treat-ment duration was shorter than 26 weeks. The ratio of eicosapentaenoic acid (EPA) to docosahexaenoic acid (DHA) was typically 1:1, or contained more EPA than DHA (5).
One major difference between herring roe oil (HRO)and the ω-3 PUFAs from fish oils is the natural DHA to EPA ratio, which is approximately 3:1 in herring roe. EPA has been found to cause a switch in production of eicosanoids from proinflammatory prostaglandins and leukotrienes in the 2 and 4 series, respectively, to the less inflammatory 3 and 5 series (6). In addition, DHA is metabolized to Specialized Pro-Resolving Lipid Mediators (protectins, resolvins and maresins) which reduce inflammatory processes (7). In herring roe, approximately two thirds of the fatty acids are esterified to phospholipids, including phosphatidylcholine. DHA and EPA found in triglyceride lowering medicines are typically bound to an ethyl group (Omacor®) or they are free fatty acids (Epanova®). These differences may especially affect the bioavailability of DHA and EPA (8, 9).
In this clinical study, the efficacy of capsulated HRO was investigated in psoriasis patients with PASI < 10. We postulated that the effect of this composition differs from fish oils previously tested in clinical studies of patients with psoriasis.
Subjects and study design
Sixty-four patients with stable, plaque psoriasis were recruited at the Department of Dermatology, Haukeland University Hospital, Bergen, Norway. The patients were enrolled in a randomized, 26-weeks, single-centre, placebo-controlled, double-blind study to investigate the effects of a dietary supplement containing HRO. The study was approved by the Regional Committees for Medical and Health Research Ethics in western Norway (REK Vest, 2017/938).
Patients consented to participate in writing. Eligible patients were block randomized using randomly selected block sizes, stratified according to sex, and assigned to either HRO or to the control group (Coconut oil). In both groups, patients received 10 capsules daily, 5 in the morning and five in the evening in conjunction with a meal. Remaining capsules were counted at clinic visits.
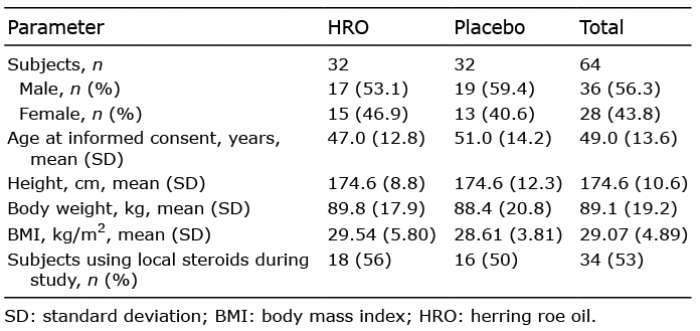
Patients with stable psoriasis for 6 months and with PASI scores less than 10 were eligible to be included in the study. Patients on stable local anti-psoriatic maintenance treatment for more than two months before study start continued this treatment. There were no limitations on the use of unmedicated moisturising creams during the study. Patient demographics and numbers of patients using local steroid treatment are shown in Table I.
Table I. Patient demographics
Herring roe oil capsules
Each HRO capsule contained 292 mg poly-unsaturated fatty acids (total ω-3): 22 % eicosapentaenoic acid (EPA, 20:5 ω-3) and 66 % docosahexaenoic acid (DHA, 22:6 ω-3), where approximately 35% of both was bound to phospholipids, including phosphatidylcholine. The total daily dose of EPA and DHA was 2.6 g and the total lipid dose was 5.9 g. Each placebo capsule contained medium chain triglycerides: Coconut oil high in caprylic acid (C8:0) and capric acid (C10:0). The same type 590 mg softgel capsule was filled with active substance or placebo.
Clinical examinations
Clinical examinations were performed at screening, baseline and at weeks 6, 12, 18 and 26. Standardised scoring tools in psoriasis were used to assess the severity of psoriasis i.e. PASI (10, 11), Physician’s Static Global Assessment (PSGA) (11), and BSA (1).
