


1Department of Dermatology and Allergology and 2Anaesthesiology, University of Ulm, Albert Einstein Allee 23, DE-89081 Ulm and 3Department of Dermatology and Dermatosurgery, Helios Klinik Rottweil, Rottweil, Germany. *E-mail: lars-alexander.schneider@gmx.de
#These authors contributed equally.
Accepted Feb 16, 2021; Epub ahead of print Feb 19, 2021
Acta Derm Venereol 2021; 101: adv00440.
doi: 10.2340/00015555-3772
The incidence of non-melanoma skin cancer (NMSC) is increasing worldwide; in Germany it is expected to double by 2030, i.e. from 250/100.000 in 2012 to around 500 cases/100.000 incidence rate in 2030 (1). In 2004 a clinical study found that the recruited patients for Mohs surgery with cardiovascular monitoring in a Texas university center were on average 68 years old. (2). Since then, the number of older patients requiring micrographic or Mohs’ surgery has increased significantly and continues to increase (3). Today, even people over the age of 100 years may require skin cancer surgery (4). Surgery for dermatological tumours is generally regarded as safe, largely without complications, and resource-sparing. On a daily clinical basis this is indeed the case; however, as the patient demographics changes, care must be taken to maintain a safe environment and provide the clinical resources needed for safe practice. Resources such as theatre slots, nurses, anaesthesia time, hospital beds for observation, etc. are increasingly limited in many countries due to political decisions about health budgets. In more than 70% of cases skin cancer surgery involves reconstructive plastic surgery of the face or head and neck. Skin surgeons thus make an important contribution to maintenance of health and quality of life in these elderly patients. Demographic changes require more attention to be paid to specific age-related comorbidities, complex medication regimens, and physical and cognitive impairments that may complicate treatment of NMSC. All these factors define a specific medical need for staff time and care, as they may lead to increased risk of perioperative complications, stress, perioperative morbidity and even mortality (5). What is currently considered safe might not be so in the future.
The aim of the current study was therefore to assess the medical risks, perioperative morbidity and complications in patients undergoing micrographic dermatological surgery for NMSC in our department.
In a retrospective survey of 198 patients hospitalized between June 2012 and June 2013 at the Department of Dermatology and Allergic Diseases, Ulm University, Germany, patients’ comorbidities, medications, and peri- and post-operative complications were analysed using digital patient records and meticulous anaesthesia department documentation. The ethics board of the University of Ulm approved the study. Our department receives referrals from a population of 2.4 million in southern Germany. Patients referred to us are selected by outpatient-based dermatology clinics. Hence, the study subjects are inpatients and represent a selected patient population of a secondary referral centre.
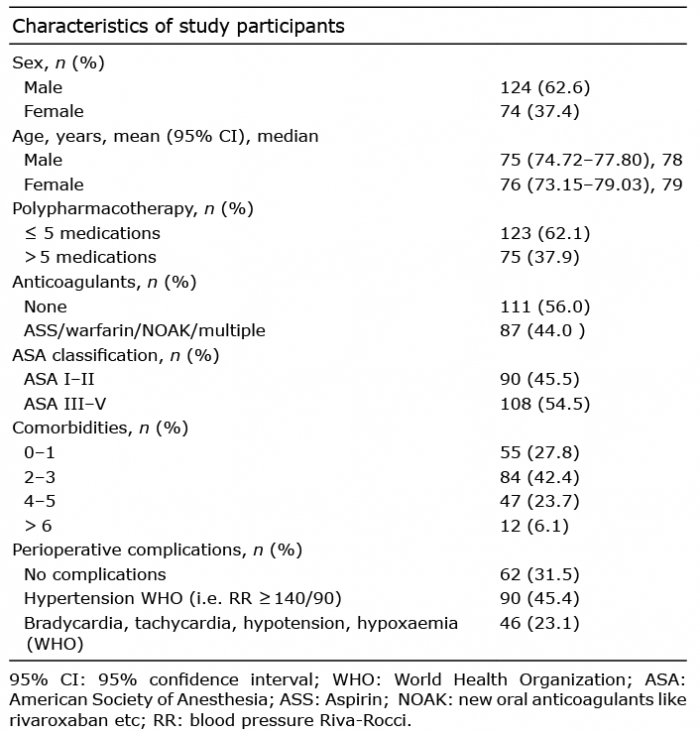
Table I shows the patients’ demographics and, together with Fig. 1, illustrates the results of the perioperative morbidity analysis. The median age of patients was 78 years, i.e. 10 years older than in Larson’s only partly comparable study from 2004 (2). Unsurprisingly, 85.8% of patients presented with at least one comorbidity, hypertension being most common (68.7%), followed by hyperlipidaemia (20.7%) and diabetes (19.7%). Risk factors for cardiovascular incidents were also detected in approximately 10% of cases, and 44% of patients were taking at least one anticoagulant, thus increasing the risk of postoperative bleeding. More than half (54.5%) of patients were preoperatively classified as American Society of Anaesthesiologists Classification (ASA) III and higher, defining patients with severe systemic diseases, significant functional limitations and, hence, increased perioperative risks. Almost one-third of subjects (29.8%) had 4 or more pre-existing illnesses, and could therefore be classified as “patients with multimorbidity”, and 37.9% were taking more than 5 regular medications and were therefore classifiable as “patients on polypharmacotherapy”. Correspondingly, the analysis of blood-pressure profiles perioperatively demonstrated hypertensive episodes during the operations in more than 45.5% of cases and cardiovascular temporary abnormalities, such as tachycardia or bradycardia (according to WHO criteria), in a further 23.1%. A total of 537 tumour operations were performed on our study population to remove skin cancer with micrographic surgery and repair the defects thereafter. Tumour operations in 62.2% of cases required anaesthesia staff to be on standby, due to pre-existing risk factors. Co-medication, to reduce pain, for sedation of the patient and alleviation of increased blood pressure, was often also administered as required; 60.9% of operations used additional remifentanil, often in combination or substituted by midazolam (5.8%) and propofol (16.8%). Despite the elderly and morbid cohort operated on at our centre, no deaths occurred in this patient population.
