


1DiSSal Section of Dermatology, University of Genoa, IRCCS San Martino Policlinic Hospital, IT-16132 Genoa, 2Section of Dermatology, IRCCS San Martino Policlinic Hospital, 3Clinical Immunology Unit, Department of Internal Medicine, University of Genoa and IRCCS San Martino Policlinic Hospital, Genoa, and 4UOC Dermatology, University of Catania and Vittorio Emanuele Hospital of Catania, Catania, Italy. *E-mail: emanuele.cozzani@unige.it
A 24-year-old woman presented with a 2-year history of spontaneous, painful, swollen erythematous lesions, rapidly progressing to ecchymosis, on her legs. The lesions had arisen together with fever and arthralgia, recurring repeatedly in the absence of trauma. She had no personal or family history of bleeding disorders. She had already undergone 2 skin biopsies. The first biopsy showed lymphohystiocytic and neutrophilic infiltrate in fat tissue. On suspicion of panniculitis she had been treated with prednisone, 25 mg/day, with no improvement. The second biopsy, showed oedema, haemorrhage and dense neutrophilic, as well as eosinophilic, infiltrate in upper dermis without vasculitis, which led to a diagnosis of Sweet’s syndrome; treatment with prednisone 50 mg/day, had been ineffective.
On admission, 2 20-cm wide ecchymotic lesions were present on her lower abdomen, and smaller ones on her right arm and chin (Fig. 1). She reported headache, abdomen and back pain, severe asthenia, lower limbs hyposthenia and pain with consequent inability to stand or walk, and epistaxis. Physical examination, extensive imaging, neurophysiological and laboratory studies, including coagulation panel, showed no abnormalities. A third skin biopsy showed perifollicular lymphocytic infiltrate and rare eosinophil cells.
What is your diagnosis? See next page for answer.
Fig. 1. Ecchymotic lesion on chin.
Acta Derm Venereol 2020; 100: adv00246.
Diagnosis: Gardner-Diamond syndrome
An intradermal injection of 0.1 ml autologous washed -erythrocytes on the left forearm, with saline isotonic solution as a control on the right forearm (with the patient blinded to the location of each injection) resulted in development of an ecchymotic lesion on the left forearm (Fig. 2). A diagnosis of Gardner-Diamond syndrome (GDS), also known as psycho-genic purpura, was made. The patient was referred to a psychiatrist, who diagnosed anxious-depressive syndrome. It emerged that she had witnessed her father’s death one year before the first lesions appeared. She was started on lorazepam and paroxetine and underwent psychotherapy. One year later, she had recovered from her symptoms, maintaining just a slight difficulty in fast walking.
GDS was first described in 1955 in a cohort of 4 females with painful ecchymotic lesions (1). Characteristics of patients with GDS have been reviewed recently (2). They are mostly young women, often showing psychiatric disorders; frequently, a trigger factor is recognized, commonly an emotional stress. Systemic symptoms are not uncommon, as well as bleeding from other sites, with normal platelets and coagulation examinations. Neurological symptoms have been reported infrequently (2).
The diagnosis is one of exclusion (2). In our case, laboratory and instrumental examinations, along with histopathology, allowed us to rule out platelet disorders, coagulopathies, vasculitis and other rheumatological conditions. Factitious purpura was excluded by close patient observation, confirmed by psychiatric evaluation.
Psychological and immunological factors have been proposed as pathophysiological mechanisms of GDS (3, 4). Autosensitization towards components of erythrocytes, have been described: Gardner & Diamond reproduced the lesions by intradermal injection of erythrocytic stroma (1, 3). This technique, the autoerythrocyte sensitization test, is often used to confirm the diagnosis, although its reliability is controversial (2, 3). Nonetheless, psychological factors are used to name this condition (psychogenic purpura): it has been hypothesized that stress and depression could alter the haemostatic equilibrium by increasing oxidative damage and vascular permeability (4).
This case was a challenging one to diagnose, because of the predominant, various systemic and neurological symptoms, as well as the unusual histopathological findings. Together, these had led to the wrong diagnoses of panniculitis and Sweet’s syndrome. GDS should always be considered in cases of unexplained bruising.
Fig. 2. Ecchymosis on left forearm after intradermal injection of autologous erythrocytes.


 Click to show fullsize
Click to show fullsize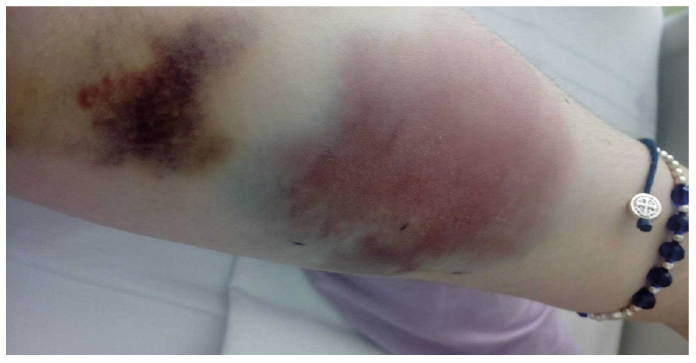 Click to show fullsize
Click to show fullsize