


Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, Tottori University, 86 Nishi-cho, Yonago-shi, Tottori 683-8503, Japan. E-mail: yxyhifu1@tottori-u.ac.jp
Accepted Sep 24, 2020; Epub ahead of print Sep 28, 2020
Acta Derm Venereol 2020; 100: adv00287.
doi: 10.2340/00015555-3650
We report here a case of multiple pedunculated poromas in a patient with rheumatoid arthritis treated with methotrexate.
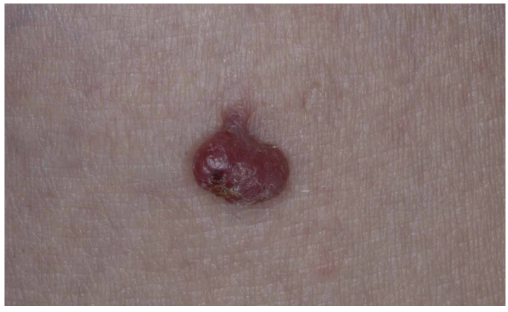
A 76-year-old Japanese woman was referred to our clinic for eval-uation of a 3-year history of multiple reddish nodules. She had a medical history of breast cancer 12 years previously. She had also been treated for 4 years with oral methotrexate (8 mg/week) for rheumatoid arthritis. Physical examination revealed multiple pedunculated nodules, approximately 4–5 mm in diameter, on both hands, face and trunk (4 nodules in total) (Fig. 1). The tumours were suspected to be pyogenic granulomas or skin tags, and were resected under local anaesthesia. Histopathologically, the entire tumour consisted of broad, anastomozing bands connected to the epidermis in a polypoid fashion (Fig. 2a). Tumour cells were composed of cuboidal poroid cells and eosinophilic cuticular cells. Small ductal structures were also seen (Fig. 2b). The tumour stroma was rich in vessels and eosinophilic hyalinized collagen (Fig. 2c). Based on these findings, a diagnosis of poromatosis in association with methotrexate treatment was made.
Fig. 1. A polypoidal nodule on the trunk.
Fig. 2. Histopathology of the tumour. (a) The tumour consisted of broad, anastomozing bands connected to the epidermis with a polypoid appearance (bar: 500 μm). (b) Tumour cells consisted of round-shaped poroid cells and eosinophilic cuticular cells. Small ductal structures were also seen (bar: 50 μm). (c) The stroma of the tumour was rich in vessels and eosinophilic hyalinized collagen (bar: 100 μm; H&E staining).
Poroma is a relatively common adnexal neoplasm that presents as a dome-shaped nodule in areas with abundant eccrine sweat glands. It occasionally occurs as multiple lesions, known as poromatosis. Although its pathogenesis remains to be elucidated, most cases of multiple poromas occur in patients who have received radiotherapy or cancer chemotherapy (1–15). An immunosuppressive condition might be involved in the development of multiple poromas. We reviewed previous reports on cases of multiple poromas related to medical treatment (Table I). Men accounted for 75% of patients. The tumours arose not only on the hands or feet, but also on the trunk and face. Eighteen (90%) of 20 cases had underlying neoplasms, especially haematological malignancies. Interest-ingly, the tumour in 13 cases (65%) had a polypoidal appearance. In addition, multiple polypoidal poromas developed in 4 cases, including the current case, and these were treated with methotrexate. Cases of multiple poromas after radiation therapy without chemotherapy were excluded from the review because the tumours in those cases developed only in the irradiated region and did not show a pedunculated appearance (not shown). The current patient had been treated with methotrexate for rheumatoid arthritis. Methotrexate is one of the chemotherapy agents (immunosuppressants) and is used for the treatment of many diseases. In addition to its well-known various adverse reactions, the drug may have a direct or indirect effect on the development of pedunculated poromas. Although we do not why drug-induced proroma shows exophytic growth, it is known that methotrexate occasionally causes acral erythema, suggesting excretion from sweat glands. An accumulation of methotrexate could be related to tumourigenesis. Since various chemotherapeutic agents were used for treat-ment in previously reported cases, other possible drugs could not be identified, except methotrexate. However, some chemotherapeutic agents are also concentrated in eccrine glands, which might cause multiple polypoidal poromas.
In conclusion, dermatologists must consider the possibility of drug involvement, especially methotrexate, in patients with multiple pedunculated poromas.
The authors have no conflicts of interest to declare.
Table I. Drug-induced multiple poromas


 Click to show fullsize
Click to show fullsize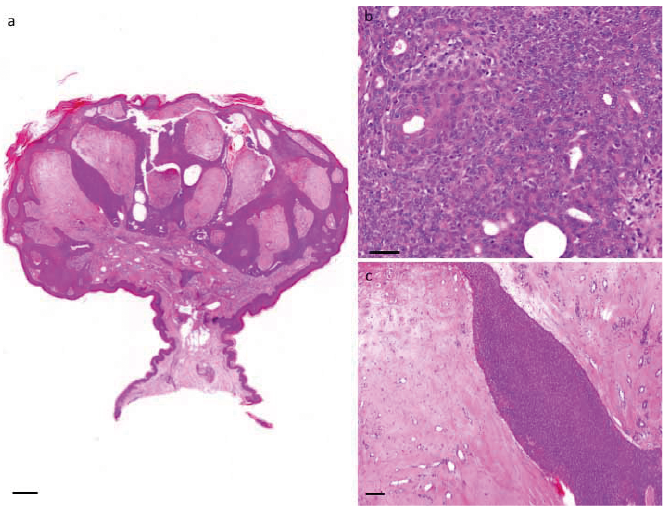 Click to show fullsize
Click to show fullsize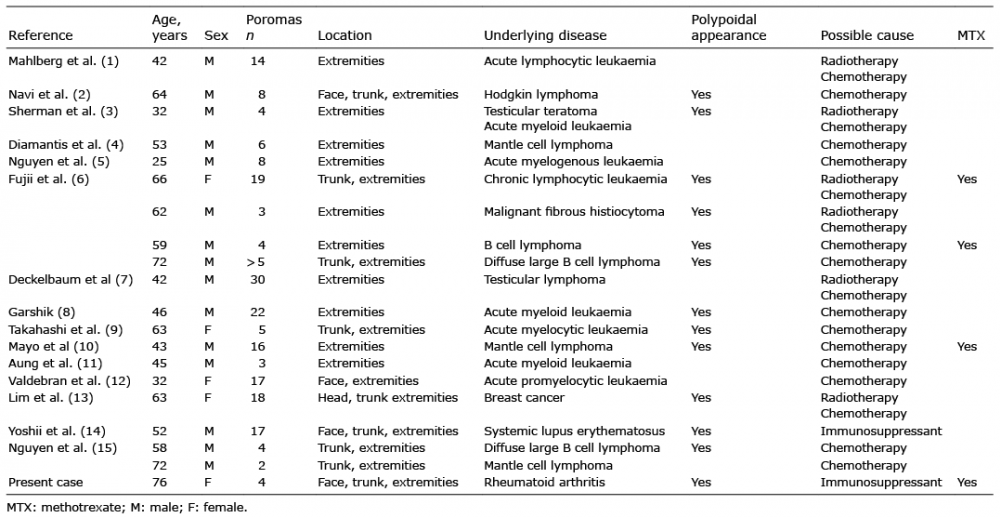 Click to show fullsize
Click to show fullsize