


1Department of Dermatology, Sheba Medical Center, Ramat Gan, 2School of Behavioral Sciences, The Academic College of Tel Aviv-Yaffo, Tel Aviv-Yaffo and 3Department of Pathology, Chaim Sheba Medical Center, Tel-Hashomer, Ramat-Gan, Israel. Affiliated to the Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
#These authors contributed equally to the manuscript.
Data regarding the impact of psychological factors in patients with pemphigus is sparse. This study evaluated the correlation of demographic, clinical, and psychological parameters with quality of life in 58 patients with pemphigus. Illness perception showed a realistic view, with the highest scores for cyclical course (3.35 ± 0.09) and treatment control (3.08 ± 0.06). Mean scores for perceived social support were relatively high from family and significant others (5.89 ± 0.18 and 5.66 ± 0.23, accordingly), and relatively low from friends (4.55 ± 0.24). There were no correlations between demographic, clinical parameters, perceived social support, and Dermatology Life Quality Index. Beliefs in cyclical course, emotional influence, psychological cause, and treatment control correlated significantly with quality of life. Stronger beliefs in self-control, chronicity, and accidental cause predicted higher quality of life, while stronger beliefs in cyclical course, psychological cause, and risk factors predicted lower quality of life. In order to enhance QoL, dermatologists should deliver the message to the patients that pemphigus is a chronic disease rather than cyclical and unexpected, and stress the patients’ role in controlling it.
Key words: pemphigus vulgaris; illness perception; social support; quality of life.
Accepted Mar 10, 2021; Epub ahead of print Mar 16, 2021
Acta Derm Venereol 2021; 101: adv00441.
doi: 10.2340/00015555-3785
Corr: Oz Segal, Dermatology Department, Chaim Sheba Medical Center, Tel-Hashomer, Ramat-Gan, Israel. E-mail: oz.segal@sheba.health.gov.il
Data on the impact of psychological factors on quality of life in patients with pemphigus are sparse. This study evaluated illness perception and perceived social support and their influence on quality of life in 58 patients with pemphigus. The results showed that patients had realistic illness perceptions and high perceived social support. Higher beliefs in personal control, chronic course, and accidental cause predicted higher quality of life, while higher beliefs in cyclical course, psychological cause, and risk factors predicted lower quality of life. The results indicate a significant influence of psychological factors on quality of life in patients with pemphigus.
Pemphigus vulgaris (PV) is a chronic autoimmune blistering disease affecting the skin and mucosa. Painful ulcerations affect the daily life of patients and require medical encounters, hospitalizations, and prolonged treatment. Pain and altered physical health lead to psychological comorbidities and impaired quality of life (QoL), both during active illness and in remission (1–5).
The significant impact of psychological factors, such as illness perception (IP) and perceived social support (PSS), on QoL has been described in different chronic medical conditions, and there are diseases in which the effect of these factors was reported to be higher than that of clinical severity (6, 7). IP comprises a patient’s beliefs about disease (8). It consists of 5 dimensions; identity (symptoms associated with the disease), timeline (disease course), consequences, control/cure (by treatment and personal), and coherence (understanding of illness and its causes). Among IP components, high illness coherence and personal and treatment control are considered as “positive” beliefs, while identity, timeline, and consequences are considered as “negative” beliefs (9). Patient IP is based on different sources of information, including physicians, other patients, relatives, friends, or media, and is often different from the IP of the physician (10). It has been reported that IP evolves as patients live with the disease, and varies between patients, leading to different behavioural responses (10). IP was found to be an important determinant of behaviour, functional recovery, and treatment adherence (6, 11, 12). PSS represents the subjective feeling of confidence about the availability of social interaction and support from family members, friends, and others when needed (13). A higher level of PSS was described as a promoter of adaptive coping and better physical and mental outcomes (13, 14). Both IP and PSS are subjective, and do not necessarily represent the correct status of the illness and social support (10). Increasing understanding of the impact of psychological factors on QoL and the potential effect of their modification on outcomes has led to numerous studies investigating these factors in different medical conditions (15). However, there is insufficient data regarding these factors and their correlations with Dermatology Life Quality Index (DLQI) in PV (5, 7).
