


1Dermatology Unit, Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy, ERN SKIN and VASCERN VASCA European Reference Centre, 2Paediatric Dermatology Department, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, VASCERN VASCA European Reference Centre, 3Department of Adult and Pediatric Dermatology, Bordeaux University Hospitals, Bordeaux, France, 4Dermatology, Department of Experimental, Diagnostic and Specialty Medicine, University of Bologna, Bologna, Italy, ERN SKIN European Reference Centre, and 5Neuroradiology Unit, Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy
#These authors contributed equally to this paper.
Infantile haemangiomas are very common benign tumours in the first months of life. They are mostly cutaneous; however, extracutaneous lesions are possible, and occur in very rare cases in the central nervous system. A European multicentre observational retrospective study was conducted in the last 5 years. Seven patients with intracranial or intraspinal infantile haem-angiomas were selected and treated with oral propranolol. Propranolol was interrupted after complete or almost complete resolution of infantile haemangiomas. All patients tolerated the treatment well without side-effects. Central nervous system infantile haemangiomas are probably underestimated due to the frequent absence of symptoms and their spontaneous involution. However, they should be investigated in case of segmental cutaneous infantile haemangiomas, particularly on the head, neck, upper trunk, lumbar or sacral area in order to diagnose intra-central nervous system involvement at an early stage.
Key words: infantile haemangioma; central nervous system; oral propranolol.
Accepted Jul 9, 2020; Epub ahead of print Jul 31, 2020
Acta Derm Venereol 2020; 100: adv00255.
Corr: Claudia Carnevale, Dermatology Unit, Bambino Gesù Children’s Hospital, IRCCS, Piazza S. Onofrio, 4, IT-00165, Rome, Italy. E-mail: claudia.carnevale@opbg.net
Infantile haemangiomas are the most common tumour in infancy. They are frequently cutaneous; however, they have also been reported in the central nervous system in rare cases. Seven patients with intracranial or intraspinal infantile haemangiomas were selected and treated with oral propranolol, without side-effects. At the end of therapy a good response of both cutaneous and intra-central nervous system components was reported. Central nervous system infantile haemangiomas are rare, but it is important to consider them in the case of large or segmental cutaneous infantile haemangiomas, particularly those on the head, neck, lumbar/sacral area.
Infantile haemangiomas (IHs) are the most common tumour in infancy, affecting 5–10% of Caucasian infants. Family history of IHs, low birth-weight, prematurity, female sex, intrauterine complications, multiple gestations, placental anomalies and advanced maternal age are risk factors for development of IHs (1–5). IHs are mostly cutaneous; however, extracutaneous lesions have been reported in liver, parotid and larynx, and very rarely (1%) in the central nervous system (CNS) (6–10).
Surgery, endovascular embolization, corticosteroids, α interferon, and vincristine have been the therapeutic options reported before the propranolol era. Propranolol is a beta-blocking agent, which is safe and highly effective in treating cutaneous and extracutaneous IHs. Only a few cases of CNS IH treated with propranolol have been reported (10–12). A few other cases of CNS IH described in the literature have been treated with corticosteroids, interferon, thalidomide, embolization or surgery (9–10, 12–16). Spontaneous involution has been also reported (9, 17).
We report here a case series of 7 patients with cutaneous and CNS IHs, treated successfully with oral propranolol.
A European multicentre observational retrospective study was conducted between 2015 and 2019. Cases with intracranial or intraspinal IHs were selected from the local databases of 4 European reference centres for vascular anomalies: 2 Italian (Bambino Gesù Children’s Hospital, Rome and University of Bologna), 1 Spanish (Hospital de la Santa Creu i Sant Pau, Barcelona), and 1 French (Bordeaux University Hospitals).
Large or segmental cutaneous IHs, involving the head, neck, lumbar or sacral area, were clinically diagnosed and screened using magnetic resonance imaging (MRI) for PHACES or LUMBAR/SACRAL syndromes revealing intracranial or intraspinal IH. All patients underwent oral propranolol treatment due to high-risk cutaneous IHs. Six patients were treated at 2 mg/kg/day, and one patient at 3 mg/kg/day. The treatment was initiated between 3 and 7 months of age and the duration was 6–14 months based on clinical response and imaging. A monthly clinical follow-up was performed and a brain/spinal MRI was repeated after 5–6 months of treatment. Propranolol was interrupted after complete or almost complete resolution of cutaneous and intra-CNS component, documented clinically and by MRI, respectively.
Seven female infants (mean age 3.7 months), with cutaneous and CNS IHs were identified among patients referred to 4 European paediatric reference centres for vascular anomalies. Five out of 7 patients presented at least 1 risk factor for developing IH (Table I).
