


1Department of Dermatology, University Hospital Henri Mondor, Créteil, 2Keyrus Life Science, Levallois-Perret and 3Pierre Fabre SA, Boulogne-Billancourt, France
A systematic literature review was conducted to identify and qualitatively assess randomized controlled trials in immunocompetent patients ≥ 18 years with head- region lesions of actinic keratoses who were treated with field-directed, lesion-directed and other therapies. Network meta-analysis was used to quantitatively evaluate field-directed therapies (5-fluorouracil formulations, diclofenac sodium, imiquimod, ingenol mebutate, 5-aminolevulinic acid or methyl aminolevulinate plus photodynamic therapy) using complete clearance or partial clearance of actinic keratoses lesions, and adverse event-related withdrawals as a proxy of acceptability. Of 2,863 references identified, 75 trials reported in 151 publications were included. In summary, comparative network meta-analysis evaluation showed that 5-fluorouracil formulations were the most efficacious interventions examined. 5-fluorouracil 4%, which was recently approved, showed a comparable efficacy profile to 5-fluorouracil 5%, and had satisfactory acceptability outcomes.
Key words: actinic keratosis; systematic literature review; network meta-analysis; field-directed intervention.
Accepted Nov 5, 2020; Epub ahead of print Nov 10, 2020
Acta Derm Venereol 2021; 101: adv00358.
doi: 10.2340/00015555-3690
Corr: Melanie Brignone, Pierre Fabre, 45 Place Abel Gance, FR-92100 Boulogne-Billancourt, France. E-mail: melanie.brignone@pierre-fabre.com
This systematic literature review and network meta- analysis showed that 5-fluorouracil interventions were associated with the best efficacy and a satisfactory acceptability profile compared with other field-directed therapies used in the treatment of actinic keratoses. These findings may contribute to inform treatment choices.
Actinic keratoses (AK) are common epithelial lesions characterized by keratotic macules, papules or plaques with superficial scaly growth caused by overexposure to ultraviolet (UV) radiation (1–4). AK is one of the most common pathologies seen by dermatologists; lesions are more common in men and the prevalence of AK increases steadily with age, fair skin phototype and cumulative sun exposure (3). The prevalence of the disease varies widely across different countries, with the highest prevalence seen in Australia (40–60%) due to its close proximity to the equator and large percentage of fair-skinned inhabitants (5, 6). In Europe, the estimated prevalence of AK in individuals >70 years is 34% in men and 18% in women (3, 5). With an ageing global population and younger patients increasingly presenting with AK (7), its prevalence and the clinical and economic burden of the disease are expected to increase substantially over the coming decades (5).
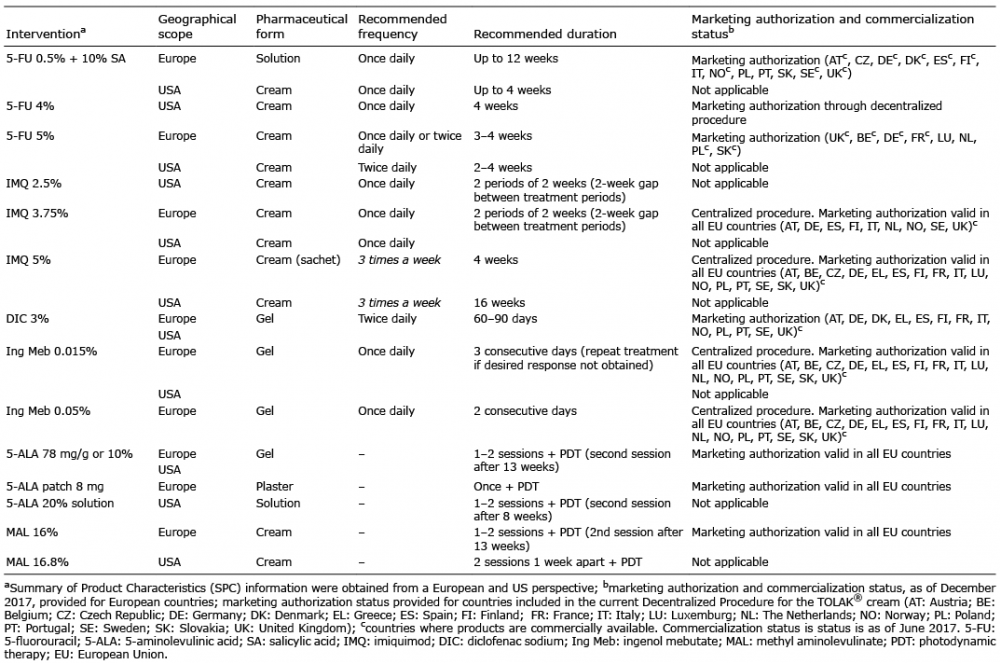