Patient reported data
Dermatological Life Quality Index (DLQI) (12) and Visual Analogue Scale (VAS) scores were used to measure: itching, pain (skin/joints), singeing and general health conditions (general/skin). Bi-weekly, questionnaires concerning compliance, number of fish meals, number of alcohol units, use of rescue medication (local steroids), intake of sugar, exercise and adverse events were completed by participants.
Dietary requirements
Patients were instructed to discontinue any supplements of cod liver oil, ω-3 and choline for 4 weeks prior to study commencement. Vitamin D, ω-3 and choline supplements were prohibited during the study. Patients were asked not to change their diet including keeping their usual intake of fish in the diet, and to refrain from excessive alcohol intake.
Laboratory analyses
All serum, plasma and full-blood samples were aliquoted and kept in a locked –80°C freezer until all analyses were performed. Analyses were performed using the same controls and procedures as those routinely used at the hospital laboratory. Levels of pro-inflammatory cytokines and C-reactive protein (CRP) were measured.
Cytokines were measured using a panel of magnetic beads for the detection of 16 cytokine analytes (IFN-γ, IL-1α, IL-1β, IL-1ra, IL-2, IL-6, IL-10, IL-12p70, IL-17A, IL-21, IL-22, IL-23, IL-33, TNF-α, VEGF-A, VEGF-D). The panel was obtained from R&D systems (McKinley, MN, USA). The assay was performed as recommended by the manufacturer, and Luminex 100 (Luminex Corp., Austin, TX, USA) and STarStation Software v.3.0 (Applied Cytometry System, Dinnington, UK) was used for recording and analysing the data.
Statistical analysis
The primary variable was the change from baseline to week 26 in PASI in the HRO group as compared to placebo. The intention-to-treat (ITT) population was used for calculations. ITT was defined as randomised patients who received at least one dose of study treatment. For subjects discontinuing the study before week 26, the last observation was imputed as the week 26 value. The primary end-point was analysed by analysis of covariance (ANCOVA). The change in PASI score from baseline to week 26 was modelled as a function of treatment group and baseline PASI score. A significance level of 5% was used in two-tailed tests. Treatment group and baseline PASI score were kept in the model regardless of p-values, other covariates i.e. sex and age were kept if significant on a 5% level.
Patient attendance
In the HRO group, 3 patients discontinued the study. One patient withdrew due to an adverse event (gastritis), one patient withdrew at 6 weeks due to unsatisfying response and one was lost to follow-up. All patients in the placebo group completed the study (Fig. 1).
Fig. 1. Flow diagram. HRO: herring roe oil.
Efficacy
Baseline characteristics of the study groups were comparable (Tables I and II). Mean DLQI, PASI, BSA, PSGA and CRP at baseline (week 0) and at week 26 are displayed in Table II. Patients included had baseline PASI scores between 3.4 and 9.9. The mean baseline CRP in the HRO group was higher than in the placebo group and the standard deviation was large due to 3 patients with elevated CRP concentrations at 17, 26 and 68 mg/l. Baseline PASI scores in the same patients were 3.7, 5.5 and 4.9.
Table II. Mean (SD) DLQI, PASI, BSA and PSGA scores, and 95% CI at baseline (week 0) and at week 26, change from baseline within group and comparison between groups. Last observation carried forward, intention-to-treat population. Mean (SD) measured CRP (mg/l) at baseline (week 0) and at week 26, change from baseline within group and comparison of log10 transformed CRP between groups
There was a statistically significant improvement in the mean PASI score with HRO treatment compared to placebo treatment with a mean change in PASI score estimated to –1.1 with a 95% confidence interval < –2.2, –0.025>, p = 0.0451. The photograph displays one patient in the active treatment group at week 26 (Fig. 2, PASI: 0.7, Baseline: PASI 9.5).
Fig. 2. Psoriasis on the back of a patient in the active treatment group at week 26 (Psoriasis Area Severity Index: 0.7).