The aims of this study were: (i) to assess IP, PSS, and DLQI among patients with PV; and (ii) to evaluate the relative contribution of socio-demographics, clinical parameters, IP, and PSS on QoL.
This cross-sectional study was approved by the Institutional Review Board (3925-17-SMC). Informed consent was obtained from each adult patient and, in a single case of a minor, from the parent.
Participants
The study population included patients registered as members of the National Israeli Association of Pemphigus who were hospitalized and followed-up in 3 tertiary care medical centres in Israel from January 2010 to February 2018. Only patients with clinical, histopathological, and immune-histochemical diagnosis of PV and complete data were eligible. Data were collected by 2 dermatologists (BS, SO) from patients’ charts and questionnaires. Evaluation of clinical data, IP, and PSS addressed the entire disease course, while DLQI assessed the current condition.
Characteristics evaluated
Socio-demographic. Age, sex, marital status, number of children, and education.
Clinical. Disease duration (years), severity (at diagnosis and current). Disease severity was defined as mild, moderate, or severe according to the extent and severity of involvement of the skin and mucosal membranes (16).
Illness perception. IP was evaluated using the Revised Illness Perception Questionnaire (IPQ-R) (17). IPQ-R consisted of 3 sections: identity, beliefs about illness, and causal dimension. The identity section included 14 general and 5 skin-related symptoms, graded as 1 or 0 (disease-related or not related, respectively), with total grade 0–19, and classified by frequency into very common, common, and rare (reported by 50–100%, 10–50%, and 0–10% of patients, respectively). The beliefs about illness section consisted of 7 subscales: (i) timeline of acute/chronic course (belief in how long the disease will last, with a higher score corresponding to a stronger perception of a long-lasting disease, 6 items); (ii) timeline of cyclical course (the patient’s awareness of the fluctuating disease course with flare-ups and remissions, 4 items); (iii) consequences (the perception that the illness has negative consequences on the patient’s life, 6 items); (iv) personal control (the degree to which a person feels able to control the illness, 6 items); (v) treatment control (the perception how effective is the treatment, 5 items); (vi) emotional representation (the extent to which the person has a feeling of emotional distress resulting from illness, 6 items); and (vii) illness coherence (the patient’s understanding of the illness, 5 items). Patients ranked each item on a 5-point Likert scale (1: strongly disagree to 5: strongly agree). Mean scores for each subscale were calculated. The causal beliefs section consisted of 4 subscales: psychological attributions (6 items), risk factors (7 items), immunity (3 items), and accident or chance (2 items). The 5-point Likert Scale was used for each item, and mean scores for each subscale were calculated.
Perceived social support. PSS was evaluated using the Multidimensional Scale of Perceived Social Support (MSPSS) (18). The questionnaire included the evaluation of 3 sources of support: family, friends, and significant others. Each item was rated using a 7-point Likert scale. Mean scores were calculated for each subscale.
Quality of life. QoL was assessed using the Dermatology Life Quality Index (DLQI), which included 10 items scored on a 3-point Likert scale (0: not relevant to 3: very much) (19). A total score was calculated for each patient and was categorized for effect on QoL, as follows: 0–1 no effect, 2–5 small effect, 6–10 moderate effect, 11–20 large effect, and 21–30 extremely large effect.
Data analysis
Categorical variables are presented as numbers and percentages. Continuous variables are reported as mean ± standard deviation (SD) and range or 95% confidence interval (95% CI). Descriptive statistics (means, SDs, and frequencies) were calculated for all variables. A repeated measure analysis of variance (ANOVA) was used to compare sections 2 and 3 of the IPQ-R. Relationships between clinical variables, IP, PSS, and DLQI were examined using Pearson’s correlations. Bonferroni tests were performed as a post-hoc analysis to identify the most prominent subscale in sections 2 and 3 of IP and PSS. To assess the contribution of each group of variables to DLQI, a Multivariate Binary Logistic Regression Model was used. This model was employed to assess the outcomes of DLQI as a categorical dependent variable (0, no influence; 1, presence of influence). Each group was entered into the model as a separate block (block 1: socio-demographic and clinical variables; block 2: IP variables; block 3: PSS variables). This analysis was performed to avoid a post-hoc procedure. All tests were 2-sided, and a p-value < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS software, version 23 (IBM Corp., Armonk, NY, USA).
