


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Chalubinskiego 1, PL-50-368, Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Accepted Dec 14, 2020; Epub ahead of print Dec 15, 2020
Acta Derm Venereol 2021; 101: adv00366.
doi: 10.2340/00015555-3729
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first identified in January 2020 as the cause of a viral pneumonia epidemic in Wuhan, China. Due to its rapid spread, it became a worldwide threat in a very short period of time (1). In March 2020 the WHO declared a pandemic of coronavirus disease 2019 (COVID-19) (2). Infection with other coronaviruses typically causes respiratory symptoms (1). In contrast, COVID-19 infection damages multiple body organs. Although the most frequent manifestations include respiratory tract symptoms (cough, loss of smell and taste), COVID-19 may also cause central nervous system (CNS) damage, renal injury, cardiological and haematological symptoms (3). In May 2020, 2 months after the beginning of the pandemic, our group published a report of the novel skin manifestation of COVID-19 (4), which was the first to report cutaneous hyperaesthesia in patients with SARS-CoV-2 infection. To date, after 5 months, no additional data has been published, and very little is known about the prevalence of this phenomenon. We believe that cutaneous hyperaesthesia remains a very rare clinical manifestation of COVID-19; nevertheless, it is not unique, and there are increasing reports of this manifestation.
In the 5 months since reporting this novel manifestation of COVID-19 (4), the authors have been contacted by several patients and/or their family members from around the world reporting similar symptoms. All patient data pertaining to the similarities and differences between subjects with skin sensitivity due to COVID-19 were collected. Each patient was also asked additional questions, with particular focus on additional dermatological symptoms that could have caused the above-mentioned hypersensitivity. Moreover, alleviating factors, medication, and duration of hyperaesthesia were taken in account.
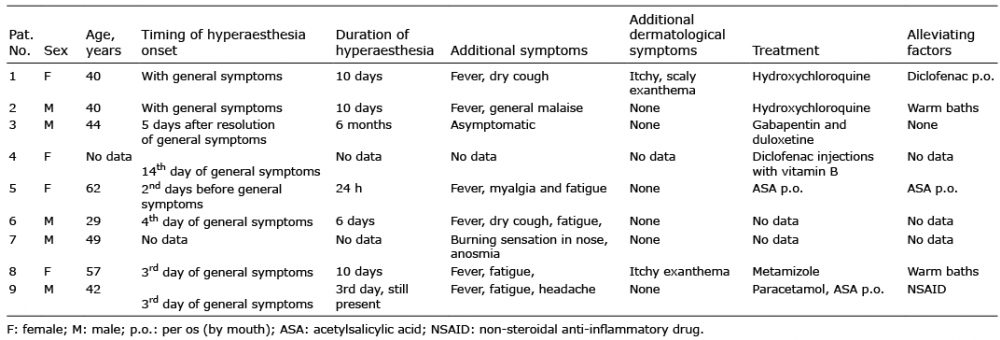
In total, this study collected data from 9 COVID-19 patients (4 women, 5 men, mean ± standard deviation age 47.7 ± 8.1 years) with cutaneous hyperaesthesia. The majority of the patients (6 people; 66.7%) presented typical general symptoms of COVID-19 (fever, malaise or dry cough) and only 2 reported associated dermatological manifestation. In both of those cases this was an itchy exanthema; however, in one of these patients this could have developed as a possible allergic reaction to paracetamol. Most frequently, hyperaesthesia appeared with, or directly after, the onset of general symptoms of COVID-19 (2–3 days); however, in one patient it was the first sign of the infection. Moreover, one of the patients reported increased sensitivity of the skin 5 days after the resolution of general COVID-19 symptoms. The duration of hyperaesthesia varied considerably among subjects (from 1 day to 6 months). The treatments applied were not similar between patients; 2 subjects were treated with hydroxychloroquine and 2 with symptomatic treatment (including acetylsalicylate and metamizole). Only 2 (22.2%) were treated for cutaneous hyperaesthesia (gabapentin/duloxetine and diclofenac injections). Among alleviating factors, patients most frequently reported oral, anti-inflammatory medication (22.2%) and warm baths (22.2%) (Table I).
Table I. Patients’ clinical characteristics
Neurological manifestations and complications are being frequently reported in COVID-19 patients. The mechanism of CNS and nerve damage is currently unknown; however, authors indicate a possible role of angiotensin-converting enzyme 2 (ACE2) receptors (found in glial cells and spinal neurones), disruption of the blood-brain barrier during viraemia, or invasion of peripheral nerve terminals (4). Although the most common neurological symptoms associated with SARS-CoV-2 infection are dizziness, headache, impaired consciousness and agitation, there may be also severe complications, including ischaemic and/or haemorrhagic stroke or encephalopathy (4–6). Subjective neurological symptoms (SNs) are common symptoms of COVID-19 and, according to Liguori et al. (7), may be present in up to 91% of subjects. The most commonly reported are hyposmia (38.8%) and dysgeusia (46.6%). Moreover, the authors found that some of the symptoms (sleep impairment, loss of smell and taste or headache) are significantly more common among female patients (8).
Cutaneous hyperaesthesia is a SNs, and is defined as an increased sensitivity to stimulation (8). Although frequent in primarily neurotropic viruses (e.g. herpes viruses) (9) it is a very rare manifestation of SARS-CoV-2 infection (10). Pain is an important problem in symptomatic patients with COVID-19, but the exact pathogenesis is unknown. Primary reports suggested that ACE2 receptor present in sensory neurones may play an important role in the uptake of SARS-CoV-2 and development of neurological effects (including nerve pain) (11). Interestingly, according to Moutal et al. (11), SARS-CoV-2 spike protein may decrease the pro-nociceptive signalling of vascular endothelial growth factor-A (VEGF-A) and act as an analgesic factor. It was demonstrated that VEGF may promote mechanical allodynia and thermal hyperalgesia; however, when blocked, these symptoms decrease significantly. Moreover, the authors raised the possibility that pain in COVID-19 may be diminished by spike protein, but did not exclude that other viral proteins may be pro-nociceptive (11). Nevertheless, it must be emphasized that that antibodies targeting VEGF- binding site of neuropilin-1 may cause neuropathy due to splicing of a neuroprotective isoform of VEGF-A (12).
In conclusion, further research is needed to determine the prevalence of cutaneous hyperaesthesia in COVID-19 patients and to clarify the pathogenesis of this symptom.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize