


1Department of Dermatology, The Faculty of Medicine, 2Faculty of Dental Sciences, Hadassah School of Dental Medicine, Hebrew University of Jerusalem, 3Tzameret, The Military Track of Medicine, The Hebrew University-Hadassah Medical School, 4The Faculty of Medicine, Hebrew University of Jerusalem, and 5Department of Clinical Microbiology and Infectious Diseases, Hadassah-Hebrew University Medical Center, Jerusalem, Israel
#These authors contributed equally.
Antibiotic-resistant Cutibacterium acnes has been reported worldwide, but data from Israeli patients with acne is currently lacking. This study evaluated the antibiotic susceptibility of C. acnes, isolated from 50 Israeli patients with acne to commonly prescribed antibiotics, using the Epsilometer test (E-test). Matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) analysis, 16S rRNA sequencing and single locus sequence typing (SLST) molecular typing were used to identify and characterize C. acnes. Among 36 strains isolated, phylotype IA1 was most common. Resistance to at least one antibiotic was found in 30.6% of tested strains. Resistance rates were highest for erythromycin (25.0%), followed by doxycycline (19.4%), clindamycin (16.7%), minocycline (11.1%) and tetracycline (8.3%). Significant correlation was found between resistance to multiple antibiotics, with 5.6% of isolates resistant to all antibiotics tested. When reviewing resistances rate worldwide antibiotic resistance was found to be prevalent in Israel. Measures to limit the emergence of antibiotic-resistant strains of Cutibacterium acnes should be taken and alternative treatments should be sought.
Key words: acne; Cutibacterium acnes; antibiotic; resistance.
Accepted Oct 2, 2020; Epub ahead of print Oct 6, 2020
Acta Derm Venereol 2020; 100: adv00295.
doi: 10.2340/00015555-3654
Corr: Sivan Sheffer-Levi, Kiryat Hadassah, Jerusalem, Israel. E-mail: sivan.sheffer@gmail.com
Cutibacterium acnes has a causative role in acne. Antibiotic resistance of Cutibacterium acnes has been reported worldwide, but there is no data regarding the antibiotic-resistance rates in Cutibacterium acnes in Israel. This study collected samples from 50 Israeli patients with acne and evaluated resistance rates for commonly prescribed antibiotics. Resistance to at least one antibiotic was found in 30.6% of isolated strains. Resistance rates were highest for erythromycin (25.0%), followed by clindamycin (16.7%) and doxycycline (19.4%), minocycline (11.1%) and tetracycline (8.3%). Antibiotic resistance was found to be prevalent in Israel. Measures to limit the emergence of antibiotic-resistant strains of Cutibacterium acnes should be taken and alternative treatments should be sought.
Acne is a common chronic inflammatory disorder of the pilosebaceous unit, affecting approximately 80% of adolescents and young adults (1). It is characterized by comedones, papules, pustules, nodules and cysts over pilosebaceous rich areas, such as the face, chest, upper back and arms. As sequelae, it may cause pigmentary changes, permanent scarring, and severe psychological implications, such as depression, social isolation and suicidal ideation. The pathophysiology of acne involves abnormal follicular keratinization, excessive sebum production (under androgen control), modification of the distribution of Cutibacterium acnes clusters and an inflammatory response (1, 2). Recent research emphasizes the role of dysseborrhoea (alteration of the sebaceous lipid profile), and involvement of external factors, such as stress, irritation, cosmetics and potential dietary factors, in inducing inflammation (3, 4). The role of the skin microbiome remains to be fully elucidated, but it is possible that changes in the distribution of species/strains, a stable distribution with pathogenic alteration in response to internal or external stimuli, or a combination of these factors, are involved in the pathogenesis of acne (5). A disturbed skin barrier and alteration of the skin microbiome results in the proliferation of C. acnes (4).
C. acnes, previously named Propionibacterium acnes, is a Gram-positive, preferential anaerobic rod, which is a dominant member of the microbiota of healthy human skin and an exclusive bacterial inhabitant of normal human facial sebaceous follicles (5). The anaerobic and lipid-rich conditions within the pilosebaceous unit provide an optimal microenvironment for the growth of C. acnes. Recent research has further elucidated the important role of C. acnes in the pathogenesis of acne. It has been shown to induce inflammatory responses in host skin parenchymal cells and immune cells through the activation of Toll-like receptors and the presence of host tissue-degrading enzymes (6) and is therefore considered an important target in the treatment of acne.
Developments in genomic research have shown that C. acnes consists of phylogenetically distinct cluster groups with different pathogenic traits. Some strains of C. acnes induce stronger cytokine/chemokine expression, as well as differentiation and proliferation of keratinocytes and sebocytes (7). These findings suggest that C. acnes strains may influence the severity of inflammatory acne. Exact identification of the pathogenic strains of C. acnes could lead to more selective and advanced therapeutics, aimed at these strains only.
Topical and oral antibiotics have been the mainstay of acne treatment for the past 40 years. Chronic course and prolonged therapy have contributed to the emergence of antibiotic-resistant C. acnes strains. Increases in antibiotic- resistant C. acnes have now been reported worldwide; however, data for different antibiotics and various regions or countries is incomplete. Many countries have reported that over 50% of strains of C. acnes are resistant, particularly to topical macrolides, and a correlation has been shown between the emergence of resistant C. acnes strains and antibiotic use. Collateral damage to the microbiome’s steady state and the emergence of antibiotic resistance in non-target bacteria is also a major concern (8). With progression into the “post-antibiotic era”, clinical guidelines for the treatment of acne, published by the international group “The Global Alliance to Improve Outcomes in Acne” in 2018, have excluded antibiotic agents as monotherapy (topically and systemically) in order to prevent further development of resistant strains (9). Development of new treatment modalities for acne is necessary and, regardless of acne, the need for novel antimicrobial agents is urgent.
To date, information regarding antibiotic resistance rates of C. acnes in Israeli patients with acne is lacking. The data provided here may contribute to raising the awareness of anti-microbial resistance and changing the way dermatologists use antibiotic agents to treat acne.
The aim of this study was to characterize the antibiotic susceptibility patterns of C. acnes isolated from Israeli patients with acne.
Patients
Patients, over 10 years of age, with acne vulgaris attending the Dermatology Clinic at Hadassah Hebrew University Medical Center, were invited to participate in the study. Written informed consent was obtained from the participants and/or their parents after providing a detailed explanation of the study. Clinical information, including age, sex, age of onset, previous or current anti-acne treatments, acne severity (according to the Physician Global Assessment) (10) and acne distribution, were obtained from medical records. The study was approved by the local ethics review board (HMO-0073-19).
Specimen collection and processing
The skin over acne lesions was first cleaned with 70% isopropyl alcohol wipes. Comedonal or pustular content was squeezed manually or punctured with a sterile needle. The content was collected on a sterile swab (Copan ESwab®, Murrieta, CA, USA) and inoculated into the surface of culture plates containing Wilkins-Chalgren agar (Oxoid, Hampshire, England) supplemented with furazolidone to inhibit the growth of staphylococci. The plates were incubated under anaerobic conditions (anaerobic chamber or anaerobic bags) between 48 h to one week, and examined daily for the appearance of typical colonies. If the culture was negative after one week, another culture was prepared from the original bacterial swab that was kept refrigerated. Isolation streaks were performed to obtain single colonies. Each isolated strain was viewed microscopically. To confirm that these bacteria were C. acnes, matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) analysis was performed (11). For strains unrecognized by MALDI-TOF, 16S PCR and sequencing were performed using Ilumina’s universal 16S primers (https://support.illumina.com/documents/documentation/chemistry_documentation/16s/16s- metagenomic-library-prep-guide-15044223-b.pdf) (12). Sequences were compared with a database using BLAST software (https://blast.ncbi.nlm.nih.gov/Blast.cgi). All confirmed C. acnes strains had undergone a PCR reaction with the single locus sequence typing (SLST) method primers, described herein, and were recognized by these specific primers. Furthermore, when the PCR product was sequenced and compared to the BLAST database, it matched C. acnes in 99% similarity.
Single locus sequence typing
Molecular characterization of C. acnes was performed using SLST, as described by Scholz et al. (13). This rapid method uses a single locus in the C. acnes genome to classify the strain and to distinguish between the defined C. acnes phylotypes. The following primers were used for SLST: forward primer 5’-CAGCGGCGCTGCTAAGAACTT-3’; reverse primer 5’-CCGGCTGGCAAATGAGGCAT-3’. The PCR product was sequenced and compared with different known SLST types (http://medbac.dk/slst). Discrimination between the different phylogenetic clusters of C. acnes, and adaptation to the phylotypes described in the traditional typing method, was performed using the scheme provided by Scholz et al. (13).
Antibiotic susceptibility
Following bacterial identification, C. acnes isolates were sub-cultured in Wilkins broth (Oxoid, Basingstoke, UK) and suspended at a density of 1.0 McFarland. Bacterial lawns were prepared on anaerobic blood plates (Novamed, Jerusalem, Israel) and allowed to dry. Antibiotic susceptibility was assessed by determining a minimal inhibitory concentration (MIC) using an Epsilometer test (E-test) (ETEST® bioMérieux, St. Louis, MO, USA). The MIC was determined at 48 h following incubation under anaerobic conditions as the point on the scale at which the ellipse of growth inhibition intercepts the plastic strip. The antibiotics used were: erythromycin, clindamycin, tetracycline, doxycycline and minocycline. The breakpoints used to define susceptibility or resistance to clindamycin and tetracycline followed the recommendations set out by the Clinical and Laboratory Standards Institute (CLSI) (14); resistance to clindamycin was defined at a MIC above 2 µg/ml and tetracycline at a MIC above 4 µg/ml. Since no standards exist for breakpoints of erythromycin, doxycycline and minocycline, those with a MIC of ≥ 0.5 µg/ml (for erythromycin) and ≥ 1 µg/ml (for doxycycline and minocycline) were defined as resistant, according to definitions used in previous studies (15).
Antibiotic susceptibility patterns in relation to characteristics of patients and acne
The antibiotic susceptibility patterns of C. acnes to the different antibiotics were compared between the patients; sub-grouped according to sex, age (> 20 years and 20 years or less), acne duration (< 2 years and 2 years or more), acne severity (mild, moderate and severe, according to Physician’s Global Assessment) (10) and acne distribution (facial only and face plus trunk). The patients were also sub-grouped according to negative or positive history of previous therapy and previous antibiotic therapy for acne. The resistance patterns to multiple antibiotics were examined as well as the correlation with different phylotypes.
Statistical analysis
Data were analysed using IBM SPSS Statistics V22.0 (https://www.ibm.com/analytics/spss-statistics-software). Descriptive statistics were used to display the research results. Sequential variances (age, acne duration) were compared using Student’s t-test. Categorical variances were compared by χ2 test. A p-value of ≤ 0.05 was considered statistically significant.
Patients’ characteristics
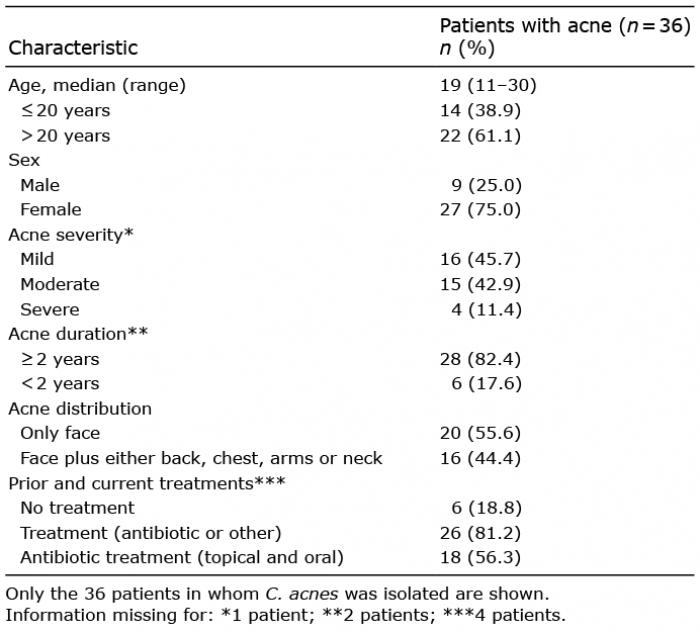
Patients’ demographic and clinical characteristics are shown in Table I. Only the 36 patients in whom C. acnes was isolated are presented. Only a minority of the patients had severe acne. Among treatments for acne, antibiotic treatment was administered in 18 patients and included topical clindamycin, erythromycin, neomycin, oral minocycline and doxycycline. Other therapies for acne included topical benzoyl peroxide, topical retinoids, isotretinoin and oral contraceptive pills.
Table I. Patient’s demographic and clinical characteristics
Identification of Cutibacterium acnes strains
Throughout the 6-month study period from December 2017 to May 2018, comedonal or pustular content samples were obtained from 50 patients with acne vulgaris (Table SI). Bacteria were isolated from 44 samples on plates and in liquid culture. Twenty-six of the isolates were identified as C. acnes using MALDI-TOF (Table SI). The 10 isolates that were not identified were sent to 16S rRNA sequencing (Table SI). These analyses showed that C. acnes strains were present in 36 patients (isolation rate 72%). The other isolates were Cutibacterium avidum (7 strains; 6 isolated from facial skin and 1 isolated from the back) and Cutibacterium granulosum (1 strain isolated from facial skin) (Table SI).
Phylotype identification
The SLST typing of the strains was tested further using the medbac website (http://medbac.dk/slst/pacnes). The data are presented in Fig. 1. Seventeen strains were of the A1 SLST type, and the remainder were C1 (4 strains), C2 (1 strain), D1 (2 strains), F4 (3 strains), H1 (2 strains) and K1 (1 strain). Six strains were recognized by the SLST method, but the sequence did not match any currently recognized strain. Since they seem to represent new SLST types the sequencing process was repeated for a second confirmation, and the data were sent to the medbac website to be added to the database. Their sequences were confirmed as C. acnes in the BLAST database, in 97.54% similarity (Appendix S1), with another independent C. acnes identification described herein (Table SI). Conversion of the SLST types to the phylotypes according to traditional typing is shown in Fig. 1 (13).
Fig. 1. Cutibacterium acnes molecular typing in the 36 clinical isolates. (A) Single locus sequence typing. (B) Phylotypes (traditional typing).
Antibiotic susceptibility assay in Israeli patients with acne
The isolates and their resistance profiles, with the number of strains inhibited at various MICs, are shown in Table II. The MIC ranges in the current study were 0.016–256 µg/ml for erythromycin, 0.016–256 µg/ml for clindamycin, 0.047–256 µg/ml for tetracycline, 0.047–64 µg/ml for doxycycline and 0.023–32 µg/ml for minocycline. MIC50, the MIC required to inhibit the growth of 50% of bacteria, of the 36 strains were all below the resistance breakpoint of all antibiotics tested. MIC50 was lowest for erythromycin (≤ 0.016 µg/ml) and highest for tetracycline and doxycycline (0.190 µg/ml). MIC90, the MIC required to inhibit the growth of 90% of bacteria, were all above the resistance breakpoint of the antibiotics tested and showed the highest value for erythromycin (≥ 256 µg/ml) and lowest value for minocycline (1 µg/ml).
Table II. The isolates examined and their resistance profiles, with the number of strains inhibited at various minimum inhibitory concentrations (MICs)
All resistant isolates (with resistance to at least one of the antibiotics tested) are shown in Table III. Overall, resistance to at least one antibiotic was found in 30.6% of the isolated strains. The antibiotic that showed the highest percentage of resistant strains was erythromycin, with 25.0% resistant strains, followed by doxycycline (19.4%), clindamycin (16.7%), minocycline (11.1%) and tetracycline (8.3%) (Fig. 2).
Table III. Antibiotic resistance pattern of resistant isolates (with resistance to at least one of the antibiotics examined)
Fig. 2. Percentage of Cutibacterium acnes resistant strains among the 36 clinical isolates. Resistant breakpoints: clindamycin > 2 µg/ml; erythromycin ≥ 0.5 µg/ml, doxycycline and minocycline ≥ 1 µg/ml; tetracycline > 4 µg/ml. Antibiotics: EM; erythromycin; CM: clindamycin; TET: tetracycline; DOX: doxycycline; MC: minocycline.
Minimal inhibitory concentration differences regarding patients’ characteristics
No statistically significant differences were found between MIC and age, sex, acne characteristics (severity, distribution and duration), previous or current treatments, or between phylotypes.
Antibiotic susceptibility patterns
The antibiotic resistance profiles of the 11 resistant strains are shown in Table III. In most cases, resistance to one or more antibiotics showed a trend towards a higher MIC for the remaining antibiotic/s even though the MIC did not exceed the resistance breakpoint. Six (16.7%) strains had cross-resistance among MLS (macrolides–lincosamides–streptogramins), namely, clindamycin and erythromycin. Seven (19.4%) had cross-resistance between the MLS and cycline antibiotics, and 3 (8.3%) strains had cross-resistance among cycline antibiotics. Interestingly, different susceptibility patterns were seen within the same family of tetracycline. Statistically significant correlations were found between resistance to all pairs of antibiotics tested, except for minocycline and doxycycline (p = 0.302); erythromycin and minocycline (p = 0.01431); clindamycin and erythromycin, doxycycline or tetracycline (p = 0.00001), clindamycin and minocycline (p = 0.028), erythromycin and doxycycline (p = 0.00001), erythromycin and tetracycline ((p = 0.0027), minocycline and tetracycline (p = 0.0001) and doxycycline and tetracycline (p = 0.014).
Antibiotics have been a mainstay of acne treatment for many years. The antibiotic treatment is administered for its antibacterial effect, addressing C. acnes colonization, but also for its anti-inflammatory and immunomodulatory properties (16). Widely used topical antibiotics for acne in Israel include clindamycin 1% gel and erythromycin 2% solution or emulsion. Systemic antibiotics, such as minocycline and doxycycline, are indicated for moderate-to-severe inflammatory acne or after a failure of topical therapy. A typical treatment course may last several months and the selective pressure from long-term use is considerable. As previously mentioned, antibiotic-resistance of C. acnes has been reported worldwide (15, 17-34), but antibiotic susceptibility patterns of C. acnes in Israeli patients with acne, to the best of our knowledge, have not been determined. This is the first report to address C. acnes antibiotic resistance rates in Israel.
The isolation rate of C. acnes from 50 patients with acne in this study was only 72%. Isolation rate of C. acnes in previous studies was shown to be between 57% (32) and 96% (31), but mostly around 80% (15, 17). If other Cutibacterium are included, the isolation rate in the current study increases to 88%. Accurate methods to identify C. acnes, as used in this study, may contribute to this relatively low isolation rate.
C. acnes recognition was performed initially with MALDI-TOF. The bacteria that were not recognized by this method were then sent to 16S rRNA sequencing, which recognized all the bacteria as either C. acnes or as a different Cutibacterium species. All C. acnes isolates were then phylotyped using the SLST method.
Previous studies have shown that different C. acnes phylogroup strains have a different effect on the innate immune response and pathogenic potential in inducing acne lesions (7). Phylotype 1A1 is considered an acne-associated type. Although specimens were not collected from healthy controls or healthy skin to analyse the skin microbiome in comparison with acne lesions in the current study, the phylotype distribution, consisting mainly of the 1A1 phylotype, is in correlation with previous studies (7). Other phylotypes found in our study (IA2, IB, II) have also been recovered from acneic skin, but their rates of recovery are low, again, in accordance with the current findings. The focus of future in vitro work should be on the 1A1 phylotype, as it appears to be the major pathogen related to acne.
This study used the E-test to assess the antibiotic susceptibility of 5 antibiotics used widely to treat acne in Israel. Methods used to assess the antibiotic resistance of C. acnes in previous reports, included the conventional agar dilution method (27, 30, 31, 35–38), E-test (15, 19, 24, 33, 34, 39) and disk diffusion assay (17). When using the E-test method to assess antibiotic susceptibility, there are no definite standards in breakpoints of antibiotic resistance. The same MIC interpretation criteria used for the agar dilution method were used in the current study, as previous reports have shown a high degree of agreement between these 2 methods (17).
Table II shows the different phenotypes, with various MIC values indicating low or high levels of resistance. It is possible that the different phenotypes correlate with different mutations and resistance mechanism. Molecular analysis of the resistance mechanisms is needed for further investigation.
Data on the percentages of resistant C. acnes from different countries worldwide show a wide variation, as seen in Table IV and Fig. 3. The data shown here are taken from the latest publication from each country. Regional differences are remarkable and dynamic changes are also observed over time. The prevalence of carriage of resistant isolates was reported to be as high as 94% in Spain and the UK (30, 40), and 98% in India (41). In other countries, such as Korea, Japan, Chile and Australia, the reported incidence of resistance was much lower, but still demonstrated a trend towards higher MIC values over time (15, 37, 39, 42). A study from the UK showed an increase in antibiotic-resistant C. acnes strains, from 34% in 1991 to 64% in 1997 (40). A recent review describes a gradual increase in C. acnes antibiotic resistance; from 20–25% in the 1970s–1980, to 50–60% in the 1990s, reaching a peak at 75% in the early 2000 and decreasing to 30–40% within the past decade (43).
Table IV. Reported resistance rates of Cutibacterium acnes from different countries worldwide
Fig. 3. Resistance rates of Cutibacterium acnes reported from different countries worldwide.
The reason for the difference in the in vitro antibiotic susceptibility patterns of C. acnes among different countries is not clear. It may be attributed to the different antibiotic prescribing habits, different drug availability, but also different patients’ ethnicities and different C. acnes phylogenetic strains. The lack of implementation of international treatment guidelines probably contributes to the difference in antibiotic susceptibility patterns. Also, when evaluating and comparing resistance rates, many variables should be taken into consideration, including study setting, demographic background, sampling site, sampling technique, type and severity of acne, pre-treatment and definition of antibiotic resistance (43).
Resistance to erythromycin in the patients in the current study showed an “all or none” pattern (Fig. 4) with susceptible bacterial strains being highly sensitive (MIC ≤0.0.64 µg/ml) or highly resistant (MIC ≥256 µg/ml). This ?nding is in accordance with previous studies and is probably explained by the resistance mechanism determined by mutations in the 23S RNA gene or acquired ermX transposon (28). This suggests that erythromycin might still be effective in the group of patients with the non-mutated C. acnes and that does not possess the erm(X) gene.
Fig. 4. Resistant vs highly resistant isolates. R high: minimal inhibitory concentration (MIC) ≥ 256 µg/ml. R: breakpoint≤MIC< 256 µg/ml. Antibiotics: EM: erythromycin; CM: clindamycin; TET: tetracycline; DOX: doxycycline; MC: minocycline.
The lack of statistically significant differences in MIC in regard to the characteristics of patients or acne in our study, is probably due to the small sample size. Other studies have shown a correlation between the emergence of resistant C. acnes strains and antibiotic use (15, 18, 20–23), acne severity (20–21, 24), sex (24), age (25), disease duration (25), clinical unresponsiveness and acne relapses (26).
The high degree of cross-resistance between erythromycin and clindamycin found in the current study is in agreement with previous studies (18, 27–28). An association between resistance to tetracycline, doxycycline and minocycline was also reported (29). As in the current study, cross-resistance between the MLS and cycline antibiotics has been described in a study from Hong Kong (25). Clinical implications may suggest lack of response of acne to other antibiotic treatments in a patient who did not respond to one antibiotic treatment.
The main limitation of the current study was the small sample size. In addition, the patients attending the dermatology outpatient clinic in our centre may not represent the general population, as most patients with acne are managed in community-based dermatology clinics. Another important issue is the lack of standardization in resistance cut-off points for C. acnes. Altering the cut-off points may have a significant impact on our results. Discrepancies between resistance breakpoints and methods to assess antibiotic susceptibility indicate the need for a standardized susceptibility test method for C. acnes. Taking all these limitations into consideration, we have still shown that antibiotic resistance of C. acnes in Israel is prevalent and should be taken into consideration when prescribing antibiotic treatment for acne. Other limitation is that there is no control healthy group.
In conclusion, antibiotic resistance of C. acnes represents a major concern in Israel, as it does worldwide. Further studies are recommended to assess the in vitro antibiotic resistance and variables affecting the resistance rate in a larger group of patients with acne. Measures to limit the emergence of resistant strains of C. acnes, such as limiting the use of antibiotics, should be taken, and new alternative treatments should be sought.
Funding sources. Gishur Fund of Hadassah Medical Center, George and Linda Hiltzick’s donation to Hadassah Medical Center.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize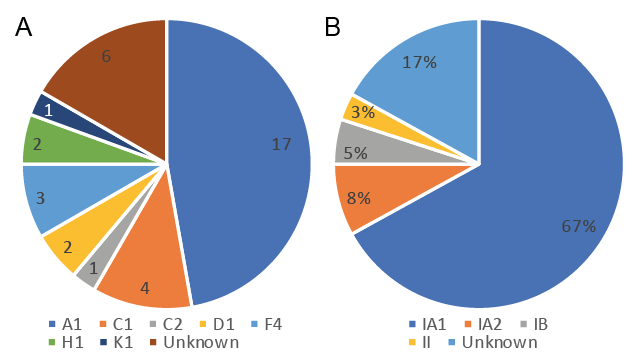 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize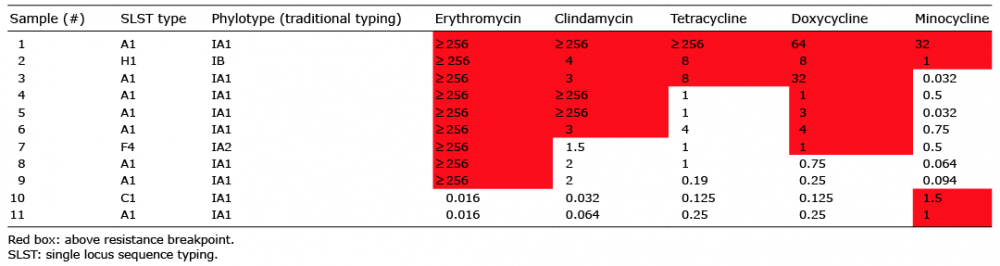 Click to show fullsize
Click to show fullsize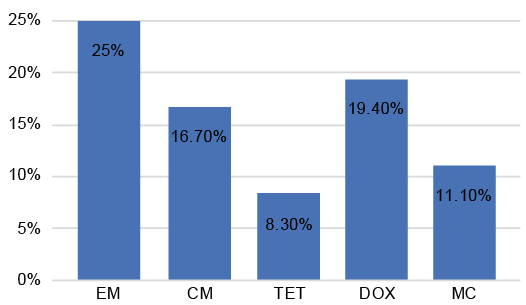 Click to show fullsize
Click to show fullsize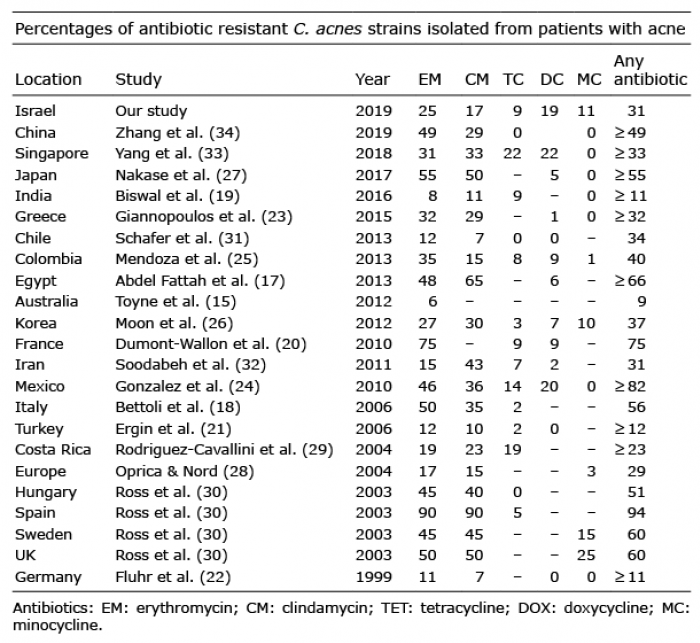 Click to show fullsize
Click to show fullsize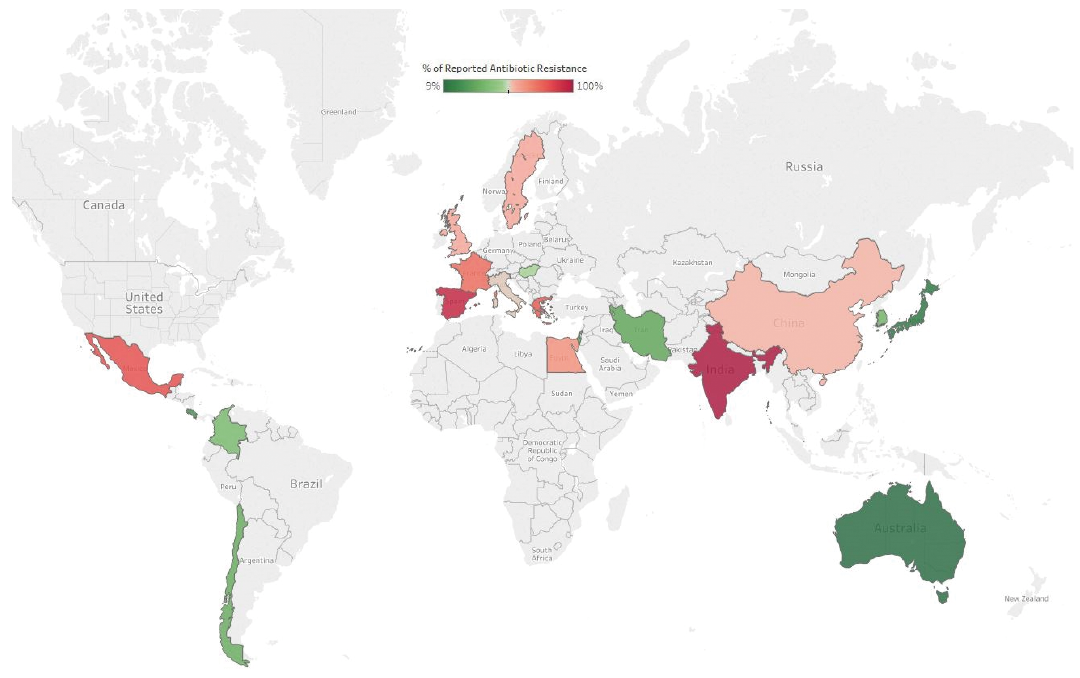 Click to show fullsize
Click to show fullsize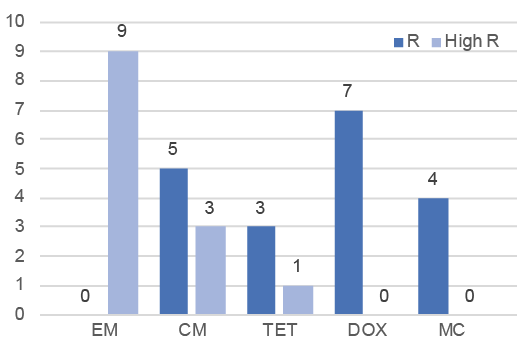 Click to show fullsize
Click to show fullsize