


Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark
Halo naevi are considered benign. They occur in children and adolescents. Eruptive multiple halo naevi are infrequently seen in adults. The first patient in this case series had previously had melanoma. Positron emission tomography-computed tomography (PET-CT) showed a papillary thyroid carcinoma. Subsequent adult patients underwent an examination programme similar to melanoma patients with unknown primary, including PET scanning. Sixteen patients were followed over a 6-year period. In total there were 2 papillary thyroid cancers, 1 neuroendocrine lung tumour, 1 patient had had lung metastases from a thin melanoma 7 years previously, 3 patients had primary cutaneous melanoma (1 had had halo naevi since excision of 2 melanomas 15 years previously) and 1 had melanoma metastasis with unknown primary. The incidence of melanoma was 955 times higher than expected (standardized incidence rate). The benefits of PET scanning must be validated in a controlled trial prior to implementation into clinical practice.
Key words: halo naevus; Sutton naevus; vitiligo; melanoma-associated hypopigmentation; thyroid cancer; neuroendocrine tumour.
Accepted Jun 15, 2020; Epub ahead of print Jun 16, 2020
Acta Derm Venereol 2020; 100: adv00228.
Corr: Henrik F. Lorentzen, Department of Dermatology, Aarhus University Hospital, DK-8200 Aarhus N, Denmark. E-mail: lorentzen@dadlnet.dk
The usual patient with halo naevus is a child or adolescent with a few halo naevi. Occasionally, multiple and eruptive halo naevi may arise in an adult patient. The current recommendation for these patients is a full examination of the skin for melanoma. In this case series, patients were examined using positron emission tomography (PET) scanning, blood tests and capsular endoscopy. A malignancy (3 primary melanomas, 1 melanoma skin metastasis with unknown primary and 1 melanoma lung metastases, 2 papillary thyroid carcinomas and 1 neuroendocrine tumour of the lung) was found in half of the patients, which was more than 100 times higher than expected. If these findings can be substantiated in a controlled trial, clinical practice may be changed for adult patients who present multiple halo naevi in an eruptive pattern.
The aetiology of halo naevi has not been clarified. As in vitiligo, melanocytes are destroyed by cytotoxic T cells. Vitiligo and halo naevi have been linked to treatment success in melanoma patients treated with immune checkpoint inhibitor (ICI), targeting PD-1. ICI treatment success and side-effects are probably related to the mutational burden of the tumour and tumour immunogenicity. Halo naevi normally occur in children (1) or adolescents (2), when a handful of naevi are attacked by an immunological process. Sunburn or mechanical trauma (Koebnerization) are hypothesized eliciting factors, but this has not been substantiated. In patients with only one halo naevus, malignant melanoma with regression must be considered; young age points to a benign halo naevus, whereas older age points to melanoma. Dermoscopy may be helpful (3, 4). When (multiple) halo naevi occur in adults some authorities recommend considering melanoma or vitiligo and recommend examination of the entire skin.
Patients occasionally present to our melanoma screening clinic with melanoma in lymph nodes or distant metastatic disease without known primary tumour. It is recommended that such patients undergo repeated full examination of the skin, including examination of the skin-mucous membrane transition zones near the mouth, perianal skin, penis or vagina, whereas gynaecological examination, ear nose and throat, and ophthalmological examinations are not mandatory (5). Recommendations vary between countries (6), but there is agreement on performing a PET scan and tumour computed tomography (CT) scan, as this is also part of staging the cancer. In this study, this programme was applied in patients with multiple eruptive naevi. Ophthalmological examination and capsule endoscopy were performed to rule out small intestine melanoma (7) and neuro-endocrine tumours of the gut (8).
Patients referred with eruptive halo naevi were submitted to an extensive search for an underlying melanoma or other cancer if they met the following criteria: the majority (> 80%) of their naevi had developed into halo naevi; they were post-adolescent; and they did not have a medical history of treatment with immune checkpoint inhibitors. The examination programme included full clinical evaluation, blood tests (including haematology, leukocyte type and distribution, basic metabolic panel, thyroid function, lactate dehydrogenase (LDH) and chromogranin A). A PET-CT scan and, when appropriate, ultrasound examination or magnetic resonance (MR) scans were performed. In some patients capsule endoscopy (swallowed camera-pill) was performed to rule out small intestine melanoma and neuroendocrine tumour.
