


Department of Dermatology, Kosin University College of Medicine, 262 Gamcheon-ro, Seo-gu, Busan, 602-702, Korea. *E-mail: ksderm77@unitel.co.kr
Accepted May 26, 2020; Epub ahead of print Jun 3, 2020
Acta Derm Venereol 2020; 100: adv00200
Non-tuberculous mycobacteria (NTM) are a heterogeneous group of acid-fast bacilli other than Mycobacterium tuberculosis and M. leprae (1). The increasing prevalence and incidence of NTM disease have highlighted the importance of this challenging diagnosis, which requires a high index of suspicion (2). M. marinum is the most common pathogen in cutaneous NTM infection. As indicated by its names “fish-tank granuloma” and “swimming pool granuloma”, it is associated with exposure to water. Clinical manifestation usually appears on an upper extremity presenting solitary, dusky red, crusted or hyperkeratotic nodules, plaques, and ulcers. Less commonly, NTM can present sporotrichoid spread, abscesses, cellulitis, and draining sinuses (1). Although there are several reports on the histological findings of NTM, no pathognomonic feature that differentiates it from other bacterial and fungal infections has been established (3–5). We report here a case of M. marinum infection that shows clinically diffuse involvement with an unusual spreading pattern and histologically mimics cutaneous tuberculosis.
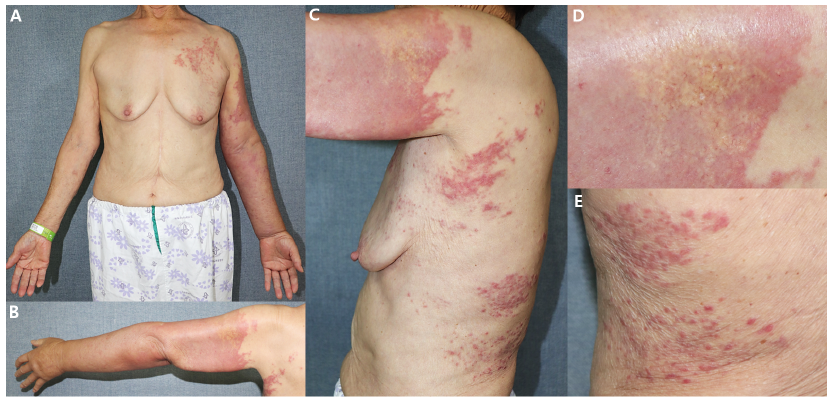
A 74-year-old woman was referred to a tertiary hospital with diffuse tender erythematous and yellow cellulitis-like patches on her left arm, together with discrete papules on the left trunk (Fig. 1A–C). The condition had been treated as cellulitis, but the symptoms worsened. Six weeks previously, erythematous changes in the left forearm with marked oedema developed. Four weeks after onset, the cutaneous lesions slowly enlarged to the proximal area, and multiple erythematous papules on the trunk appeared. Her occupation was trimming oysters, and she reported a history of local steroid injection in the elbow to treat arthritis. She had undergone surgery for gastric cancer 20 years previously.
Fig. 1. Clinical features. (A, B) Diffuse tender erythematous and yellow cellulitis-like patches on the left arm. Marked oedema on the left arm is contrasted with the right arm. (C) Yellowish atrophic scars and erythematous active lesions were interspersed with numerous telangiectasia on the proximal area of the left arm. Multiple erythematous papules on the trunk were seen. (D, E) Close-up view of the yellowish atrophic scars and erythematous papules, respectively.
To diagnose her unusual lesion, skin biopsy was performed. Histopathological findings showed epithelioid granuloma with caseous necrosis in the upper dermis, and mixed cell infiltration with vascular proliferation in the deep dermis (Fig. 2A). Under higher magnification, caseous necrosis, palisading epithelioid histiocytes, multinucleated giant cells, perivascular lymphocytic infiltration, and dermal fibrosis were observed (Fig. 2B, C). Periodic acid-Schiff (PAS) staining was negative, and Ziehl–Neelsen staining revealed a few acid-fast bacilli on both specimens from the arm and trunk lesions. Based on the histopathology, cultures and the real-time polymerase chain reaction (PCR) test for mycobacteria were carried out. No bacterial growth was seen at 37°C. After 2 weeks of incubation at 30°C, 3% Ogawa media presented whitish colonies that turned yellow under direct exposure to light. In the PCR sequencing, genomes matched with M. marinum. Computed tomography scan and magnetic resonance imaging (MRI) suggested bursitis and soft-tissue swelling without systemic involvement. After 3 months of combination therapy with doxycycline, clarithromycin, and rifampin, the patient showed moderate improvement and was lost to follow-up.