Socio-demographic data
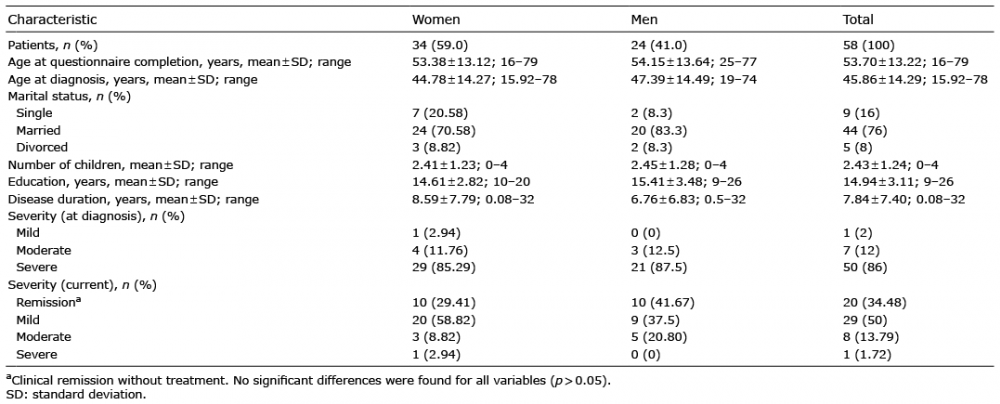
Of the 71 patients eligible for the study, 4 declined to participate, and 9 did not return the questionnaires. Thus, the study population comprised 58 patients: 34 (59%) women and 24 (41%) men. Socio-demographic data are shown in Table I. Mean age at diagnosis was 45.86 ± 14.29 years and at questionnaire completion 53.70 ± 13.22 years. There were no significant sex-based differences in age at onset, marital status, number of children, and years of education (p > 0.05).
Table I. Socio-demographic and clinical characteristics
Clinical parameters
Data regarding clinical parameters are shown in Table I. Mean disease duration was 7.86 ± 7.40 years. Most patients (> 85%) presented with a severe disease at presentation; most (85%) were in remission or had a mild illness at the time of completing the questionnaire. There were no significant differences in the severity and duration of the disease between men and women.
Evaluation of illness perception
Data regarding IP components are shown in Table II. Mean identity score was 6.67, which is not high. Among the beliefs about disease course, belief in a cyclical course was more dominant than that of chronic course (p < 0.011). In addition, belief in cyclical course was the most prominent subscale out of all subscales in the section. Belief in treatment control and illness coherence scores were also high. Evaluation of causal beliefs demonstrated the highest grading for psychological attribution to disease onset, followed by immunity, risk factors, and chance or accident. There were no significant differences in the scoring of any IP sections in relation to socio-demographic and clinical parameters.
Table II. Illness perception, perceived social support and dermatological life quality index
Evaluation of perceived social support
Data on PSS scores are shown in Table II. PSS scores were relatively high for all sources of support. PSS from family and significant others received significantly higher scores than PSS from friends. There were no significant differences found in PSS scoring in relation to socio-demographic and clinical parameters.
Evaluation of Dermatology Life Quality Index
Mean DLQI at the time of questionnaire completion was 4.59 ± 7.32, which indicates low impairment in QoL (Table II).
Correlation between clinical parameters, illness perception, perceived social support and Dermatology Life Quality Index
Data are presented in Table III. DLQI had significant positive correlations with several variables of IP, including belief in cyclical disease course, emotional influence, treatment control, and psychological attribution to disease cause. Out of the clinical variables, only disease severity at onset positively correlated with IP components, including beliefs in psychological attribution to disease onset and its consequences on the patient’s life. Current disease severity and duration did not show significant correlation with DLQI, IP and PSS. Several IP variables showed correlation with DLQI, and no such correlation was found for PSS. All PSS variables correlated with each other, and with several IP variables.