Given the risk of AK progressing to invasive squamous cell carcinoma (SCC), it is important to prevent its development and treat patients at diagnosis (1). Treatment options include either lesion-directed therapies that target discrete AK lesions or field-directed therapies that target multiple clinical lesions and the underlying field damage (8). Surgery, cryotherapy or ablative procedures (e.g. laser therapy) are mainly used to treat individual lesions, while topical treatments (with or without photodynamic therapy (PDT)), are used to treat both lesions and field damage (2). International treatment recommendations are based upon clinical presentation (single AK lesions (≥ 1 and ≤ 5 lesions); multiple AK lesions/field cancerization (≥ 6 lesions); immunocompromised patients with AK at any severity) (6). Current recommendations include the following field-directed treatments: 5-fluorouracil (5-FU; 4%, 5%, 0.5% (± 10% salicylic acid (SA))), diclofenac sodium (DIC; 3%), imiquimod (IMQ; 2.5%, 3.75%, 5%), ingenol mebutate (Ing Meb; 0.015%, 0.05%), 5-aminolevulinic acid (ALA) plus PDT and methyl aminolevulinate (MAL; 16.0%, 16.8%) plus PDT (6).
A systematic literature review (SLR) and network meta-analysis (NMA) were conducted in order to qualitatively and quantitively assess the comparative efficacy and acceptability of AK interventions, including the most recently approved intervention, 5-FU 4%, for the treatment of head-region lesions in immunocompetent patients with AK.
The protocols for the SLR and the statistical analysis plan for the NMAs were defined prior to the literature search and analyses, and in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (9) and health technology assessment body standards (Agency for Healthcare Research and Quality, USA, National Institute for Health and Care Excellence, UK, Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen, Germany, and Haute Autorité de Santé, France).
Eligibility criteria for trials included in the systematic literature review
Trials were eligible for inclusion if they were randomized controlled trials (RCTs; single-, double- or triple-blind or open-label) with either parallel or crossover design, where AK lesions of the face, ears and/or scalp were investigated in immunocompetent adult patients (≥18 years) with a diagnosis of AK and treated with an intervention of interest. The interventions of interest included field-directed therapy (5-FU (4%, 5%, 0.5% ± SA), IMQ (2.5%, 3.75%, 5%), DIC 3%, Ing Meb 0.015% and PDT using ALA or MAL), lesion-directed therapy (cryosurgery/cryotherapy, laser therapy or curettage, excision or shave biopsy) or other interventions (chemical peeling, adapalene gel, vitamin D, colchicine, tretinoin, isotretinoin, resiquimod). Placebo, another included intervention of interest (pharmacological and non-pharmacological) or any other intervention (pharmacological and non-pharmacological) served as comparators. Only records published in English were eligible for inclusion. In addition, clinical trial reports were provided for 5-FU 4%, a recently approved field-directed therapy.
Information sources and search strategies
Key biomedical literature databases (MEDLINE®, MEDLINE® In-Process and Embase® databases and the Cochrane Central Register of Clinical Trials) were searched using the relevant interfaces from inception to 29 November 2017. The database search strategies are shown in Table SI. In addition, relevant conference proceedings (published between January 2015 and November 2017) and ClinicalTrials.gov were manually searched and investigated for trials not published as full-text articles or to supplement results of previously published trials. A comparison of retrieved trials with bibliographic searching of included SLRs was performed to identify potential missing trials. Investigations were conducted in case of missing information.
