


Departments of 1Dermatology, 2Plastic Surgery and 3Diagnostic Pathology, Sapporo City General Hospital, North 11 West 13, Chuo-ku, Sapporo, 060-8604, 4Department of Pathology, Saitama Medical University, International Medical Center, Saitama, and 5Honma Dermatology Clinic, Sapporo, Japan. E-mail: yfujita@med.hokudai.ac.jp
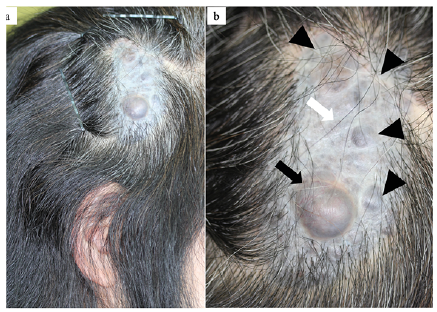
A 54-year-old Japanese woman presented with multiple nodules arising within a hairless birthmark on her head. On examination, multiple greyish-black dome-shaped nodules, the largest measuring 17 × 16 mm, arising within a 67×40-mm alopecic grey oval plaque were observed on her right temple (Fig. 1). The largest nodule had started to grow rapidly 2 years prior to the presentation. Her past medical history was unremarkable, with no neurological, skeletal or congenital anomalies. There was no relevant family history. Punch biopsies from the largest nodule showed an atypical melanocytic lesion, with the possibility of malignant melanoma (MM), arising on a melanocytic naevus. The entire plaque was excised with a 10-mm margin, and sentinel lymph node biopsy (SLNB) was performed.
A scanning view of the surgical specimen revealed multiple dermal nodules within a melanocytic naevus. The largest nodule was surrounded by a fibrillar capsule, showing sharp demarcation; nodular proliferation of predominantly large epithelioid cells with amphophilic or vacuolar cytoplasm and varying degrees of melanin pigmentation were observed. Although enlargement of nuclei and prominence of nucleoli were observed, the cytological atypia was low-grade and mitotic figures were sporadic, with a mitotic rate of 1 per 10 high-power field (HPF). There were no findings of necrosis or of abnormal mitosis (Fig. 2a). The rest of the nodules showed nodular proliferation of epithelioid cells with enlarged nuclei, the cells had lower cellularity than the largest nodule, and neither nuclear pleomorphisms nor mitotic figures were observed (Fig. 2b). The cells of the melanocytic naevus in the background were forming nests at the level of the dermis, which partly extended into the tendon tissue (data not shown). The surgical margin and SLNB were negative.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical presentation. (a) A hairless plaque on the right temple. (b) Closer observation shows multiple greyish-black dome-shaped nodules (arrowheads). Skin biopsies were taken from the largest nodule (black arrow) and the hairless plaque (white arrow).
Fig. 2. (a) Histopathology of the largest nodule (insert: scanning view). An oval dermal nodule with interior bleeding is observed. The nodule shows sharp demarcation from the adjacent melanocytic nevus. The cells have a predominantly epithelioid morphology, with amphophilic or vacuolar cytoplasm and various degree of melanin pigmentation. Sporadic mitosis figure (arrowhead) is observed, with a mitotic rate of 1 mitotic figure per 10HPFs. (Haematoxylin and eosin (H&E) x 100) (b) Histopathology of other small nodules (insert: scanning view). Proliferation of epithelioid cells with enlarged nuclei is observed. Note that the cells have lower cellularity and atypia than the largest nodule. (H&E x 100).
Acta Derm Venereol 2020; 100: adv00206.
Diagnosis: Atypical (largest nodule) and benign (other nodules) proliferative nodules (PNs) arising within a mid-sized congenital melanocytic naevus (CMN)
The overall histological findings were consistent with multiple PNs, with the largest being atypical PN and the remainder benign PNs, arising within a mid-sized CMN. Immunohistochemical examination showed an elevated Ki-67 index of 7% in the largest nodule vs less than 1% in the rest of the nodules and in the CMN. Melan-A and SOX10 were diffusely positive, and HMB-45 was partially positive, without significant differences between the nodules and the CMN (Fig. 3). No evidence of recurrence or metastasis was observed at 21-month follow-up after the wide excision.
PNs present as one or more small nodules that typically arise within pre-existing large (i.e. 20 cm or larger in diameter) CMN, particularly during infancy and childhood (1). Despite an alarming appearance that resembles MM, PNs have a benign clinical course without recurrence or distant metastases after complete excision. PNs are distinguished from MM by the following histological features: lack of high-grade cellular atypia, lack of necrosis within the nodule, rarity of mitoses, evidence of maturation, lack of pagetoid spread and no destructive expansile growth (2, 3). Neither immunohistochemistry nor fluorescence in situ is able to differentiate PNs from MM (4). In challenging cases, mass spectrometry imaging or comparative genomic hybridization can be used as an ancillary diagnostic technique (5).
Histopathologically, PNs are classified as benign or atypical. The latter are characterized by 2 or more of the following findings: sharp demarcation, expansile growth, epidermal effacement, focal pagetoid spread, mucinosis, variable pleomorphism and a mitotic rate of one or more mitotic figures per 10 HPFs (6). Atypical PNs are considered to be borderline lesions between benign PNs and dermal melanomas (6). In the present case, the largest nodule had 4 characteristic findings of atypical PNs: sharp demarcation, expansile growth, pleomorphism and a mitotic rate of 1 per 10HPFs. The clinical behaviour, without recurrence or distant metastases, in the present case is reminiscent of a benign lesion, which is consistent with previous studies that consider PNs including atypical ones to be benign lesions distinguished from MM.
In conclusion, we report here a case of multiple PNs arising within a mid-sized CMN. Although eruptive nodules arising within a pre-existing CMN require clinicians to exclude malignant skin tumours, attentive histological evaluation is essential to avoid over- or under-diagnosis.
Fig. 3. Immunohistochemical staining of the surgical specimens. Higher Ki-67 positivity (arrowheads) is observed in (a) the largest nodule, compared with (b) other small nodules and (c) the melanocytic naevus (a, b, c: x 200). The largest nodule shows diffuse positivity for (d) Melan-A and (e) SOX10, and partial positivity for (f) HMB-45 (d, e, f: x 100).


 Click to show fullsize
Click to show fullsize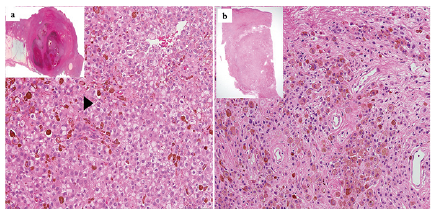 Click to show fullsize
Click to show fullsize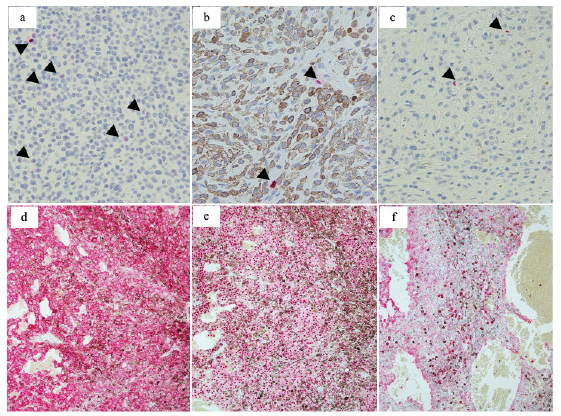 Click to show fullsize
Click to show fullsize