Standardized incidence ratios (SIR) were calculated by listing the number of patients in categories defined by age and sex. Expected incidences were calculated using data from the NORDCAN database (9) using 2016 data for Denmark, which is the most recent data available and coincides with the middle of the study observation period.
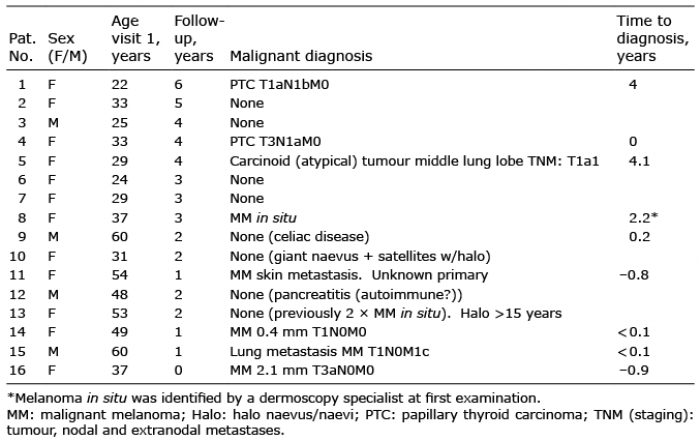
During a 6-year period, 16 patients (4 (25%) males, 12 females) were referred with multiple eruptive halo naevi (Table I). Median age at first visit was 35 years (interquartile range (IQR): 29–51 years). After referral patients were followed for 0–6 years with a median of 2 years (IQR 2–3.5 years). No malignancies were found in 8 (50%) of the patients, although one of these (patient 9) had coeliac disease diagnosed due to low cobalamin blood level and a capsule endoscopy. Another patient (patient 12) developed pancreatitis shortly after referral. Since the age of 19 years, he had had 8 attacks of acute pancreatitis. No gallstones were observed during endoscopic retrograde cholangiopancreatoscopy (ERCP). Biopsies were not performed. He had a slightly raised chromogranin A blood level, which was considered to be unrelated to the pancreatitis. A PET scan did not show any neuroendocrine tumours or other malignancies.
Table I. Patients listed consecutively
Patient 2 had a monozygotic twin sister. Both had atypical naevus syndrome, but only patient 2 developed eruptive multiple halo naevi (Fig. 1). None of her naevi were clinically or dermoscopically suspicious. The twin sister had one suspicious naevus, which showed “compound naevus with atypical proliferation”, previously characterized as dysplastic naevus. Both twins consented to have a naevus or halo naevus stained for PD1, PD1 ligand and PD2 ligand. One of the samples was lost during preparation.
Fig. 1. Patient 2 (right) and her monozygotic twin sister (left). Both sisters had atypical naevus syndrome. The patient developed multiple halo naevi (more than 30 on her back) over a period of 2–4 weeks. She was repeatedly examined using the FotoFinder system and with handheld dermoscopy (Heine T20 (HEINE Optotechnik GmbH & Co. KG, Germany)). No suspicious lesions were found. In contrast, a dermoscopic suspicious lesion was found on her sister. Histological diagnosis revealed compound naevus with atypical proliferation. It may be hypothesized that an immune response to some “stronger” antigen (higher mutational burden or immunological hotter) in the patient with vitiligo, elicited the eruptive halo response. However, no signs of regressing melanoma were found. An immunoprotective effect against melanoma in vitiligo has been suggested (27).
Two patients were diagnosed with papillary thyroid carcinoma (PTC) (Table I). Patient 1 was diagnosed 4 years after the emergence of halo naevi. Patient 4 was diagnosed within 1 month. She had a medical history of superficially spreading malignant melanoma 1.3 mm (T2aN0M0) and therefore a PET scan was performed immediately. During follow-up she was diagnosed with a melanoma in situ. Her brother had had Langerhans cell histiocytosis and therefore she was investigated and found negative for PTEN mutation (seen in Cowden’s syndrome). The PTC and her previous melanoma carried a BRAF v700 mutation, which is also often the case in Langerhans cell histiocytosis, but her brother’s tissue samples were not subjected to BRAF analysis.