Trial selection process
Two reviewers independently screened titles and abstracts of RCTs that were identified in the electronic database searches. For records that were considered relevant according to the title and abstract screening, full-text articles were obtained, and the eligibility criteria were applied by the 2 independent reviewers. Any trial selection discrepancies between reviewer decisions at either screening stage were resolved by a third independent reviewer.
Outcomes of interest
The SLR data were first qualitatively then quantitively analysed with the objective to undertake comparative analyses of field-directed treatments. The trials were qualitatively assessed and described. Efficacy outcomes of interest for the qualitative assessment were complete clearance of AK lesions (defined as the proportion of patients with no visible AK lesions (100% reduction) in the treatment area at the evaluation visit), partial clearance (the proportion of patients with 75% or greater reduction in AK lesion count in the treatment area at the end of trial visit when compared with baseline) and lesion count at baseline and endpoints. Complete and partial clearance rates were then defined as relevant outcomes for quantitative analyses, as they were more frequently reported than lesion count.
Acceptability outcomes of interest were withdrawals due to adverse events (AEs), occurring over the entire trial period and not limited to the treatment period.
Qualitative assessment for the systematic literature review
A descriptive analysis of the selected trials was performed (trial, patients, disease and treatment outcomes). An assessment of the quality of reporting was carried out using recommendations from the Critical Appraisal Skills Programme checklist for RCTs (10). Trials evaluating approved field-directed interventions administered according to their Summary of Product Characteristics (SPC) criteria, in addition to cryotherapy and laser therapy, were included in the qualitative analyses of efficacy and acceptability (Table I).
Table I. Interventions of interest
Feasibility assessment for the network meta-analysis
The RCTs identified in the SLR that assessed approved field-directed interventions underwent an assessment for inclusion in the quantitative assessment. The feasibility of performing an NMA to compare the interventions of interest quantitatively was assessed in the following steps: (i) the possibility of constructing a connected network of trials; (ii) the availability of data for each outcome of interest; and (iii) a comparison of trial and clinical characteristics that could modify relative treatment effect for each outcome. To be included in the NMA, trials identified in the SLR must have assessed approved field-directed topical interventions, including PDT, administered as monotherapy and according to their SPC. RCTs involving prior treatment as part of their methodology were excluded. Further information on the feasibility assessment is shown in Appendix S1.
Analytical approach
The interventions were compared using NMA methodology; NMA combines both direct and indirect evidence from multiple trials in order to determine the relative efficacy and acceptability of interventions of interest (11). The NMA was conducted within a generalized linear model framework, which has the flexibility to adapt to the structure of the data in line with National Institute for Health and Care Excellence Decision Support Unit guidelines (12). All outcomes analysed in the NMA were binary (clearance rates and withdrawal rates). Both fixed- and random-effects models were used for all outcomes. The choice between random- and fixed-effects model was based on model fit, as given by deviance information criteria (13) (i) when the difference in deviance information criteria between the 2 models is > 3, then the model with the lower value was selected as the preferred model and the conclusions were drawn based on the preferred model; and (ii) when the difference is < 3, then there was no preferred model and the conclusions were stated based on both the models (if the conclusions of both models agree it was noted that the conclusions were robust; however, if the conclusions did not agree, it was noted that there was insufficient evidence to draw statistical conclusions). Statistical heterogeneity was assessed for all the outcomes using I2 statistics; inconsistency was evaluated using Bucher’s method (14). Actual estimations were undertaken using Markov Chain Monte Carlo (MCMC) techniques using the statistical package WinBUGS 1.4 (MRC Biostatistics Unit, Cambridge, and Imperial College School of Medicine, London, UK).
The relative treatment effect between 2 interventions was calculated as odds ratio with 95% credible intervals (CrIs) or risk difference (RD) with 95% CrIs and forest plots; relative acceptability was assessed by RD values and forest plots. Treatments were ranked using surface under the cumulative ranking (SUCRA) probabilities. SUCRA is a numerical presentation of the overall ranking of each intervention and provides the probability of being the best treatment.