Table III. Correlations between clinical data, illness perception, perceived social support and quality of life
Multivariate binary logistic regression model for assessing variables that predict Dermatology Life Quality Index
Table IV presents the contribution of socio-demographic and clinical data (block 1), IP (block 2), and PSS (block 3) to DLQI. Out of the 3 blocks, the first and third blocks did not show a significant effect on DLQI, while the variables of block 2 accounted for 55% of DLQI variance. Of all IP components, higher beliefs in personal disease control, chronic disease course, and attributing chance or accident to disease causation predicted lower DLQI. Higher beliefs in cyclical disease course, influence of psychological aspects, and risk factors in the disease aetiology predicted higher DLQI. Since belief in personal disease control was the most significant variable related to DLQI, we created a receiver operating characteristic curve (20) to determine the cut-off level that would yield optimal specificity and sensitivity, over which belief in personal control has no impact on DLQI. Based on maximization of the area under the curve (0.596; 95% CI 0.44–0.75) a cut-off level of 3.17 was defined. Thus, patients with levels of belief of personal control ≥ 3.17 believed in a null effect of PV on their QoL.
Table IV. Multivariate binary logistic regression for prediction of Dermatology life quality index (DLQI)
This study evaluated the relationships between demographic, clinical, and psychological variables and QoL among patients with PV. The results revealed significant correlations between disease severity at onset and IP, within components of IP, within components of PSS, and between IP and QoL. There were no correlations found between socio-demographic and clinical variables, PSS, and QoL.
The mean DLQI in this study was lower than that described in studies in which it was evaluated at disease onset before the treatment, and it was similar to that reported in patients who were treated (5, 7, 21–25). Former studies focusing on chronic illnesses, including PV, have shown highest level of DLQI at disease onset that decreased following treatment (25). These results did not show a significant correlation between current disease severity and DLQI, which is consistent with previous reports that showed a lack of such correlation in several chronic medical conditions, but did find significant impact of psychological factors (7, 26, 27).
Overall, it appears that patients hold a rather realistic IP. They had correct beliefs about PV manifestations. Notably, in addition to classic manifestations, itch was also commonly reported. Given that pruritus is a frequent skin-related complaint, it is possible that it has been mistakenly attributed to PV. Another possibility is that pruritus is more common in PV than previously described, appearing more frequently in chronic stages, and thus receiving less attention in the literature. A recent study describing a high prevalence of pruritus in PV supports this hypothesis (28).
Although most patients believed that PV has a chronic and also cyclical course, the latter belief was dominant. A possible explanation is that, while current treatment allows a high rate of remission without persistent symptoms, patients still develop relapses, causing higher psychological impact due to their unexpected occurrence. Contrary to a former study, which demonstrated correlation between female sex and belief in cyclical disease course, and between marital status, disease duration and chronic disease course, we did not find such associations (7). Patients believed that their illness has significant negative consequences on their lives. This belief was significantly correlated with severity at onset, but not with disease duration, which is different from previous reports. This may result from advances in treatments’ efficacy, tolerability, and safety (7). The patients in the current study reported a strong belief in the ability of the treatment to control their illness. However, they felt that their own role in disease control is less crucial. High belief in treatment control has been reported as a promoter of adherence to treatment (12); however, when combined with low belief in personal control, it may cause impaired self-confidence, anxiety, and frustration, leading to lower QoL (29). In contrast, while a high level of personal control promotes better coping, when it is combined with low treatment control, it may decrease compliance (29, 30). Thus, for the optimal outcome there is a need for balance between treatment control and personal control. Increases in personal control can be achieved by directing patients towards the controllable aspects of disease management, such as maintaining oral and skin hygiene, physical activity, and following the treatment regimen. The favoured approach is shifting from a traditional treatment provider–patient relationship to a partnership with encouraging of an active patient role. This can be achieved by providing up-to-date information about disease, its treatment and outcomes, shared decision-making, referral to support groups and psychological counselling (24, 25, 29).