Patient 5 (Table I) had had 4 cases of superficially spreading melanomas (0.26 mm (2013), 0.89 mm (2013), 1.07 mm (2013) and 0.45 mm + mitoses (2015)) prior to diagnosis of atypical carcinoid tumour in her middle lung lobe. After lobectomy she had an additional case of melanoma in situ. Prior to the diagnosis of the neuroendocrine tumour she experienced hypoaesthesia and paraesthesia of the skin on her shoulder and deltoid area. She underwent neurological evaluation and MR brain and neck scan, which ruled out brain metastases from one of her previous melanomas. Subsequently she underwent a PET scan that showed tumour activity in the lung. Biopsy confirmed the diagnosis of neuroendocrine tumour. No signs of disseminated melanoma were identified. Chromogranin A blood analysis was not performed.
Patient 15 (Table I) had had a superficially spreading malign melanoma 0.52 mm (T1aN0M0) 7 years prior to the development of multiple eruptive halo naevi and vitiligo-like depigmentation in a pityriasis versicolor-like distribution on his upper back and chest, i.e. melanoma-associated depigmentation (MAL). He also had a melanoma in situ 9 months prior to the halo naevi and MAL. The PET scan showed multiple lung metastases. Biopsy revealed BRAF-positive metastatic melanoma.
Three patients (patients 8, 14 and 16) (Table I) had primary melanomas identified during skin examination and 3 patients (patients 4, 5 and 15) had cutaneous melanomas in addition to another cancer within 1 year before or after referral for multiple eruptive halo naevi.
Blood test (including TSH, LDH, liver and kidney function test, complete blood count and leukocyte differential count) did not point to any of the malignant diagnoses.
Sex did not influence cancer incidence (p = 0.57, Fisher’s exact test, MedCalc®). Patients were distributed equally into 3 age categories (≤ 29 [n = 5]; 29–48 [n = 6] and ≥ 49 [n = 5] years) and no differences were observed (p = 0.82; χ2 test; MedCalc®).
Four patients had had a cancer at least 2 years prior to entering the study: patient 4: malignant melanoma of 1.26 mm + a malignant melanoma in situ after the finding of her PTC. Patient 5: 4 cutaneous malignant melanomas before and 1 malignant melanoma in situ after her lung carcinoid. Patient 13: 2 cases of malignant melanoma in situ. Patient 15: cutaneous malignant 0.52 mm and a malignant melanoma in situ prior to his lung metastases from melanoma. There was no difference between the 4 patients without previous cancers and the 12 patients with previous malignant disease (p = 0.57, Fisher’s exact test) regarding occurrence of cancer concomitant with halo naevi eruption.
SIR for cutaneous melanoma was 955 (95% confidence interval: 262–1.562), i.e. the incidence of cutaneous melanoma related disease was 955 times higher than expected in the multiple eruptive halo naevus group compared with a sex- and age-matched background population (Table II). In the NORDCAN (9) database, data for 2017 and 2018 have not been validated. In this study, incidence rates for 2016 were used. When the expected incidence rates for the 6-year period 2011 to 2016 were used, a very similar SIR was obtained (Table II). Patients were followed from 1 to 6 commenced years, and therefore the expected number of cutaneous melanomas was corrected for person years of observations, i.e. if a patient was followed for 3 years, the expected occurrences of melanoma were calculated as 3 times the yearly incidence rate for 2011 to 2016. SIR for this calculation was 191 (Table II).
SIR for all cancers was 113, i.e. the observed cancer incidence was 113 times higher than expected in the eruptive halo naevi group.
SIR for thyroid carcinomas was 247, i.e. the observed incidence of thyroid carcinomas was 247 times higher than expected in the eruptive halo group. This estimate is lower than would be expected if only papillary thyroid carcinomas were examined. The NORDCAN database, however, do not provide data on subgroups of thyroid carcinomas. Papillary thyroid carcinomas constitute 70% of all thyroid carcinomas.
SIR specifically for neuroendocrine tumours is not provided, as they are not quantified as a separate group in the NORDCAN database.
Table II. Standardized incidence ratio
The aetiology and pathogenesis of halo naevi are not fully known. An antibody response and a cytotoxic T-cell response have been suggested. The antibody theory has been downplayed, because circulating antibodies against epitopes from the melanocyte/naevus-cell/melanoma lineage have been found to be an epiphenomenon. Halo naevi are customarily described as a symmetrical circular loss of pigmentation surrounding naevi of an adolescent. A single halo naevus to a few halo naevi, often located on the trunk, is most common. This may co-exist with the related disease of vitiligo. Treatment recommendations are full examination of the skin to exclude melanoma, reassurance of the patient and a “wait-and-see” approach. In case of a singular halo naevus, where melanoma cannot be ruled out with certainty, excision is recommended. Melanoma with a halo can be segregated from benign halo by dermoscopy (4).
Epstein reported 5 cases of melanoma patients who developed halo naevi in the follow-up period after resection of a primary cutaneous melanoma. Three patients had several to many halo naevi and 2 had a single halo naevus. Mean age was 39.6 years (10).
Kolm et al. (4) reported 86 patients who had dermoscopy performed on 138 halo naevi. No melanomas were found. Mean age was 23.2 years. Two of their patients (age 45 and 58 years) had a personal history of melanoma (4).
One patient (patient 5) was diagnosed with an atypical lung neuroendocrine tumour. Dereure et al. described a patient who developed multiple halo naevi simultaneously with the development of a gut carcinoid tumour (8).
Two of the patients in the current study had PTC (patients 1 and 4) and 1 patient had a benign thyroid adenoma (patient 11) on PET-CT. Patients 4 and 11 both had previous melanoma. Tran et al. performed a meta-analysis of studies on the risk of thyroid cancer in patients who had had a cutaneous malignant melanoma and vice versa, and found increased risk for both directions (11). The authors raised the hypothesis that a common risk factor could explain the bidirectional risk increment. Oakley et al., in the Utah study of bidirectional increased risk of melanoma and PTC, reported high occurrence of BRAF mutations (12). This was also found in patient 4. A proportion of papillary thyroid carcinomas are considered thyroid microcarcinomas, some of which runs an indolent course. Tuttle et al. performed active surveillance using ultrasonography of 291 low-grade PTC, and found a growth of 3 mm or more in only 12.1% of cases. No distant metastases were observed (13). Patient 1 had a PTC stage T1a, meaning that it would be classified as a microcarcinoma with a slow growth rate.
Patient 9 had coeliac disease, diagnosed due to vitamin B12 deficiency and capsule endoscopy. Marthinsen & Nilsson (14) described 3 girls with coeliac disease and halo naevi. One of them had simultaneous onset of the 2 diseases.
Patient 12 developed pancreatitis during follow-up. He had previously had 6 attacks of acute pancreatitis, the first during military service, when he was 19 years old. It remains to be clarified whether he had autoimmune pancreatitis.
Halo naevi belong to the group of dermatoses designated immunological leukodermas, together with vitiligo and melanoma-associated hypopigmentation (15). The convergence theory of vitiligo states that damaged melanocytes induce local inflammation that leads to an adaptive immune response, especially CD8+ T cells (16). Immunohistochemical studies suggested a stronger cytotoxic response (higher prevalence of granzyme and TIA-1) in halo naevi compared with melanoma, but also a higher immune-regulatory mechanism (higher prevalence of PD1) in halo naevi (17), suggesting a feedback mechanism or balance between apoptotic factors and tolerogenic factors. Maleki Vareki proposed a 2×2 cross-tabulation of immunologically hot or cold tumours (i.e. T-cell inflamed) vs tumours with high or low mutational burden (18). Melanomas often carry a high mutational burden and are immunogenic, and, for that reason, a substantial proportion is susceptible to immune checkpoint inhibitors. Ward reviewed carcinogenesis (radiation and in 131I) and infiltration of thyroid carcinomas with immune- and inflammatory cells (19). The selection of a less immunogenic tumour-cells leads to “tumour-escape” from immunological surveillance.
The transcription factor microphthalmia-associated transcription factor (MITF) has a fundamental role in melanocyte differentiation, proliferation and melanin production, also after ultraviolet damage to nearby keratinocytes releasing melanocyte-stimulating-hormone (MSH) leading to MITF activation. Byrne & Fisher provided a teleological interpretation of MITF function: the survival of melanocytes despite accumulation of DNA damage (20). Thus, a balance between cell death caused by apoptosis and cytotoxic action of T-cells and cell survival regulated by MITF exists. MITF upregulation resulted in decreased immune cell migration into tumour in human melanoma cell lines (21). PD-1 blockage shifts the balance towards melanoma cell death, but also melanocyte cell death leading to vitiligo (20) or melanoma-associated hypopigmentation.
