


1Department of Dermatology, 2Department of Pathology, and 3Department of Immuno-Hematology, Saint-Louis Hospital, Assistance Publique – Hôpitaux de Paris, Paris 7 University, 2 avenue Claude Vellefaux, FR-75010, Paris, France. E-mail: heloise.paugoy@aphp.fr
Accepted Mar 10, 2021; Epub ahead of print Mar 16, 2021
Acta Derm Venereol 2021; 101: adv00442.
doi: 10.2340/00015555-3787
Neutrophilic dermatoses are a heterogeneous group of disorders characterized by neutrophilic infiltration of the skin (1). Major types of neutrophilic dermatoses are pyoderma gangrenosum (PG), Sweet’s syndrome, subcorneal pustular dermatosis (SPD), erythema elevatum diutinum (EED), and aseptic abscess. They have been reported in association with various conditions, including autoimmune diseases, inflammatory bowel diseases, myeloid malignancies (acute myeloid leukaemia and myelodysplasia) and monoclonal gammopathies (MG). A previous study (2) revealed an association between IgA isotype MG and neutrophilic dermatoses, mostly EED, SPD and PG. Neutrophilic urticaria with systemic inflammation (NUSI) has been defined as neutrophilic urticarial lesions with fever in which the interleukin-1 cytokine could play a key pathophysiological role (3). Neutrophilic urticaria may be linked with inherited hyperactivation of the inflammasome pathway, such as NLRP3 gain of function (4), or external stimuli that may activate the inflammasome, such as IgM MG in Schnitzler syndrome.
We report here a case of a NUSI associated with an IgA myeloma.
A 65-year-old man with a 2-year history of IgA MG was referred to our department for a 2-year history of transient pruritic urticarial lesions (Fig. 1). The skin lesions lasted from 1 to 4 h, with an upsurge after 16.00 h, with no post-inflammatory pigmentation. The lesions were predominant on the trunk and limbs and spared the face. Alteration of the patient’s general condition was noted, with weight loss, asthenia, and fever. The patient had bilateral axillary and inguinal lymph nodes. No arthralgia was reported. High-dose H1-antihistamines (cetirizine 20 mg twice a day) were partially efficient.
Fig. 1. Urticarial lesions on the trunk and left arm.
Laboratory investigations ruled out common causes of chronic urticaria. They revealed elevated C protein level (20 mg/l, normal < 5 mg/l), elevated ferritin levels (470 µg/l, normal 30–400 µg/l), normal glycosylated ferritin (75%, 377 µg/l, normal 50–80%, 26–388 µg/l), mild normocytic anaemia (10.5 g/dl), lymphopaenia (980/mm3), slight increase in neutrophils (7,620/mm3), normal liver enzymes and serum creatinine levels, normal calcaemia (2.41 mmol/l), with kappa monoclonal IgA spike on serum protein electrophoresis and immunofixation (21.75 g/l, normal 1.04–3.37 g/l). Beta-2-microglobulin was increased, at 5.8 mg/l (normal < 2.2 mg/l). Bone marrow biopsy revealed a proportion of 38% abnormal plasma cells. Skin biopsy revealed perivascular and interstitial neutrophilic infiltrate of the entire dermis without leukocytoclasia or vasculitis, with moderate interstitial oedema and peri-sudoral neutrophilic infiltrate (Fig. 2).
Fig. 2. Histopathological findings. (a) Low-power view highlighting dermo-hypodermal neutrophilic infiltrate (Hematoxylin and eosin (HES) staining ×4 magnification). (b) Perivascular and interstitial neutrophilic infiltrate of the entire dermis without vasculitis or leukocytoclasia (HES ×25). (c) Peri-sudoral neutrophilic infiltrate (HES ×40). (d) Subcutaneous fat with perivascular neutrophilic infiltrate (HES ×25).