Base-case analysis was conducted on trials that provided results for the outcomes of interest at trial endpoint. To evaluate the robustness of the findings, sensitivity analyses were conducted for complete and partial clearance rates in order to avoid confounding results due to the variability in the clinical and methodological characteristics among the included RCTs. Key factors considered for these sensitivity analyses were the type of evaluation of complete clearance (clinical, histological, unclear), the assessment of the outcome as primary outcome, the exclusion of open-label trials, the evaluation of treatment effect at 4 weeks post-treatment and the use of intent-to-treat data only. The variables considered for analysis of each outcome for the base case and sensitivity analyses are summarized in Fig. 1.
Fig. 1. Criteria to be considered for analysis of each outcome of interest. AE: adverse event.
Trial characteristics
After removal of duplicates, screening and evaluation of eligibility of the 2,863 references identified at initial screening, 75 RCTs reported in 151 publications were included in the SLR (Fig. 2). Of these 75, 67 (89.3%) were published as journal articles, 22 (29.3%) were phase 3 and 42 (56.0%) had a double-blind design. The trial duration ranged from 4 to 104 weeks. A summary of key trial characteristics is shown in Table SII.
Fig. 2. Trial selection flow chart. aTotal of 128 non-priority trials from database searching and 15 trials from ClinicalTrials.gov that were included, but not extracted; bHDFUDR045 and HDFUP3S049 results were reported by Dohil et al. (15) and not discussed separately; cHDFUP4LTS050 (16) was an uncontrolled, single-group trial that assessed patients from previous trials (HDFUP3B048 and HDFUP3S049); dHauschild et al. (17) and Hauschild et al. (18) references have been counted as 2 trials and 3 publications. CTR: clinical trial report; AK: actinic keratoses; SLR: systematic literature review; SGA: subgroup analysis.
Patient and disease characteristics
Across the 75 RCTs, patients’ age ranged from 56.5 to 76 years, and the majority were male. Disease severity was reported in 24 trials (mild, n = 2; mild to moderate, n = 17; mild to severe, n = 5). Seventy RCTs reported details of baseline lesion count, which varied from a mean of 2.6 to 31.0 lesions per patient. The majority (n = 62) included patients with ≥ 5 lesions in their inclusion criteria. RCTs generally reported 10 lesions as the upper limit in their inclusion criteria, while fewer included patients with 15–20 lesions as the upper limit. In some trials, the baseline lesion count upper limit was not specified and was only reported in the baseline characteristics. A summary of key patient and disease characteristics is shown in Table SII.
Qualitative efficacy and acceptability
Complete clearance rates were reported in 36 RCTs (48.0%) that assessed field-directed interventions using approved doses, cryotherapy or laser therapy (Fig. 3A). Complete clearance rates varied across the RCTs for each intervention. Few interventions, which were reported in more than one trial, consistently achieved complete clearance rates ≥ 50%, i.e. 5-FU 5%, ALA-PDT and cryotherapy, not taking into account potential influencing factors such as sample size, baseline lesions count and time-point of assessments.
Fig. 3. Qualitative assessment of (A) complete clearance, (B) partial clearance, and (C) acceptability at trial endpoint. 5-FU: 5-fluorouracil; AEs: adverse events; ALA: 5-aminolevulinic acid; DIC: diclofenac sodium; IMQ: imiquimod; Ing Meb: ingenol mebutate; MAL: methyl aminolevulinate; PDT: photodynamic therapy.
Partial clearance rates were reported in 20 RCTs (26.7%) that assessed field-directed interventions using approved doses and varied for each intervention (Fig. 3B). As with complete clearance rates, partial clearance rates varied across the trials for each intervention. Interventions that consistently achieved partial clearance rates ≥ 50% in more than one trial included 5-FU 4% and 5-FU 5%.
Trial withdrawals due to AEs were reported in 24 RCTs (32.0%) that assessed interventions using approved doses (Fig. 3C). Interventions with ≤ 5% of patients experiencing withdrawals due to AEs in more than one trial included 5-FU 4%, 5-FU 0.5%, ALA-PDT, IMQ 2.5%, IMQ 3.75%, Ing Meb 0.015% and MAL-PDT plus laser.
Comparative efficacy and acceptability
In total, 31 RCTs contributed to the master network with the evaluation of 13 interventions, including placebo (Fig. 4A). The mean number of lesions at baseline was reported in 18 of the 31 trials, with a variation from 5 to more than 30 lesions at baseline (Fig. 5).
Fig. 4. Trials contributing to the base-case analysis for: (A) the master network, (B) complete clearance, (C) partial clearance, and (D) withdrawals due to adverse events (AEs) (1, 4, 16, 19-48). Line width is proportional to the number of direct evidence available in the literature. 5-FU: 5-fluorouracil; ALA: 5-aminolevulinic acid; DIC: diclofenac sodium; IMQ: imiquimod; Ing Meb: ingenol mebutate; MAL: methyl aminolevulinate; PDT: photodynamic therapy; SA: salicylic acid.
Fig. 5. Mean baseline lesion count in trials included in the feasibility assessment (1, 4, 22-24, 26, 28, 29, 33, 35, 38, 41, 42, 44-48).
For complete clearance, a total of 21 RCTs contributed to the base-case analysis, allowing comparisons among 13 interventions (Fig. 4B). Compared with placebo, significantly higher complete clearance rates were achieved with 5-FU 4%, 5-FU 5%, 5-FU 0.5% (cream), 5-FU 0.5% + 10% SA (solution), ALA-PDT, IMQ 5%, Ing Meb 0.015% and MAL-PDT vs placebo (Fig. 6A). A non-significant association, compared with placebo, was shown with IMQ 2.5% and 3.75%, as well as DIC 3%. The SUCRA values for complete clearance rate ranked 5-FU 5% as having the probability of being the best treatment among the interventions of interest, followed by 5-FU 4% (Fig. 7). The sensitivity analyses confirmed these results.
Fig. 6. Relative comparison of (A) complete clearance rates, (B) partial clearance rates, and (C) withdrawals due to adverse events (AEs) of all relative interventions vs placebo. 5-FU: 5-fluorouracil; ALA: 5-aminolevulinic acid; CI: confidence interval; DIC: diclofenac sodium; IMQ: imiquimod; Ing Meb: ingenol mebutate; MAL: methyl aminolevulinate; OR: odds ratio; PDT: photodynamic therapy; SA: salicylic acid.
Fig. 7. Surface under the cumulative ranking (SUCRA) values according to the probability of being the best treatment. 5-FU: 5-fluorouracil; ALA: 5-aminolevulinic acid; DIC: diclofenac sodium; IMQ: imiquimod; Ing Meb: ingenol mebutate; MAL: methyl aminolevulinate; PDT: photodynamic therapy; SA: salicylic acid.
For partial clearance, 10 RCTs contributed to the base-case analysis allowing comparisons among 10 interventions (Fig. 4C). Significantly higher partial clearance rates were achieved with 5-FU 5%, 5-FU 4%, IMQ 5% and Ing Meb 0.015% compared with placebo (Fig. 6B). The remaining 4 interventions showed a non-statistically significant higher partial clearance rate compared with placebo. The SUCRA values ranked 5-FU 4% as having the probability of being the best treatment to achieve partial clearance, followed by 5-FU 5% (Fig. 7). There was no change in the direction of these results in the sensitivity analyses, confirming the robustness of the findings.
A total of 9 RCTs contributed to base-case analysis for withdrawals due to AEs as a proxy of acceptability, allowing comparisons among 10 interventions (Fig. 4D). Compared with placebo, a numerically (non-statistically significant) lower risk of withdrawals due to AEs was observed with 5-FU 4%, 5-FU 5%, 5-FU 0.5% + SA 10% (solution), IMQ 2.5% and 3.75%, as well as Ing Meb 0.015% (Fig. 6C). The SUCRA values ranked 5-FU 0.5% + 10% SA (solution) as having the lowest probability of leading to withdrawals due to AEs, followed by IMQ 2.5% and 5-FU 4% (Fig. 7).
This analysis provides a comprehensive review of the available RCTs assessing various interventions in the current management of AK. It also provides comparative information for documenting the relative efficacy and acceptability profiles of these AK interventions. Both the qualitative SLR assessment and comparative NMA showed that 5-FU interventions were the most efficacious of the field-directed interventions examined on complete and partial clearance rates outcomes.