Autoimmunity may be explained by 1 of 3 mechanisms: (i) molecular mimicry (structural similarity leads the immune system to attack self-antigens); (ii) epitope spreading (release of antigens normally sequestered intracellularly); or (iii) bystander activation (activation of immunity against “x” during an immune response against “y” due to a substantial inflammatory reaction) (22).
Common susceptibility genes have been suggested to explain the co-occurrence of thyroid disease and vitiligo (23). Presentation of melanocyte-specific antigens on thyroid tissue has also been reviewed as a possible explanation of the bidirectional auto-immunity link between vitiligo and autoimmune thyroid disease (23).
Rosai discussed the ontogeny of neuroendocrine cells and though an origin from the neural crest could not be substantiated by a chick-quail chimera model, he argued that from a histological viewpoint, neuroendocrine cells, especially from the lung, larynx, thyroid C-cells and thymus are neural-like. A small proportion of neuroendocrine tumours contain melanin, otherwise considered specific for the melanocyte lineage (24). Melanocytes, naevus cells and melanoma cells belong to the same lineage (25) and share antigens. Eighty percent of benign melanocytic naevi carry a BRAF mutation and 5.9–18.2% carry an NRAS mutation, and it is hypothesized, that naevi develop from BRAF-mutated melanocytes, that after a period (weeks to months) of proliferation enter a phase of growth arrest, oncogenic-induced senescence (26). BRAF-mutated naevus cells express specific antigens. This may contribute to the understanding of the difference between halo naevi (naevus cells + “spill-over” to melanocytes of adjacent skin) and vitiligo (melanocytes).
Selection bias is an inherent risk for case series. Patients with previous melanoma may participate in a follow-up programme, and, for that reason, the reference threshold to a tertiary skin cancer screening clinic might be lower. Diagnostic suspicion bias was a particular risk in this case study, as a proportion of patients had a personal history of melanoma, e.g. patient 5 had a PET scanning performed due to previous melanoma, which revealed the neuro-endocrine tumour. Suspicion was not raised due to positive chromogranin A blood test, which was not performed. A possible value of PET scanning cannot be inferred from this case series, as PET scanning, in itself, was used as the gold standard for the examination programme for patients with previous melanoma and eruptive naevi was a simultaneously occurring phenomenon. The circularity of this incorporation bias hampers conclusions regarding the value of PET scanning for the medical indication of eruptive halo-naevi in adults. In order to develop multiple halo naevi, the patient would have to present with multiple naevi. Atypical naevus syndrome or multiple sun-induced naevi, both, in themselves, increase melanoma risk. The incidental finding of melanoma, neuroendocrine tumour and papillary thyroid carcinoma might be caused by a silent phase of the cancers and the screening procedure incur a lead-time bias.
In conclusion, this study found a substantial excess incidence of melanoma (SIR=955) and cancer overall (SIR=113). There is a theoretical background for the development of halo naevi as an immunological cross-reaction to melanocytic and other cancers. Melanoma-associated hypopigmentation during ICI treatment supports this. The halo reaction studied in this case series was much more pronounced than is normally expected in patients with halo naevus. Case series can be biased (including spectrum bias) for various reasons and the value of an examination programme needs validation in controlled trials before incorporation into clinical practice.
The author has no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize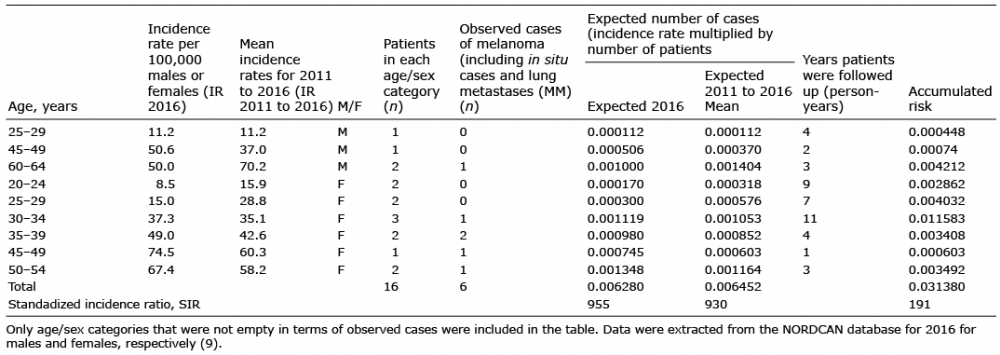 Click to show fullsize
Click to show fullsize