


1Department of Dermatology, University Hospital of Brest, 2LIEN, University of Brest, Brest, 3Univiversity Paris-Sud, 4La Roche-Posay Dermatological Laboratories, Levallois-Perret, and 5EMMA, Fontenay sous Bois, France
Pruritus in atopic dermatitis has been studied extensively; however, evaluation of skin pain has been very limited. The aim of this study was to evaluate the presence, frequency and characteristics of skin pain in patients with atopic dermatitis. A survey was conducted of a representative sample of 5,000 18–80-year-old individuals selected from the French population according to sex, age, geographical area and socioprofessional status. Data on socio-demographic status and the presence of any skin disease were collected. Pain in the past month and health-related quality of life were evaluated. Mean intensity of skin pain during the previous month was assessed with a horizontal visual analogue scale (0–10). Skin pain was reported by more than half of the patients with atopic dermatitis, at a pain intensity of almost 6/10. A neuropathic component was suggested by the Douleur Neuropathique – 4 questions (DN4) questionnaire (a tool for detection of neuropathic pain), as well as the presence of pain inside and outside of skin lesions. Severe alterations to health-related quality of life were assessed with the Dermatology Life Quality Index and Short Form 12 Health Survey (SF-12). Pain is reported frequently by patients with atopic dermatitis. Healthcare professionals should question patients about pain and provide effective treatments. Future clinical trials must take skin pain into account.
Key words: atopic dermatitis; skin; pain; patient-reported outcome; health-related quality of life; itch.
Accepted May 11, 2020; Epub ahead of print May 19, 2020
Acta Derm Venereol 2020; 100: adv00198.
Corr: Laurent Misery, Department of Dermatology, University Hospital of Brest, 2 avenue Foch, FR-29200 Brest, France. E-mail: laurent.misery@chu-brest.fr
Pruritus in atopic dermatitis has been studied extensively; however, skin pain is very poorly evaluated. The aim of this study was to evaluate the presence, frequency and characteristics of skin pain in patients with atopic dermatitis. A survey was conducted on a representative sample of 5,000 18–80-year-old individuals from the French population. Pain and quality of life were evaluated. Skin pain was reported by more than half of the patients with AD, at a pain intensity of almost 6/10. A neuropathic component was suggested by the DN4 questionnaire, as well as the presence of pain inside and outside of skin lesions. Severe alterations in quality of life were assessed by Dermatology Life Quality Index and Short Form 12 Health Survey (SF-12) measurements. Pain is frequently reported by patients with atopic dermatitis. Healthcare professionals should question patients about pain and provide effective treatments. Future clinical trials must also take skin pain into account.
Patients with AD experience pruritus (itch) (1), and this symptom is included in the definition of the disease (2). At the recent meeting of the Harmonising Outcome Measures for Eczema initiative (HOME V) participants agreed that intensity of itch should be measured when assessing long-term control of eczema in addition to the frequency of itch captured by the symptoms domain (3). There is currently an increasing number of promising treatments for patients with AD (4). All these clinical trials investigate soothing itch (1, 4, 5).
Pain is considered a major clinical, social, and economic problem in communities worldwide. Differences in the methodology and conduct of epidemiological studies make it difficult to provide precise estimates of prevalence and incidence; however, the burden of pain is large. Improved concepts and methods are needed to study pain from a population perspective and to enhance the development of strategies for pain prevention and management (6, 7).
Although the first question on the Dermatology Life Quality Index (DLQI) is “Over the last week, how itchy, sore, painful or stinging has your skin been?” (8), few studies have focused on skin pain in atopic patients, and pain is rarely considered a therapeutic target in clinical trials (4). Despite being commonly reported by patients with AD, pain has been poorly studied. To the best of our knowledge, to date, 2 studies have been performed on this topic (9, 10). Unfortunately, these studies included only a small number of patients, and they were not compared with a healthy population. The aim of the current study was to evaluate the presence, frequency and characteristics of skin pain among patients with AD, through a survey of a large representative sample of the French population.
Institutional review board approval was not required, since the study used completely anonymized data and did not involve patient contact.
A self-administered questionnaire was given to a representative sample of the French 18–80-year-old population, a total of 5,000 individuals. The sample was selected according to the usual method to obtain a representative sample according to sex, age, geographical area and socio-professional status, using a stratified proportional, sampling-with-replacement design. Proportional quota sampling was used to ensure the population was representative of the French general population according to data published by the National Institute for Statistics and Economic Studies Institute (INSEE). Data were collected online by random selection of 5,000 Internet users who agreed to participate in surveys and did not have previous information on the aims of the study. Participants were paid. Each selected participant was contacted by e-mail. If contact was not achieved, another potential another participant with the same characteristics was randomly selected.
Socio-demographic data were collected, as well as the presence of AD or any other skin disease according to a list of diseases, as previously described (11). Pain was assessed with a very simple question: “In the past month, have you had any pain in your skin?” Mean pain intensity in the last 24 h was measured using a horizontal visual analogue scale (VAS) ranging from 0 (no pain) to 10 (worst imaginable pain). No other verbal descriptors were given at intermediate points. Among the common pain intensity measures, the validity of the VAS is one of the most evidenced (12).
A neuropathic component of pain was assessed with the Douleur Neuropathique – 4 questions (DN4) questionnaire (13). The DN4 interview (DN4i) consists of 7 items that include sensory descriptors (burning, painful cold, electric shocks, tingling, prickling and numbness), which are potentially applicable to the patient’s pain. For each item, 1 point is assigned if the patient answers “Yes.” A score cannot be calculated if more than 4 items are missing. A score of DN4i ≥ 3 is indicative of a neuropathic pain syndrome, with a sensitivity of 78% and a specificity of 81% (14), and the questionnaire has been broadly validated (15). A systematic review concluded that the DN4 is one of the two most suitable question-naires for screening neuropathic pain (16).
The SF-12 is a short version of the SF-36, which comprises 12 items. It is a health-related generic health-related quality of life (HRQoL) questionnaire that can be used to assess the health status of the general population (17). Responses to questions are dichotomous (yes/no) or ordinal (excellent to poor), or they express a frequency (always to never). The following 2 scores can be calculated from these 12 questions: a Physical Component Summary (PCS-12) and a Mental Component Summary (MCS-12). There is no overall score. Missing data remain as missing. If there was no response to a question from one of these subscales, the score cannot be calculated. Thus, a given subject can have a PCS-12 score but no MCS-12 score. After the abnormal responses and reversed items were processed each response was assigned a coefficient. PCS-12 and MCS-12 scores were obtained by summation. Finally, PCS-12 and MCS-12 scores were transformed (mean 50, standard deviation (SD) 10) for comparison with American “standards”, which allowed the direct interpretation of scores compared with the general American population. Therefore, scores above or below 50 are above or below the mean of the general American population. The higher the score, the better the HRQoL (18). Notably, question 8 investigates pain: “During the past 4 weeks, how much did PAIN interfere with your normal work (including both work outside the home and housework)?”
The DLQI is a health HRQoL scale specific for dermatological disorders (8). It comprises 10 items focusing on the following 8 dimensions: “symptoms”, “daily activities”, “leisure”, “work”, “personal relationships”, “feeling”, “school” and “treatment”. A total score (between 0 and 30) is calculated and can be expressed as a percentage. The higher the score, the greater is the impairment in HRQoL. In general, HRQoL is considered moderately impaired in patients who score between 6 and 11, very impaired in those scoring between 11 and 21, and extremely impaired in those with a score of 21 or more (19).
All collected questionnaires were entered on an Excel file and analysed using STATA 14 and R statistical software (StataCorp, College Station, TX, USA). Quantitative variables were expressed as means with standard deviations (SD). The qualitative variables were expressed as absolute numbers and percentages. The χ2 independence test and the Fisher exact test (for circumstances with low numbers) were performed to test the association between the qualitative variables. The results were expressed in terms of significance (p-values) at an error risk of 5%. A value of p < 0.05 means that the association is statistically significant. For univariate and multivariate logistic regressions, R statistical software was used.
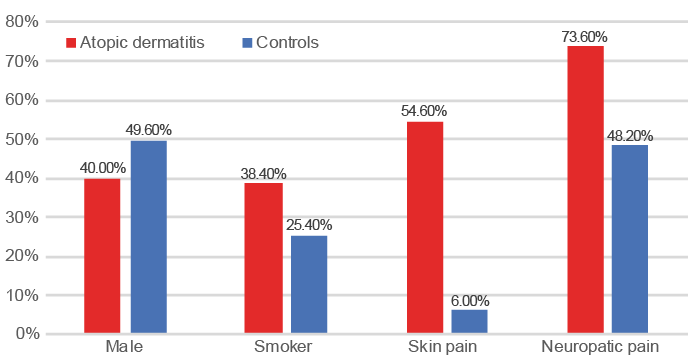
Of the 5,000 subjects interviewed, 185 (74 men and 111 women) reported having AD. A total of 3,247 did not report any skin disease (men: 49.6%, women: 50.4%; mean age: 47.25 ± 16.4 years) and were considered controls (Fig. 1). The mean age of patients reporting AD was 41.7 ± 15 years (controls: 47.25 ± 16.4 years; p = 0.005). The estimated prevalence of AD was 3.7% (95% confidence interval (95% CI) 3.2–4.2%). Patients with AD more frequently were smokers compared with controls (38.4% vs. 25.4%, p < 0.001), but, among smokers, there were no significant differences in the number of cigarettes/day. Notably, compared with controls, patients with AD less frequently lived in rural areas and small towns and more frequently lived in the Paris area and large towns (data not shown).
Fig. 1. Differences between patients with atopic dermatitis and controls.
Skin pain was reported by 54.6% of patients with AD (n = 101, VAS 5.91/10) and 6.0% (n = 195, VAS 4.34/10) of controls (p < 0.0001). According to DN4 scoring, a neuro-pathic component of pain was detected more frequently in patients than in controls (73.6 vs. 48.2%, p < 0.002).
Among patients, the mean age of those reporting skin pain was lower (39.7 ± 14.5 years) than those without skin pain (44.15 ± 15.3 years; p < 0.05). There was no significant difference regarding sex. Patients with painful AD were more likely to have consulted a dermatologist in the previous 3 months (68.3%) compared with patients without skin pain (36.9%; p < 0.001) as well as general practitioner (98% vs. 92.9%; p = 0.04). The number of consultations with dermatologists and general practitioners was also higher among patients with painful AD. Patients with painful AD were more likely to be smokers (49.5% vs. 25%; p < 0.002).
HRQoL was altered more in patients with skin pain. There were no significant differences in the PCS-12 scores, whereas there were significant differences in the MCS-12 (37.7 vs. 42.3; p < 0.001) and DLQI scores (15.2 vs. 8.8; p < 0.00001).
Finally, univariate analysis showed that atopic patients declaring they had skin pain had more frequent consultations with dermatologists (OR 3.69 (95% CI 2.60–7.80); p < 0.001), were more likely to be smokers (OR 2.94 (95% CI 1.57–7.52); p<0.001), and had more alterations in their HRQoL, as measured by DLQI (OR 6.34 (95% CI 3.28–12.27); p < 0.001) and MCS-12 (OR 0.31 (95% CI 0.13–0.73); p < 0.01). Multivariate analysis showed differences only for DLQI and consultations with a dermatologist (Fig. 2).
Fig. 2. Multivariate analysis of differences between patients with atopic dermatitis who had skin pain and those who did not have skin pain. CI: confidence interval.
This study confirmed that almost 4% of the French adult population report having AD (11), that adult patients with AD are more likely to be smokers than controls (20), and that urban living is associated with a higher prevalence of AD (21), which is probably related to outdoor pollution (22, 23).
More than half of the patients with AD reported experiencing skin pain, with a mean level of almost 6/10. In previous studies, performed on selected cohorts, 42.7% (9) to 78% (10) of patients reported pain. The main strengths of the methodology of the current study include the absence of selecting patients according to recruitment for a particular department and comparison with controls.
Since we completed this research, a new study has been performed on 602 adult patients (according to modified UK Working Party Criteria), which found that 61% of patients reported experiencing pain due to AD (24). The new study was a cross-sectional, US population, internet survey-based study without comparison with healthy subjects. Among those patients experiencing skin pain, 48% reported pain occurring only after frequent scratching, 42% reported intermittent pain, and 11% reported constant pain throughout the day. AD pain was most commonly associated with open areas caused by scratching (27%) and fissures in the skin (27%), followed by inflamed red skin (25%), with only a minority reporting pain mostly caused by burning from creams or ointments (10%). Mild AD was associated with more pain from scratching, whereas severe AD was associated with more constant pain and pain from inflamed skin.
AD patients with chronic itch may scratch their skin, which results in skin-barrier disruption and painful erosions or infections. Infections, and mainly erosions and excoriations, may explain skin pain in atopic patients. However, it is not the only mechanism for such pain, since patients report that skin pain is not only related to skin excoriations, and it is common in patients without excoriation (9).
Indeed, a neuropathic component was suggested in the majority of patients according to the DN4 question-naire. Pain was commonly described as “burning” and “stinging” by patients with AD (10), and these patients usually describe their pruritus as painful, throbbing, biting, stinging, burning, sharp, tingling, pinprick-like, and/or associated with crawling sensations (9, 25–27). All these clinical characteristics suggest that itch could be partially (but probably not entirely) neuropathic (28). It is notable that some neuropathic pain was also found in many controls. Some of the controls could have neuropathies, but we suggest that the large majority could have sensitive skin (29), which is very common (30).
From a neurophysiological perspective, a long-lasting inflammatory response from chronic AD lesions may cause sensitization of the peripheral and central nervous system, which increases patients’ experience of pain (31). Increased intralesional and extralesional sensitivity to mechanical pain in patients with AD compared with controls suggest sensitization of mechano-sensitive circuitry not normally associated with itch (32). Contrary to previous studies underlying an increase in skin innervation in skin lesions (33), new data using 3-dimensional optical clearing and imaging show a decrease in epidermal innervations inside and outside skin lesions (34). Such downregulation is commonly observed in small-fibre neuropathies, which commonly induce neuropathic pain (35, 36).
We consider that the presence of pain inside and outside of skin lesions in AD is probably related to neurogenic inflammation (37–39). The assessment of neuropathic pain in this study and others (9, 10, 32) supports this hypothesis. The epidermis interacts closely with nerve endings, and both the epidermis and nerves produce substances for mutual interactions (40). We are starting to understand the intricate connections between the skin neurones and resident skin cells and how their interaction could be crucial for controlling inflammation and involved in the pathogenesis of diseases such as AD (37, 41, 42).
There is a vicious feedback loop between AD, itch and pain, and it is essential to interrupt this circle through effective treatments for AD, itch and pain. Pain generally inhibits itch, even when the pain stimuli precede the itch provocations (43); however, this is probably not the case in AD. Patients with AD exhibit considerable somatosensory aberrations to cutaneous stimuli, among which pain and itch can notably exist concomitantly, which is difficult to explain without considering a maladaptive central processing of itch, and leads to a blunting of normal pain-induced itch suppression (43). In this context, it is necessary to ascertain whether patients experience itch and pain simultaneously or more sequentially, i.e. as bouts of itch, resulting in scratching that subsequently cause pain (which then wanes as the sequence repeats itself) (43).
Univariate analysis showed that atopic patients with skin pain were more likely to be smokers. More intense pain is known to be associated with variables related to smoking severity (years as a daily smoker, current cigarettes per day, cigarettes per day during the heaviest lifetime smoking period, and current level of nicotine dependence), and these associations persist when taking into account the variance accounted for by sex and negative affectivity (44). On the other hand, there is increasing evidence to show that pain can motivate cigarette smoking behaviour, smokers have reliably endorsed the use of tobacco to cope with pain, and there is reason to suspect that pain may impede smoking cessation (45).
From the patient’s point of view, it is also necessary to stop both AD and pain. Indeed, patients with skin pain more frequently consult dermatologists and general practitioners, and their HRQoL is more affected, as shown by the current study. To the best of our knowledge, skin pain has not been evaluated in clinical trials, and there is an urge to include it in patient-related outcomes. The current study evaluated skin intensity at almost 6/10, which could justify very effective painkillers and/or treatments of AD, especially biologics. Patients, especially those with severe AD, are probably undertreated, since a recent study showed that the use of pain medication was not increased in patients with AD (46).
AD alters HRQoL and is a severe burden on patients, with consequences on sleep and sexual life, and is frequently associated with psychiatric comorbidity (47–50). To date, those were considered to be consequences of itch and alterations in body image; however, pain probably also has an impact. There is a need to measure pain intensity in all patients and to include such measurements in all studies on the burden of AD.
The main limitation of this study is that the diagnosis of AD was not given by doctors, but by patients. Consequently, data on skin lesions and severity of the disease was collected. However, many studies previously used surveys to assess or approach the prevalence of AD, contact dermatitis, psoriasis or other skin diseases (11, 51–56). Surveys are crucial tools in medical research and have been used in dermatological studies to assess the morbidity rates of various skin disorders. Online surveys in dermatology research have many advantages, such as higher response, lower cost, better data quality and time-saving, and these advantages outweigh the concerns regarding security and selection bias (56).
In conclusion, this study showed that skin pain is reported by more than half of the patients with AD, at a pain intensity of almost 6/10 and with consequences on HRQoL. The pathophysiology of AD remains unclear. The management of skin pain is an unmet need, and future clinical trials should take pain in AD into account. It is time that pain in AD is addressed (57).


 Click to show fullsize
Click to show fullsize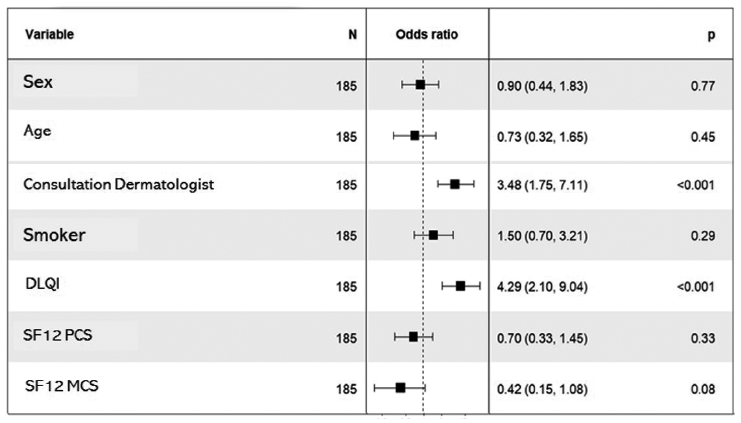 Click to show fullsize
Click to show fullsize