In an NMA using trials retrieved in a Cochrane review published in 2012, the 5-FU (0.5% and 5%) formulations were ranked first for achieving complete clearance, the only outcome that was evaluated (11). In addition, a multicentre, single-blind, randomized trial evaluating effectiveness of 4 frequently used field-directed treatments showed that 5-FU cream was the most effective of 4 field-directed treatments (IMQ 5%, MAL-PDT and Ing Meb 0.015%) after 12 months of follow-up in patients with multiple grade I–III AK lesions on the head (49).
Since these publications, 5-FU 4% was approved for the topical treatment of non-hyperkeratotic, non-hypertrophic AK (Olsen grade I and II) of the face, ears and/or scalp in adults. Clinical efficacy, safety and local tolerability of 5-FU 4% for treating AK lesions of the head region was demonstrated in an extensive clinical programme including 4 trials capturing treatment efficacy and tolerability: a randomized, evaluator-blinded, vehicle controlled, multicentre, phase 2 trial (15); a randomized, double-blind, parallel-group, phase 3 trial (15); a randomized, evaluator-blinded, vehicle-controlled, multicentre, phase 3 trial (48); and an open-label, multicentre, long-term safety trial (16). Clinical data from the phase 2 trial and both phase 3 trials were implemented in the present SLR and NMA to document the relative effect of 5-FU 4%.
This NMA was also conducted on additional outcomes: partial clearance as an additional measure of treatment efficacy and withdrawals due to AEs as a proxy of acceptability. Including additional outcomes to capture the broad treatment effect is important as variations in complete clearance rates across the trials were observed for each intervention. This could be attributed to differences in sample size, dose schedule within the SPC recommendations, time-points of assessment and baseline lesion counts across the trials. In addition, complete clearance rates were found to be influenced by the mean number of lesions at baseline (50).
In the present analysis, 5-FU interventions (4% and 5%) achieved the highest rates of complete clearance and partial clearance rates. Acceptability as an endpoint is clinically relevant, as compliance, and therefore clinical efficacy, is dependent on the degree of unwanted side-effects (49). 5-FU interventions (4% and 0.5% + SA (solution)) and imiquimod 2.5% were found to be the interventions leading to fewest withdrawals due to AEs.
In conclusion, this analysis showed that 5-FU interventions had the best efficacy, with a satisfactory acceptability profile. The findings from this analysis may, together with the evaluation of total costs in economic analyses, guide treatment choices.
Editorial and writing support was provided by Christina Campbell of Parexel International and funded by Pierre Fabre SA.
This analysis was sponsored by Pierre Fabre Dermatologie.
Conflicts of interest: KE is a consultant for Pierre Fabre. CP is an external consultant contracted by Pierre Fabre. MB is an employee of Pierre Fabre and has no conflicts of interest to disclose.


 Click to show fullsize
Click to show fullsize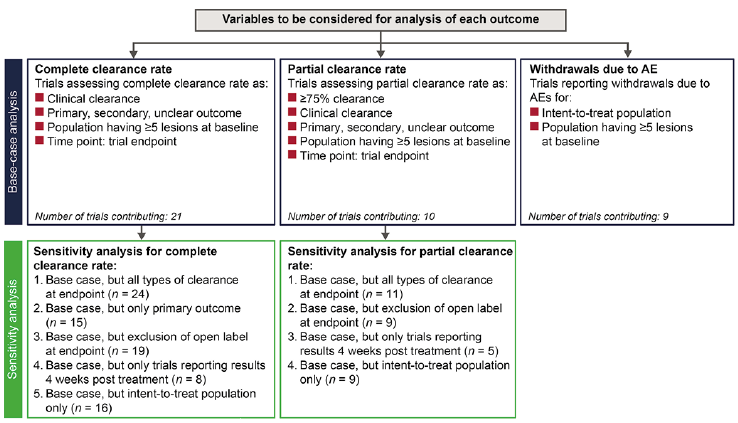 Click to show fullsize
Click to show fullsize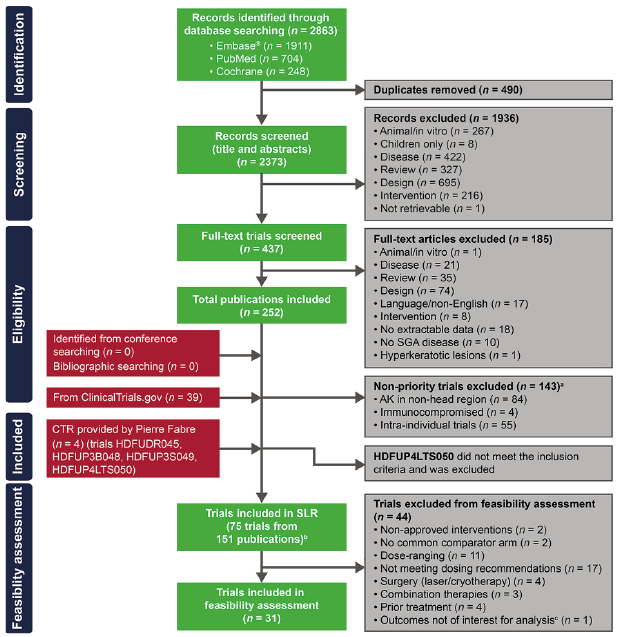 Click to show fullsize
Click to show fullsize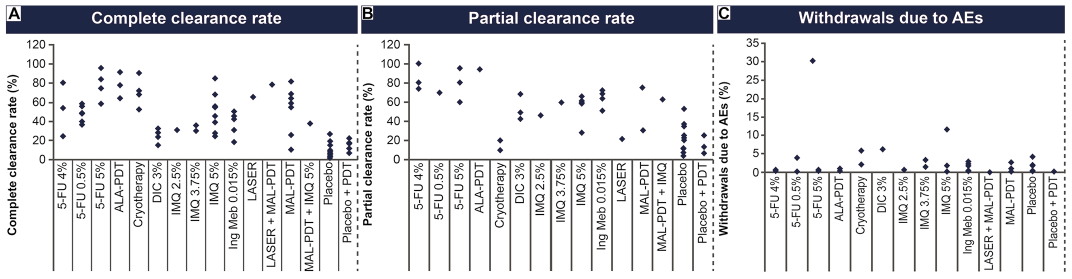 Click to show fullsize
Click to show fullsize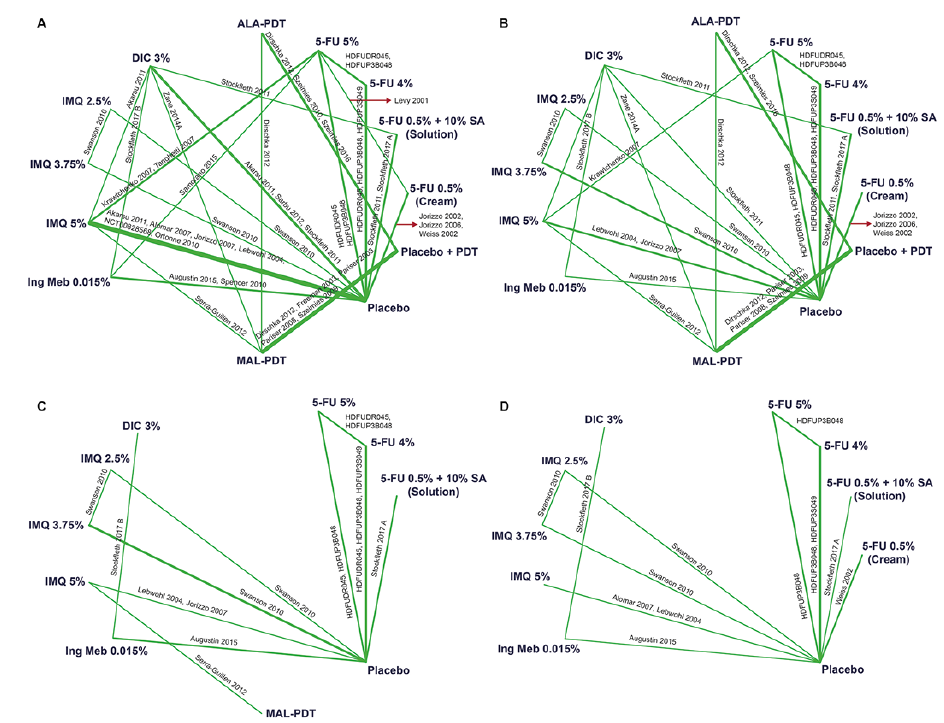 Click to show fullsize
Click to show fullsize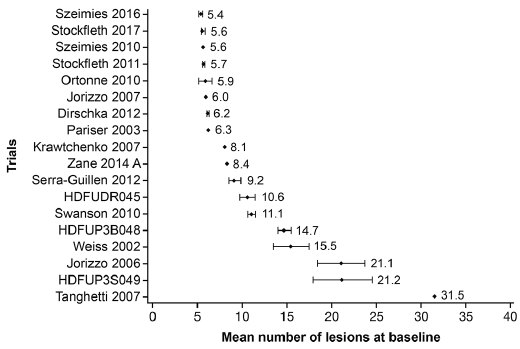 Click to show fullsize
Click to show fullsize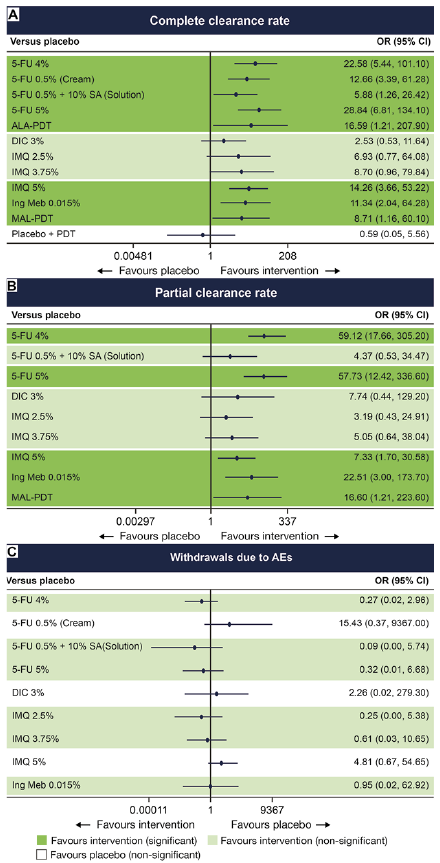 Click to show fullsize
Click to show fullsize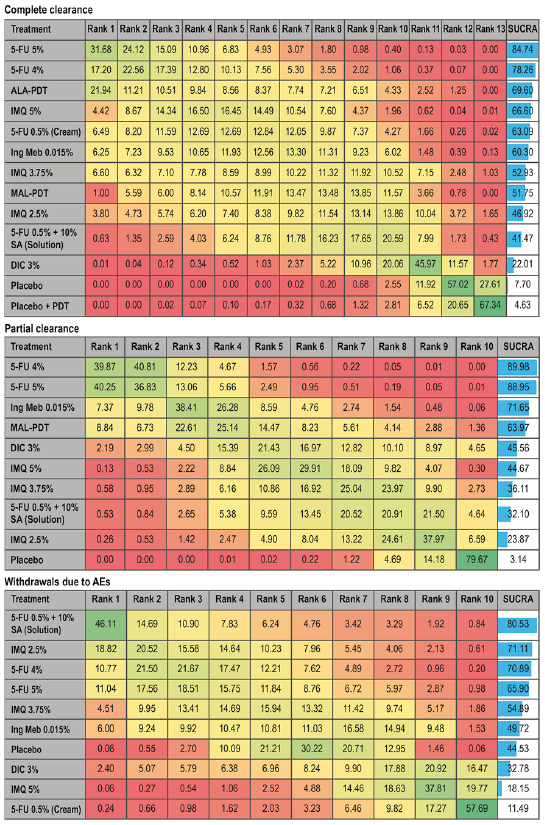 Click to show fullsize
Click to show fullsize