Computed tomography (CT) scan and 18-fluorodeoxyglucose positron emission tomography (18-FDG PET) scan showed bilateral axillary and inguinal adenomegalies of moderate intensity (maximum standardized uptake value (SUVmax) 6.4 and 7.5), but no osteolytic lesions. A biopsy of an axillary adenomegaly found reactive follicular and interfollicular hyperplasia with significant non-monotypic plasmocytosis. A diagnosis of a NUSI associated with an IgA symptomatic myeloma was made. Because of anaemia, asthenia, weight loss, and fever, plasma cell therapy was required. Treatment with Revlimid-Velcade-Dexamethasone-autologous stem-cell transplantation was started. A treatment regimen of bortezomib (1.3 mg/m2)/lenalidomide (25 mg, day 1–14)/dexamethasone (40 mg) resulted in a dramatic improvement in cutaneous lesions, fever, and disappearance of adenomegalies (after only 2 days of treatment). Spike of kappa monoclonal IgA became also undetectable. An autologous stem-cell transplantation was made after 4 cycles of chemotherapy. After 6 months follow-up, the patient was in complete remission, and receiving maintenance therapy with lenalidomide.
NUSI is considered more as a type of neutrophilic dermatosis than as a variant of urticaria. The presence of urticarial lesions with systemic inflammatory symptoms requires investigation for connective tissue diseases, such as systemic lupus erythematosus, urticarial vasculitis, adult-onset Still’s disease and Schnitzler syndrome. The clinical similarity of NUSI with autoinflammatory diseases underscores the possibility of a shared pathogenesis among all the diseases, centred on IL-1 dysregulation with subsequent neutrophil-driven inflammation.
Neutrophilic dermatosis associated with monoclonal gammopathy and myeloma include SPD (5–8), PG (9) and EED (10), mostly associated with an IgA isotype, and neutrophilic urticaria in the setting of Schnitzler syndrome mostly associated with an IgM isotypes (11, 12).
There were no formal criteria for Schnitzler syndrome, which is characterized by 2 obligate criteria (chronic urticarial rash, monoclonal IgM or IgG) and at least one of the minor criteria (Strasbourg criteria) (recurrent fever >38° unexplained, abnormal bone remodelling with or without bone pain, neutrophilic dermal infiltrate on skin biopsy, leucocytosis and/or elevated CRP). However, because of their similarities, a pathophysiological link between the current case and Schnitzler syndrome is possible.
Three cases of neutrophilic urticaria associated with IgA myeloma have been reported previously (13–15), but none had systemic symptoms. Rapid and complete resolution of skin, systemic symptoms and disappearance of the kappa monoclonal IgA spike after the start of chemotherapy suggests a pathophysiological link between NUSI and IgA immunoglobulin. Myeloma may be suspected in a patient with NUSI symptoms.
Patient consent was obtained and is available on request from the authors.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize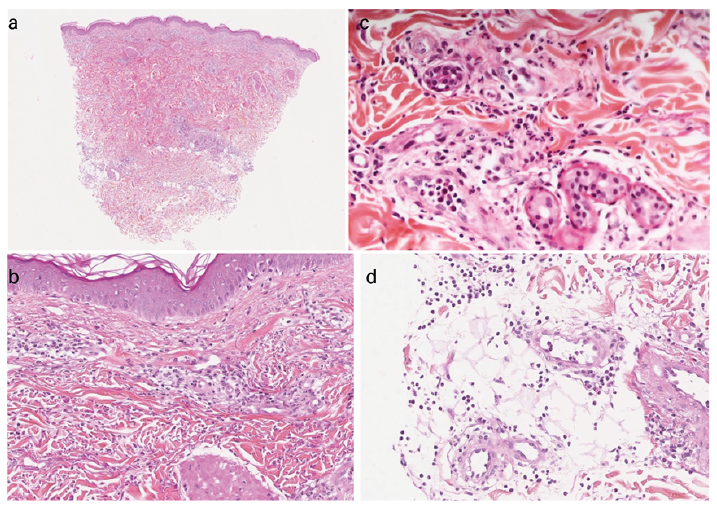 Click to show fullsize
Click to show fullsize