Although PV is rare, the current patients showed a high level of coherence, which was unrelated to age, education, or disease duration. Of note, proper coherence has been described as a promoter of better prognosis, with its enhancement resulting in better outcomes (31).
Similar to previous reports on PV and other skin disorders, such as vitiligo, psoriasis and alopecia areata, psychological trigger in current study was the dominant belief regarding disease aetiology, followed by immune alterations (7, 32). Psychological causation was related to disease severity at onset. Notably, a strong belief in a psychological cause was described in association with anxiety, depression, and impaired psychological well-being (33).
The current study has shown positive correlations between several components of IP, some “positive” (belief in treatment control and coherence), and some “negative” (identity, consequences, emotional influence and psychological attribution), and chronic and cyclical course. These correlations should be taken into account when planning to modify IP.
Although it is uncommon for rare disorders, PSS was high, with support from family being the highest, followed by PSS from significant others (34). Notably, the incidence of PV in the Jewish population is relatively high; therefore it is more recognized in Israel than in other countries (35). A high level of support from family is expected and important, because contacts with family are closer and more frequent compared with other relationships. The differences in PSS sources may result from age, cultural practices, and the availability of healthcare system (36). Membership in the National Israeli Association of Pemphigus, which is an active provider of information and support, may also have given an impact on PSS (37). The lower score for PSS from friends can be explained by fear of stigmatization and a desire to seek “medical-objective support” (34). There was no correlation between PSS and clinical parameters, but there was adverse correlation with IP components, including identity, consequences, beliefs in psychological causation, and risk factors. This supports the stress-buffering hypothesis proposing that PSS has a protective (buffering) role in persons who are under stress, from its pathogenic influence, and thus is related to well-being (13).
An assessment of the relationships between DLQI, socio-demographic, clinical variables, IP, and PSS revealed significant correlation only for IP components, including belief in cyclical course, emotional influence, psychological cause, and treatment control. When correlations with “negative” IP elements are predictable, regarding treatment control, we suggest that combination of high beliefs in cyclical (unpredictable) course and treatment control may represent a feeling of lack of self-control, leading to anxiety and a decline in QoL. The search for variables with a predictive value for DLQI also indicated several IP components, without an impact of socio-demographic, clinical parameters, and PSS. Higher beliefs in chronic course, personal control, and the causal role of chance or accident predicted lower DLQI, while higher belief in cyclical course, psychological attribution, and risk factors predicted higher DLQI.
Study limitations
There were several limitations in the current study. Due to difficulty in recruiting patients with a rare disease, the sample was relatively small, which could influence the results. DLQI was assessed only regarding current status and not throughout disease course. The study cohort had relatively low mean DLQI, which may prevent the results from being applicable to patients with severe disease. Multicentre prospective longitudinal studies evaluating QoL and psychological factors, together with assessment of stress, anxiety, and depression, are needed.