Table I. Demographic data and perioperative statistical risk assessment for 198 study participants undergoing micrographic tumour surgery due to skin cancer at the Department of Dermatology and Allergic Diseases, University of Ulm, Germany
Fig. 1. Prevalence of comorbidities in 198 patients with non-melanoma skin cancer surgery (total of 537 operations) at the Department of Dermatology and Allergic Diseases, University of Ulm, Germany. OSAS: obstructive sleep apnoea syndrome.
This study confirms that skin cancer surgery under the conditions described, with a very low rate of general anaesthesia of just 13% of all 537 operations, is safe and endurable, even for elderly patients. However, close monitoring and provision of staff to look after the cardiovascular wellbeing of the elderly patient population was key to safe practice at our centre.
To our knowledge, this study is the first analysis of pre- and peri-operative morbidity in patients with NMSC published in the last 10 years. These data demonstrate that the demographic change over the last 16 years has resulted in a referred hospital cohort of elderly patients with indicators for multimorbidity in our centre, requiring specific attention to medical needs other than the surgery for skin cancer, as well as provision of a safe perioperative care environment. Perioperative stress, often associated with skin surgery to the face, is not trivial, and may cause cardiovascular events, such as hypertensive episodes requiring patient observation as shown here. Even in a selected cohort, such as the current study cohort, this type of surgery is mostly performed under local anaesthesia; however, resources such as standby personnel for perioperative monitoring, and provision of intravenous medication via a drip in case of potential complications, as described above, ensure a complication-free intervention.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize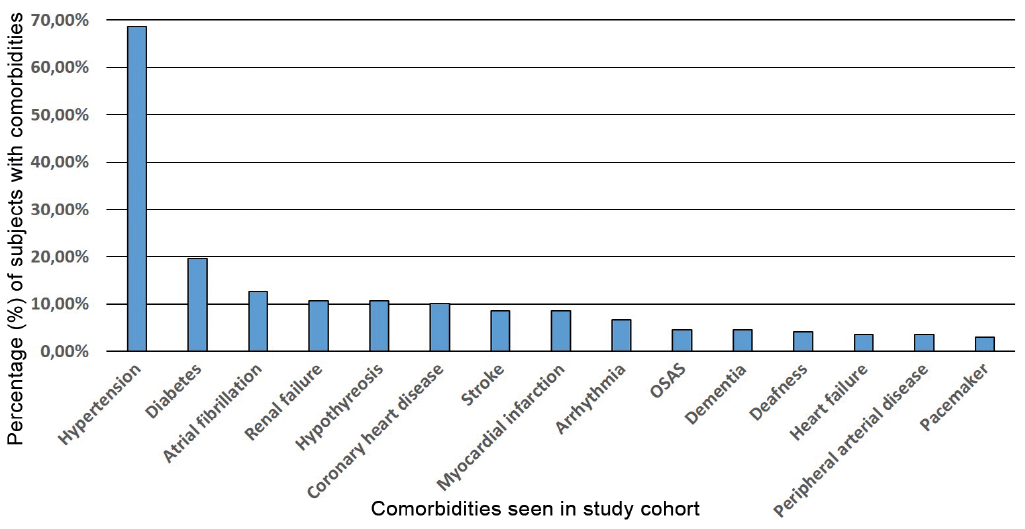 Click to show fullsize
Click to show fullsize