There were no statistically significant beneficial effects of treatment compared to placebo in analyses of variables such as PASI 50, PSGA, DLQI, BSA or VAS scores (data not shown) during the course of the study.
A panel of cytokines (IFN-?, IL-1α, IL-1ra, IL-1β, IL-2, IL-6, IL-10, IL-12p70, IL-17A, IL-21, IL-22, IL-23, IL-33, TNF-α, VEGF-A, VEGF-D) was measured in plasma at week 0, 12 and 26. Generally, measured cytokine concentrations at baseline were low in the majority of patients in both study groups which is as expected in patients with mild disease (data not shown). Although certain cytokines dropped significantly in the active treatment group (IFN-γ, IL-6, IL-21, IL-22, IL-23, IL-33) from baseline to week 26, no statistically significant differences were observed when comparing changes of cytokines in the active treatment group with changes in the placebo group.
Post-hoc analyses
The ITT population was split into halves of low and high baseline PASI scores, separated at the median score of 5.5 and the difference in mean PASI scores between study groups were compared at week 26. In the patients with baseline PASI ≤ 5.5, the treatment difference between HRO and placebo in terms of PASI score was estimated to –0.005 with a 95% confidence interval < –1.2, 1.2>, p = 0.99, indicating no difference between HRO treatment and placebo. However, in the subjects with baseline PASI > 5.5, the mean treatment difference between HRO and placebo in PASI score was estimated to –2.4 with a 95% confidence interval <–4.3, –0.5>, p = 0.0157, showing a statistically significant improvement with HRO treatment compared to placebo (Fig. 3). Effects of age and sex as explanatory variables were investigated, but did not reveal any trends.
Analyses of changes in cytokine levels were undertaken. The numbers of patients with a decrease, no change or increase in plasma cytokines from baseline to week 26 were reviewed for all measured cytokines. The results for IL-17A and IL-23 are shown in Table III.
Fig. 3. Changes in Psoriasis Area Severity Index (PASI) score from baseline to week 26, in herring roe oil (HRO) and placebo treated patients with baseline PASI >5.5 (n = 31). Boxplot showing minimum, maximum, Q1 (25th percentile), Q3 (75th percentile), median (line) and mean (diamond) changes in both treatment groups. Patients in the sub-population were evenly distributed in the treatment groups, HRO n = 15; placebo n = 16.
Table III. Numbers of patients with or without changes of interleukin (IL)-17 and IL-23 from baseline to week 26
Safety
Adverse events were recorded throughout the study and most patients experienced one or more adverse events in the 26-week study period, i.e. 94% of patients in the HRO group and 88% of patients in the placebo group. No serious adverse events were related to the administration of active treatment or placebo.
Adverse events in skin and subcutaneous tissue were equally distributed between the active (44%) and the placebo (44%) group. Infections and infestations, primarily influenza like illness, pyrexia, influenza and nasopharyngitis, were evenly represented in the HRO and the placebo group.
In the active treatment group, 47% (n = 15) of patients experienced gastrointestinal events whereas 34% (n = 11) of patients in the placebo group experienced such events. The most frequently reported gastrointestinal events were nausea (16%), diarrhoea (14%), upper abdominal pain (13%), flatulence (11%) and abdominal discomfort (9%) and their prevalence were similar in both study groups.
Musculoskeletal and connective tissue events originated from 16% (n = 5) of the patients treated with HRO and from 41% (n = 13) of the patients in the placebo group.
Ω-3 fatty acids as phospholipid esters have promise as adjunct treatment for plaque psoriasis (13, 14). The fatty acids have multiple roles in the skin, including maturation and differentiation of the stratum corneum, inhibition of proinflammatory eicosanoids and inhibition of proinflammatory cytokines (tumour necrosis factor-alpha, interferon-gamma, and interleukin-12) (15).
Improvement of the mean PASI score in the HRO group compared to the control group at 26 weeks was demonstrated in this study. The effect was statistically significant in the ITT population and in a post-hoc analysis the effect was larger for patients with PASI over 5.5 at baseline. Beneficial effects of treatment on PASI were not observed at the earlier visits (weeks 6, 12 and 18). Thus, the time to onset of efficacy was relatively long, which may be explained by the mechanism of action or the relatively mild nature of the disease in this particular patient population which had PASI < 10 at baseline.
The impact of bioactive substances present in HRO on pro-inflammatory and anti-inflammatory mediators implicated in psoriasis, has been previously studied (16–19). Although the mechanism of action of HRO in psoriasis is unknown, lipid mediators derived from DHA have demonstrated anti-inflammatory effects in animal disease models, including suppression of IL-17A (20).
Statistically significant reductions of mean IL-17A and IL-23 plasma concentrations were not observed in this study when comparing the active treatment group and the control group from baseline to week 26. However, in the comparison of patient numbers with a decrease, no change or an increase in IL-23, significantly more patients in the HRO treated group had a decrease in plasma levels (n = 10) than an increase (n = 2) at week 26, indicating that IL-23 could be involved in the observed disease improvement.
Observations of clear reductions in plasma cytokine concentrations may not be expected in this study population as the baseline concentrations of cytokines were low in a large proportion of the recruited patients.
The treatment effect of HRO versus control in the total study population was a mean change in PASI score estimated to –1.1 at week 26. As evidenced by the post-hoc analysis, which split the study population in halves of low and high baseline PASI scores, the measured efficacy was mediated by patients with baseline PASI scores above 5.5. The inclusion of patients with mild psoriasis could explain why secondary efficacy endpoints were not met. Firstly, PASI does not discriminate well when BSA is low (11). This is a simple consequence of the scoring methodology: If the PASI score assigned for each lesion characteristics (erythema, thickness, scaling and area) is 1, a relative reduction in either of these categories would not impact the PASI score unless lesions are completely cleared. Hence, measuring improvements at the lower end of the scale is inherently challenging (11). Secondly, the inability to measure significant effects in secondary endpoints may also be due to baseline values reflecting mild psoriasis. Mean baseline DLQI was < 9 and more than 80% of patients were categorised with PSGA ≤ 2. Furthermore, a delay in measurable improvements of patient assessed dermato-logy life quality may be expected. Another reason is that the improvement at 26 weeks did not reach a sufficiently clinically meaningful level for the patients to be reflected in the patient reported outcome measures (21).
Although this study targeted a psoriasis population typically treated with topical steroids, no attempt was made to compare the efficacy of HRO with steroid creams. HRO will never eliminate the need for local steroids, but it may be demonstrated as a useful long-term treatment alternative e.g. in cases where successful treatment with topical steroids is hampered by adverse reactions (22, 23) or non-compliance (24).
The study treatment was well tolerated and the prevalence of adverse events was as could be expected for a study of 26 weeks duration. Approximately 90% of the patients experienced one or more adverse events and there was no significant difference between the active treatment group and the placebo group. Although one patient withdrew from the study due to abdominal pain, nausea and gastritis, no serious adverse reactions occurred.
According to the NICE guideline on assessment and management of psoriasis, systemic treatment would usually be recommended where severity score is BSA >10% or PASI >10 (25). This study demonstrates promise for HRO as a safe systemic treatment option in patients with psoriasis with PASI<10. More comprehensive studies are needed to establish whether the effect of HRO in the treatment of psoriasis vulgaris is clinically meaningful, investigating doses and defining a patient group with more severe disease in studies of longer duration.
The study was conducted with support from Forskningsenhet for helseundersøkelser (FHU) which was established with financial contributions from Trond Mohn Stiftelse (TMS).
PCS and HH are employed by Arctic Nutrition AS, the company sponsoring the study. NM and SB are employed by Smerud Medical Research International AS, a CRO receiving fees for services from Arctic Nutrition AS.


