


1Department of Skin and Venereal Diseases, Medical Academy, Lithuanian University of Health Sciences, Eiveniu St. 2, LT-50161 Kaunas, Lithuania and 2Department of Dermatology & Venereology Otto-von-Guericke University Magdeburg, Germany. E-mail: k.tvaronaviciute@gmail.com
Accepted Oct 15, 2020; Epub ahead of print Oct 19, 2020
Acta Derm Venereol 2020; 100: adv00311.
doi: 10.2340/00015555-3672
SAPHO (synovitis-acne-pustulosis-hyperostosis-osteitis) syndrome is a rare inflammatory condition that has no validated diagnostic criteria among other seronegative spondyloarthropathies (1). The main symptoms are hyperostosis (of the anterior chest wall (ACW), vertebral) and/or chronic recurrent multifocal non-infectious osteomyelitis involving the axial or peripheral skeleton (2, 3). Cutaneous manifestations in patients with SAPHO syndrome include palmoplantar pustulosis (PPP), severe forms of acne, and various forms of psoriasis, especially pustular psoriasis (4). In SAPHO syndrome, acne can present as acne conglobate, acne fulminans, hidradenitis suppurativa (HS), or HS combined with pyoderma gangrenosum (PG) (5, 6). Furthermore, depressive disorders and new evidence of underreported schizophrenia in these disease constellations must be considered. This case report summarizes a successful clinical outcome with biologic therapy in a patient with HS plus conglobate acne associated with SAPHO syndrome.
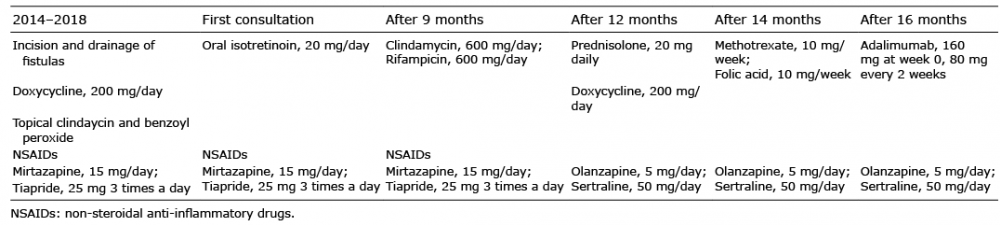
An 18-year-old male (body mass index 15.74 kg/m2) with a history of depression and conglobate acne since 14 years of age presented to the Department of Skin and Venereal Diseases, Hospital of Lithuanian University of Health Sciences Kaunas Clinics, Kaunas, Lithuania in September 2018. From 14 years of age, the patient had attended the surgery department for over 20 episodes of incision and drainage of painful fistulas on the neck, which were treated with oral doxycycline, 200 mg/day, together with a combination of topical clindamycin and benzoyl peroxide (Table I) Non-steroidal anti-inflammatory drugs (NSAIDs) were used throughout the treatment period. His depression was treated with psychotherapy and mirtazapine, 15 mg/day, and tiapride, 25 mg 3 times a day. At the first consultation, a low dose of oral isotretinoin, 20 mg/day, was prescribed and, after 5 months, due to worsening of his acne and depression, the patient decided to discontinue the treatment. The patient presented to our outpatient clinic, then the skin lesions worsened. Clinical examination revealed lesions on his neck, back and right armpit (Fig. 1). Based on clinical findings, a diagnosis of hidradenitis suppurativa (HS), Hurley II, Physician Global Assessment (PGA) score 3 was diagnosed and, primarily directed at treatment of HS, treatment with clindamycin, 600 mg/day, and rifampicin, 600 mg/day was initiated. On admission, the patient’s quality of life (QoL) was substantially impaired, Dermatology Life Quality Index (DLQI) score 20 points. Unfortunately, after 2 months of therapy, no improvement in cutaneous symptoms was seen. The patient began to report severe migratory pain of the chest bones (visual analogue scale; VAS 9). Laboratory tests revealed an erythrocyte sedimentation rate (ESR) of 13.2 mm/h (reference range 0–7 mm/h), leukocyte count (10.2×109/l; reference range 3.9–8.8×109/l) with elevated neutrophils (73.5%; reference range 41–71%). Serological tests for hepatitis B and C, QuantiFERON-TB Gold, and HLA-B27 were negative. Due to severe chest pain, whole-body bone scintigraphy using technetium-99m labelled with methylene diphosphonate was performed, which showed an intense uptake of the contrast agent at the sternoclavicular and sacroiliac joints. Computed tomography (CT) scan of the thoracic bones revealed small osteolytic lesions in the sternum and hyperostosis of the first ribs and sternocostal junctions. Based on the clinical presentation and radiographic findings, a diagnosis of SAPHO syndrome in association with HS plus conglobate acne was made. In addition, the patient was examined by psychiatrists, and the diagnosis of depression was changed to simple schizophrenia. Treatment with mirtazapine and tiapride was then switched to olanzapine, 5 mg/day, and sertraline, 50 mg/day. To improve severe sternal pain and reduce skin inflammation, the patient was treated with prednisolone, 20 mg daily, and doxycycline, 200 mg daily. A temporary clinical effect was achieved, but this treatment was stopped due to gastrointestinal symptoms after 2 months. As a result, subcutaneous injections of methotrexate (MTX), 10 mg/week, and folic acid, 10 mg/week, were started. After 9 injections of MTX, the patient experienced a substantial improvement in chest pain. However, no improvements were observed in his cutaneous symptoms. Furthermore, elevated liver enzymes were observed: ALT 130 IU/l (reference range 0–45 IU/l); AST 52 IU/l (reference range 0–35 IU/l). Therefore, anti-TNF-α monotherapy with adalimumab with an induction dose of 160 mg and a maintenance dose of 80 mg every 2 weeks was started. After 6–12 weeks of this regimen, a clinical response of cutaneous symptoms of both HS and conglobate acne was observed, with decreased pain in the inflammatory nodules, resolution of the associated pustular discharge, and no development of new lesions (Fig. 2). The chest pain disappeared (VAS score 0), erythrocyte sedimentation rate, leukocyte count and liver enzymes returned to normal ranges. Moreover, after 12 weeks of treatment, an improvement in the patient’s QoL was shown in activities of daily living, work and leisure, and the DLQI score decreased to 3 points.
Table I. Sequence of treatment
Fig. 1. Clinical presentation prior to initiation of therapy. (A) Chronic inflammatory nodules, papules, comedones, and scars on the upper neck. (B) Active fistulas and scars on the lateral neck region. (C) Nodules, cysts, and scars in the right armpit.
Fig. 2. Clinical presentation after 6–12 weeks of therapy. (A) A decrease in inflammatory papules, comedones, and cysts on the back. (B) No active fistulas on the lateral neck region. (C) No nodules, cysts, or scars in the right armpit.
This case demonstrates sustained clinical and biological improvement with adalimumab therapy. However, the pathogenesis of SAPHO syndrome remains poorly understood. Inflammatory pathways involving proinflammatory cytokines tumour necrosis (TNF)-α, interleukin (IL)-1, IL-17 and genetic susceptibilities are major triggers for both SAPHO and HS (7). TNF-α is an important pro-in?ammatory cytokine, involved in many in?ammatory processes. Blocking TNF-α may therefore improve SAPHO syndrome and HS (8). Adalimumab is the only agent approved for use in HS. In the current case, TNF-α inhibitors were efficient in treating the cutaneous HS, conglobate acne manifestations and SAPHO joint symptoms.
In conclusion, the association of SAPHO syndrome with HS and conglobate acne is rare. The QoL of patients affected by both SAPHO and HS may be highly compromised and coexistence of these diseases may represent a therapeutic challenge. Matusiak et al. (9) reported a study that evaluated pruritus and pain among 103 patients with HS. They found that the most troublesome symptom of HS was pain, followed by exudation, pruritus, appearance and smell, consecutively. Pruritus of mild-to-moderate intensity is a common HS-associated symptom that adversely affects patients’ QoL (9). Patients with HS, severe acne, and bone pain should be screened carefully for spondyloarthritis and SAPHO syndrome. An in-depth case history of mental disorders is recommended. It should be noted that the current patient was treated with olanzapine and sertraline which stabilized the mental state.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize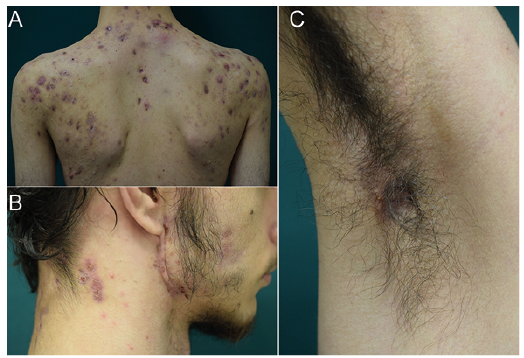 Click to show fullsize
Click to show fullsize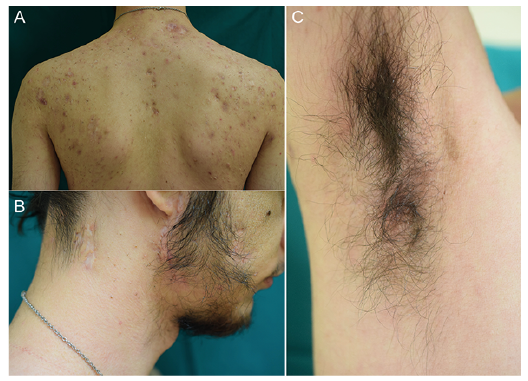 Click to show fullsize
Click to show fullsize