Fig. 2. (A) Histopathology revealed epithelioid granuloma with central necrosis in the upper dermis, mixed cell infiltration with vascular proliferation in the deep dermis (original magnification, ×40). (B) Under higher magnification, caseous necrosis, palisading epithelioid histiocytes, multinucleated giant cells, perivascular lymphocytic infiltration, and dermal fibrosis were seen (original magnification, ×100). (C) Mixed cell infiltration with vascular proliferation in the deep dermis was noted (original magnification, ×100).
NTM is subdivided into 4 categories according to growth rate and pigment formation. Among these groups, M. marinum belongs to Runyon group I, which grows and forms yellow pigment under light in 10–28 days (6). Due to its optimal growth temperature of 30–32°C, M. marinum infection tends to be localized on the inoculated skin and not to spread beneath the subcutaneous tissues (6).
In the patient reported here, yellowish atrophic scars and active erythematous lesions were interspersed with numerous telangiectasia on her left arm. The lesions were diffuse and spread to the proximal area despite conventional treatment. The peculiar “wolf-bitten” appearance, previous non-response to antibiotics and the histopathological finding of caseous necrosis gave rise to suspicion of cutaneous tuberculosis. Caseous necrosis does not usually appear in M. marinum infection (6–8); it has been reported occasionally, and is little-known. It is easier to consider it as a classic histological symptom of cutaneous tuberculosis (5, 9). Differentiation of these 2 diseases is essential, since the primary therapeutic option is different. Thus, microbial culture is mandatory, and clinicians should take care to specify appropriate culture conditions and avoid empirical anti-tuberculous treatment.
Based on the patient’s occupation, minor trauma was suspected as the portal of entry. In addition, whether it was an id reaction or a true infection would account for the late-developing papules on her trunk. Ziehl–Neelson staining revealed acid-fast bacilli on a specimen from lesions of the trunk, as well as from the arm, suggesting occurrence secondary to auto-inoculation or lymphatic/haematogenous spread. With no surface changes of erosion or ulceration, autoinoculation is less likely. The eccentric “birds in flocks” distribution on the patient’s trunk is unusual, since the lymphocutaneous pattern of sporotrichoid spread in M. marinum presents nodules or ulcers arranged in rows, and M. marinum cannot thrive at the core body temperature (9, 10). This clinical pattern does not fit localized or disseminated forms, which have multiple lesions on the contralateral side of the body. The diffuse deep involvement of the arm and the “birds in flocks” spread pattern of papules with only a moderate response may be due to the delayed diagnosis and local injection of steroid. Although many patients with M. marinum infection present suspicious risk factors that alert the physician, it is difficult to suspect the disease at an initial encounter. Understanding the various clinic-histopathological findings of NTM infection will enable a high index of suspicion and timely diagnosis with proper treatment.


 Click to show fullsize
Click to show fullsize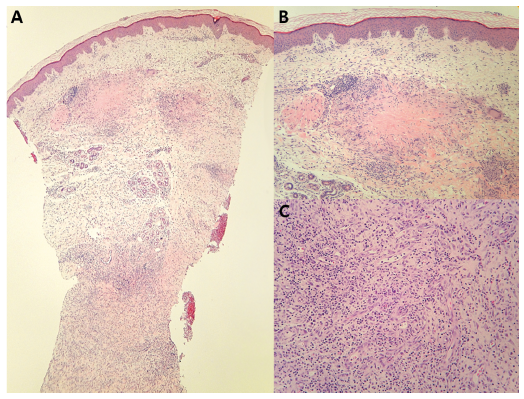 Click to show fullsize
Click to show fullsize