 Click to show fullsize
Click to show fullsize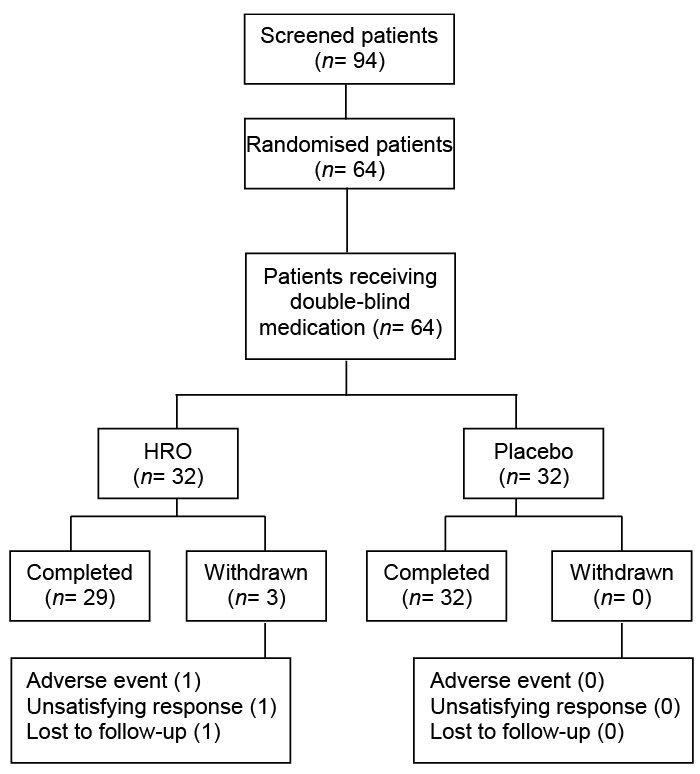 Click to show fullsize
Click to show fullsize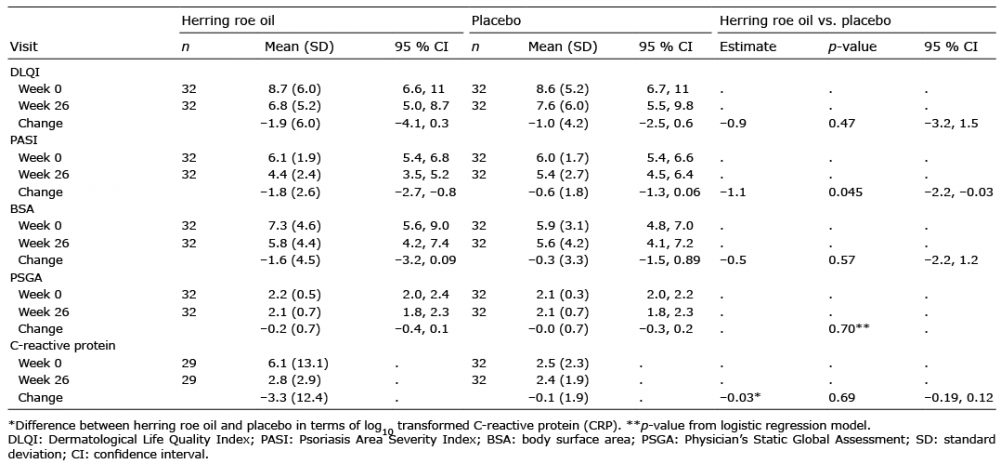 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize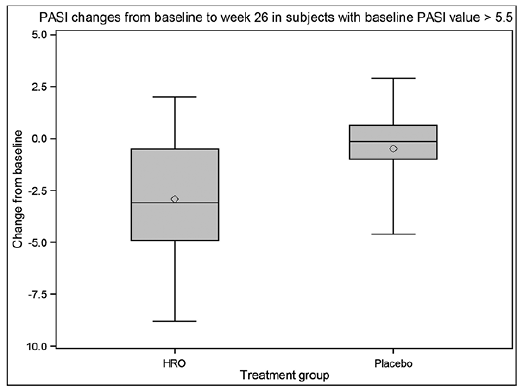 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize