


Department of Dermatology, University Hospital of Oulu, and Medical Research Center, PEDEGO Research Group, University of Oulu, FIN-90220 Oulu, Finland. *E-mail: kaisa.tasanen@oulu.fi
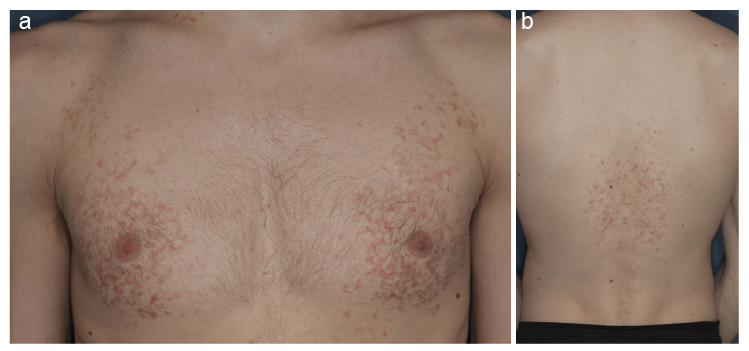
A 24-year-old, otherwise healthy, Caucasian male was referred to the Department of Dermatology with pruritic rash, which had appeared gradually over the previous year. Physical examination revealed a reticular, hyperpigmented, slightly scaly rash and erythematous papules on his chest, back and sides (Fig. 1). There was no mucous membrane involvement and no enlarged lymph nodes were found. The patient had tried to treat his skin symptoms with both moderate and potent topical corticosteroid creams, but without response. A punch biopsy of a skin lesion showed orthokeratosis in the epidermis, which was slightly spongiotic, and a few apoptotic keratinocytes. Melanin pigment was seen in the upper dermis.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical photographs. (a) Symmetrically distributed erythematous papules and reticulated pattern on the chest and (b) on the back.
Acta Derm Venereol 2020; 100: adv00321.
Diagnosis: Prurigo pigmentosa and new-onset type 1 diabetes
The reticulate network-like pattern of papules on the patient’s chest raised suspicion of prurigo pigmentosa (PP). The patient’s total blood cell count, erythrocyte sedimentation rate, level of C-reactive protein, fasting plasma glucose (FPG), glycated haemoglobin fraction (HbA1c) and urine test results were taken. In laboratory tests the FPG was 22.2 mmol/l (reference 4.2–6.0 mmol/l) and HbA1c 127 mmol/mol (reference 20–42 mmol/mol). The urine strip-test revealed the presence of ketones and glucose. Afterwards, more detailed anamnesis revealed that the patient had noticed unintentional weight loss, thirst and more frequent urination. These being signs of possible type I diabetes, the patient was referred to the emergency department of internal medicine, where the diagnosis was confirmed and he was hospitalized and then prescribed insulin glargine treatment. The PP lesions started to fade a few weeks after initiation of treatment for type 1 diabetes.
PP is a rare inflammatory skin condition that affects people of all ages, sex and ethnicities. However, it may be twice as common in women as in men and frequently occurs in the second or third decade of life. Most published case reports describe young Japanese women. The preponderance of Japanese patients is thought to come from better awareness of the disease in Japan rather than from ethnic factors (1, 2).
The clinical picture of PP is representative. The condition typically manifests as symmetrically distributed inflamed red raised papules that coalesce to form a reticulate (network-like) pattern, most commonly seen on the upper back, chest, neck and abdomen. Disease progression follows 3 stages, which develop in 2–3 days: early-stage lesions are erythematous macules and urticaria-like itchy papules with sudden onset. Once these are resolved, they are followed by crusted erythematous papules (fully developed lesions). Lastly, the lesions heal with reticulated post-inflammatory hyperpigmentation (late-stage lesions), which can take months to disappear. Recurrences are distinctive and can occur at varying intervals (weeks or years). The clinical picture may also show signs of scratching. Histological examination of early-stage lesions may show superficial perivascular neutrophilic infiltrate and necrotic keratinocytes. The fully-developed stages are characterized by lymphocytic infiltrate and necrosis of keratinocytes. Scale-crust and melanophages can be seen in late-stage lesions (1–4).
The aetiology of PP is unknown. Nevertheless, it has been suggested that it may be associated with ketotic states, fasting and dieting, diabetes mellitus, anorexia nervosa and bariatric surgery. There are many patients with PP who have high levels of ketones in the blood or urine. It has been proposed that ketone bodies cluster around blood vessels causing neutrophilic inflammation. However, not every PP patient is ketotic, and, thus, other factors may also contribute to progression of the disease. Contact allergies, mechanical stimulation and sweating/climate have also been proposed as risk factors (1, 2, 5).
When no evident cause of PP is found, the first-line treatment is tetracyclines, the anti-inflammatory effects of which inhibit neutrophil function. Dapsone and macrolide antibiotics can also be considered as first-line options. Corticosteroids have no effect on PP, as was seen in the current patient (1, 2).
PP may be underdiagnosed in Western countries. In the current case, the recognition of PP led to investigation of the patient’s glucose parameters and facilitated the diagnosis of previously undetected type I diabetes in this young man. It is important to remember that dermatologists may occasionally be the first healthcare professionals to detect signs of a serious and, even potentially life-threatening, condition.


 Click to show fullsize
Click to show fullsize