


Departments of 1Dermatology, 2Internal Medicine and Infectious Diseases and 3Pathology, University Hospital Center of Tours, FR-37044 Tours Cedex 9, and 4INSERM 1246-SPHERE, University of Tours, Tours, France. E-mail: annabel.maruani@univ-tours.fr
A 20-year-old woman presented at the dermatology department with multiple crusted ulcerations of the limbs. The lesions first appeared one month earlier during her stay in an isolated bush village in Guinea. Before her journey, she had all mandatory and recommended vaccines. The condition began a few weeks after her arrival in Guinea, with painful erosions and crusts on the lower limbs, spreading to the upper limbs. She had no fever and she was the only one in her family affected. Most of the lesions remained stable until her return to France, but some had healed without scars; no conventional treatment was administered.
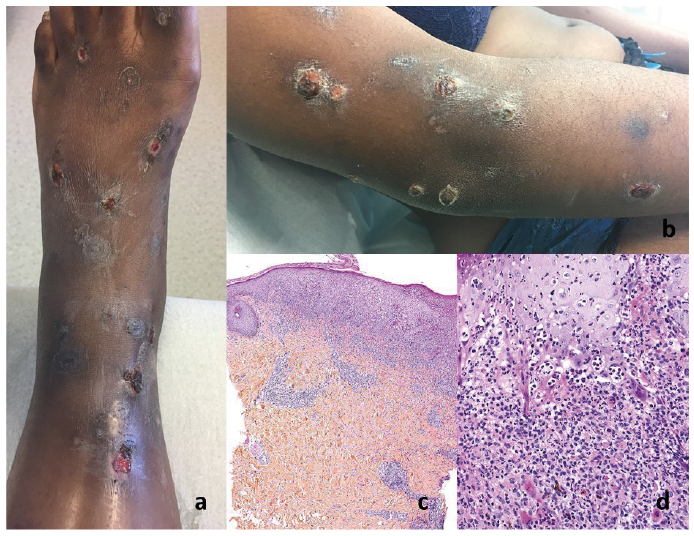
At consultation, she presented a dozen ulcerations, crust-covered, with surrounding inflammatory swollen skin (Fig. 1a, b). One pustule was noted on the forearm. The ecthyma had no associated fever or other symptoms.
Blood laboratory tests, including complete blood count cell and inflammatory marker testing, were normal. Microscopy examination of skin samples showed a dermal infiltrate with mixed inflammatory cells (Fig. 1c, d). Periodic acid-Schiff and Gram staining were negative. With direct bacteriological examination, a non-capsulated Gram-positive pathogen was found.
What is your diagnosis? See next page for answer.
Fig. 1. Erosions and crusts on the lower (a) and upper (b) limbs of a 20-year-old woman returning from Guinea. Inflammatory infiltrate of the dermis constituted of mononuclear cells, histiocytes and numerous polynuclear neutrophils (haematoxylin eosin saffron staining) (d, ×20), underlying a thickened and ulcerated epidermis (c, ×2.5).
Acta Derm Venereol 2020; 100: adv00253.
Diagnosis: Cutaneous diphtheria
Cultures of skin swabs and biopsies revealed Corynebacterium diphtheriae as well as Streptococcus pyogenes and Staphylococcus aureus. PCR testing for diphtheria toxin was positive, but PCR testing of a throat swab was negative for C. diphtheriae. She had no respiratory symptoms or strep throat indications. There were no respiratory signs, and cardiology and neurology examinations were normal. She was hospitalized and received oral amoxicillin, clavulanic acid and clindamycin for 14 days and was isolated. The treatment course was favourable in less than one week.
None of the patient’s family exhibited symptoms. Considering the positive PCR test for diphtheria toxin, the family members received preventative treatment with amoxicillin, as did the hospital staff who took care of the patient before the diagnosis.
Cutaneous diphtheria is the most frequent extra-ENT presentation of diphtheria, an infectious disease caused mostly by C. diphtheriae (1, 2). Carriage of diphtheria is high in endemic countries, so most affected patients are travellers returning from an endemic country, regardless of their vaccination status (3, 4). Cutaneous diphtheria presents with multiple chronic and haemorrhagic cutaneous erosions, which are often painful. Diagnosis is based on culture of skin samples, and the presence of diphtheria toxin must be assessed quickly by PCR or Elek test (2). The standard treatment is penicillin antibiotics, and diphtheria antitoxin must be discussed in cutaneous forms caused by toxigenic bacteria.
This case highlights this typical form of a rare infectious condition in western countries, which must not to be forgotten when presented with returning travellers.


 Click to show fullsize
Click to show fullsize