Table I. Risk factors for development of infantile haemangiomas
Three IHs were segmental, one multifocal in a segmental pattern and 3 indeterminate. Two cutaneous IHs were located on the sacral and lumbar area and associated with an intraspinal IH. The others were on the head and/or face (Fig. 1a) with an intracranial component (Fig. 2a) except patient 2 with an intraspinal involvement (Fig. 2c). In this case, the cutaneous component was on the right preauricular area, lips and sternum (Fig. 1b) distributed in a segmental pattern. In patient 3, with a cutaneous infantile haemangioma on the right buttock, the intra-spinal involvement was associated with an asymptomatic primary tethered cord with low-lying conus medullaris. Surgical treatment was postponed after treatment with propranolol to avoid intraoperative bleeding.
Five patients had a complete or almost complete resolution of the cutaneous IHs after propranolol treatment. All CNS lesions responded to treatment (Fig. 2b, d) (Table II): patient 3 had complete regression of the tumour and then underwent successful neurosurgery. None of the patients presented severe side-effects.
Fig. 1. (a) Patient 1. Mixed large segmental infantile haemangioma (IH) of the neck and occipital area. (b) Patient 2. Multiple IHs distributed in a segmental pattern in an infant of 3 months of age: superficial lesion on the sternum, mixed on the lower lip and right pre-auricular area (arrow).
Fig. 2. Axial post-gadolinium T1WI of posterior fossa before and after treatment. (a) A well-circumscribed extra-axial contrast enhancing mass located in the right cerebellopontine angle cistern extending to the internal auditory canal and through the foramen of Luschka to the fourth ventricle. (b) An almost complete resolution of the lesion; only a small contrast enhancing nodule is evident in the internal auditory canal. (c) Axial post-gadolinium T1WI of the thoracic spine before and after treatment: a contrast enhancing mass located in the right costo-vertebral angle with intraspinal (extradural) extension through the neuroforamen. (d) Complete resolution of the lesion.
Table II. Patients’ features
CNS IHs are extremely rare, but probably underestimated due to the frequent absence of symptoms and spontaneous involution. They are usually incidentally diagnosed with MRI performed in large/segmental cutaneous IH on the head, neck, upper trunk and lumbar or sacral area to rule out a syndrome (3). Moreover, in PHACE syndrome, the incidence of intracranial IH is greater than the other associated anomalies (7). Orbital IH may be associated with intra-CNS component, as reported in the literature and observed in patients 5 and 7 (8). Thirteen cases of cutaneous IHs with intra-spinal involvement have been reported in the literature (6, 9, 11, 13, 17). Interestingly, 3 patients (6, 9) presented cutaneous IH on the face, while the intra-spinal localization was at the cervical and dorsal level. Overall, these patients suggest that in the case of segmental IH of the head, MRI should be always extended to the spine. In our population, 3 patients presented an intra-spinal involvement: 2 of them (patients 4 and 6) unexpectedly manifested a focal cutaneous IH, in the third patient the skin lesion was multifocal and distributed in a segmental pattern (patient 2). This last patient may suggest that in case of multifocal cutaneous IHs in a segmental pattern (as shown in Fig. 1b) radiological investigations should be performed to rule out an intra-CNS involvement. Some authors reported patients with severe neurological symptoms treated surgically for suspected brain tumours, in which histology and immunohistochemistry (Glut 1 +) confirmed IHs diagnosis (10, 12). Indeed, IHs should be considered in differential diagnosis with other brain tumours (haemangioblastoma, medulloblastoma, and soft tissue sarcoma), vascular malformations (cerebral-cavernous or artero-venous malformations), and congenital haemangiomas (6). Rapidly involuting congenital haemangiomas (RICHs) are usually diagnosed during pregnancy through ultrasound echography, they are Glut 1 negative, not sensitive to propranolol, and characterized by a rapid spontaneous involution (3). The diagnosis of CNS IHs is performed by MRI, which documents well-circumscribed extra-axial masses with high signal intensity on T2 and isointensity on T1, with contrast enhancement (6, 9). In children with asymptomatic intra-CNS mass and doubtful MRI images, response to propranolol could be a clue for the diagnosis avoiding biopsy.
None of the patients in the current study was symptomatic, while some authors reported neurological disorders in patients with CNS IHs (e.g. development-delay, seizures, hypotonia, optic nerve atrophy) (6, 7, 10, 12, 15, 16). These patients demonstrate that CNS-IH is a potentially functional damaging lesion.
A small number of CNS IH have been reported in asymptomatic patients with diffuse neonatal haemangio-matosis (10). Thus, in asymptomatic newborn with haemangiomatosis, brain MRI is not indicated (3). Finally, intracranial IHs has been reported in symptomatic patients without cutaneous lesions (12).
Viswanathan et al. (6) described intracranial IHs in the posterior fossa, pineal region, hypothalamus, hippocampus, and the cerebellar convexity, without parenchymal invasion; in our patients, they were localized in the internal auditory canal, cerebellopontine angle, temporal fossa, and extradural spine, according to the cases reported by Hernandez-Martín &Torello (9).
Oral propranolol is the first line therapy for IHs during proliferative phase, having demonstrated efficacy, safety and tolerability (1–4). It is indicated for life-threatening, functional damaging and disfiguring infantile haeman-giomas. Ghosh & Ghosh (11) described, in 2011, the first case of intraspinal IH treated with propranolol and Kang et al. (12) reported in 2016 the first intracranial IH successfully treated with propranolol. Since in literature several intracranial IHs have been described with neurological symptoms, we suggest also considering treatment for asymptomatic patients with CNS IH in the early proliferative phase. Moreover, propranolol could be also useful prior to surgery in asymptomatic patients with sacral IH who require intervention for primary tethered cord with low-lying conus medullaris and high risk of bleeding, as in patient 3.
In our patients, propranolol was indicated either for aesthetic reasons or for functional risk. However, due to its characteristic to pass the blood-brain barrier (18), it has been effective and well-tolerated also for intra-CNS lesions. These data suggest that oral propranolol should be considered the first-line therapy for this rare/underestimated localization in order to avoid possible complications.
Our experience confirms that segmental cutaneous IHs on the head, neck, upper trunk and lumbar or sacral region should be investigated both for brain and spinal involvement.
Five of the authors of this publication are members of the Vascular Anomalies Working Group (VASCA WG) of the European Reference Network for Rare Multisystemic Vascular Diseases (VASCERN).


 Click to show fullsize
Click to show fullsize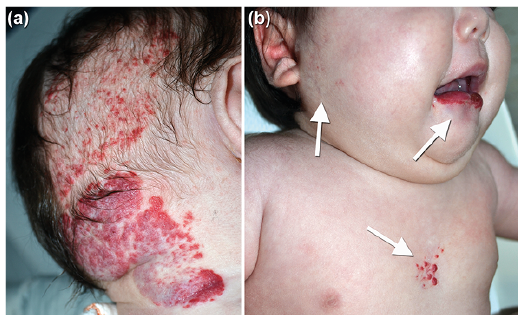 Click to show fullsize
Click to show fullsize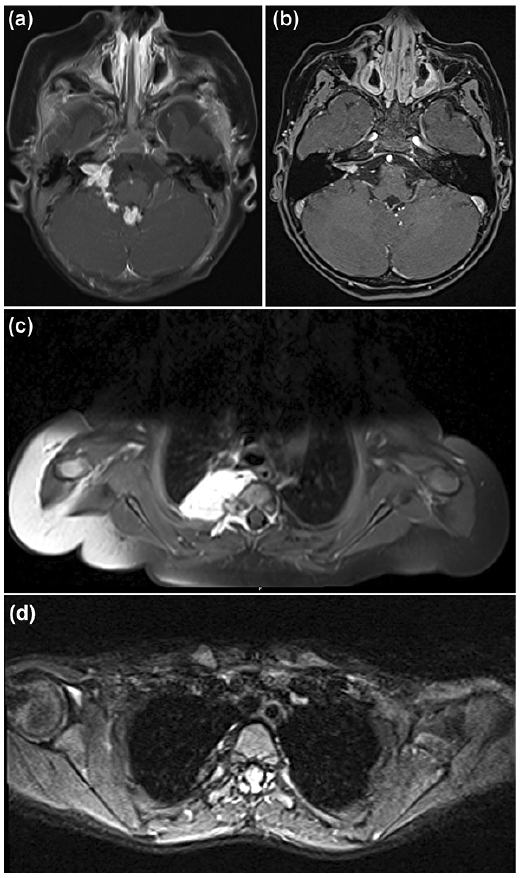 Click to show fullsize
Click to show fullsize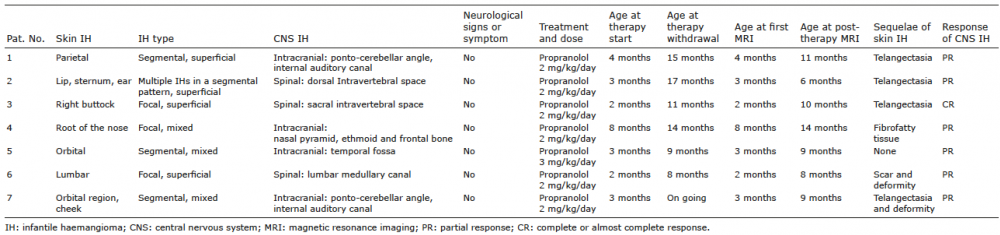 Click to show fullsize
Click to show fullsize