Conclusion
Patients with PV had a realistic IP. The strongest beliefs were those of cyclical course and treatment control. Perceived social support was high, especially from family. There was a lack of correlation between demographic and clinical variables, PSS, and QoL. There was significant negative correlation of IP variables, including beliefs in cyclical course, emotional influence, psychological causation, and treatment control, with QoL. Beliefs in chronic course, personal control, and the role of accident predicted better QoL, while beliefs in cyclical course, psychological causation, and risk factors predicted lower QoL. Thus, the results of the current study emphasize significant effects of psychological factors on QoL. In order to enhance QoL in PV, patient’s guidance should be focused on the chronic nature of the disease, which they can control, with the cyclic component of the disease course being less significant, and that there is no significant impact of a personal role, such as psychological trigger or risk factors, in its aetiology.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize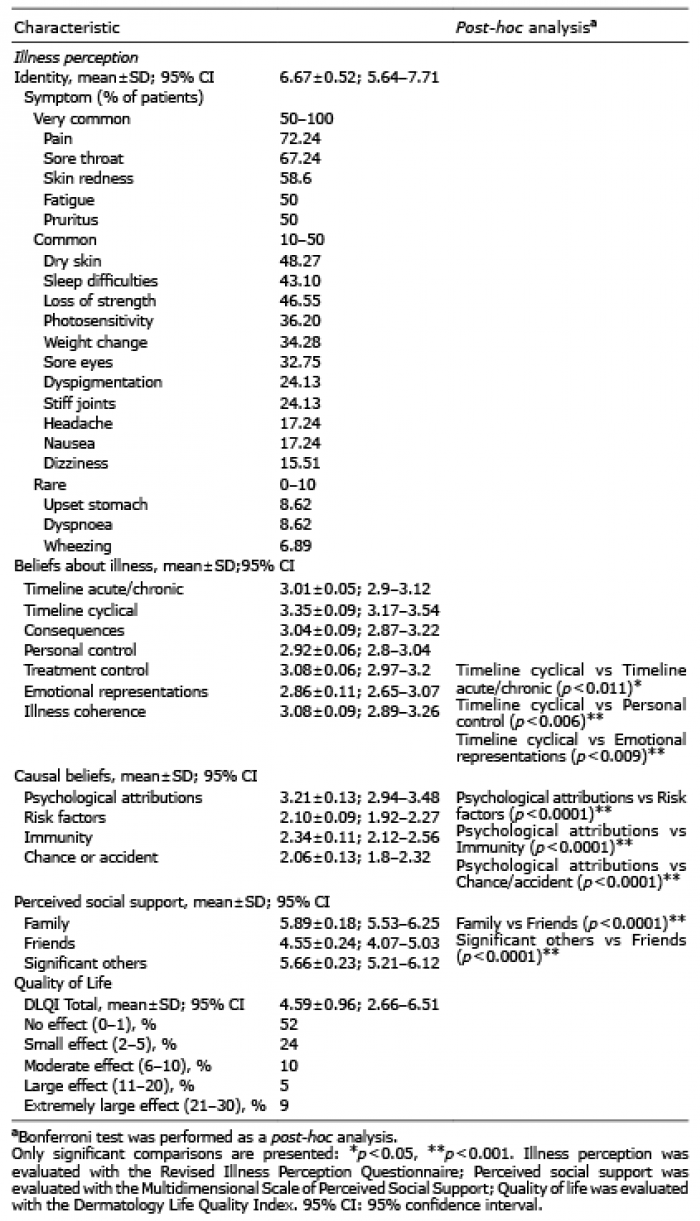 Click to show fullsize
Click to show fullsize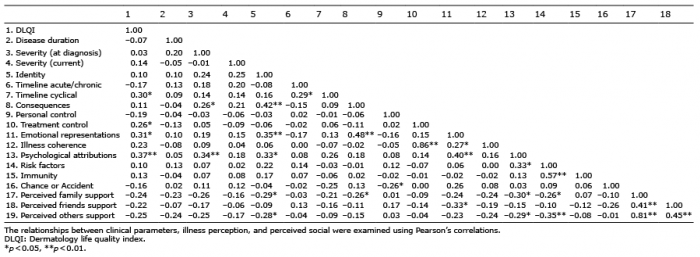 Click to show fullsize
Click to show fullsize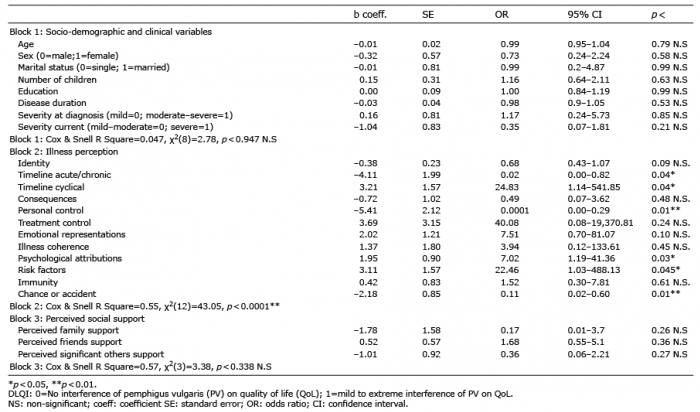 Click to show fullsize
Click to show fullsize