


1Pediatric Dermatology Unit and 2Surgical Pathology & Cytopathology Unit, Department of Medicine DIMED, University of Padova, Via Gallucci, 4, IT-35128 Padua, Italy. *E-mail: anna.bellonifortina@unipd.it
#These authors contributed equally and should be considered as first authors.
An 8-year-old girl presented with a 2-year history of an asymptomatic, erythematous, slowly growing, single plaque on the back of her right hand (Fig. 1A, B). The lesion had first presented as a small scaly plaque. Dermoscopic evaluation revealed uniform dotted vessels and white small scales in the middle of the lesion and a slightly elevated rim. After 6 weeks of daily application of betamethasone and salicylic acid dermatological examination showed more elevated edges and atrophic centre, with no reduction in plaque size. Dermoscopy revealed a whitish-pink homogenous area with a keratotic edge (Fig. 1C, D). The patient was generally in good health. No other family member showed similar lesions or were affected by skin diseases.
An incisional biopsy was performed with a 6-mm punch, with the aim of sampling both the atrophic centre and the elevated edge. At first observation, histopathological examination of the collected material revealed hyperkeratosis, psoriasiform acanthosis and focal cytopathic alterations (koilocytic changes) of the granulocytes of the granular layer, and the presence of cornoid lamella and invagination of the corresponding epidermis with absence of granulosum layer (Fig. 2).
What is your diagnosis? See next page for answer.
Fig. 1. Clinical photographs. (A) Initial clinical presentation. (B) Initial dermoscopic presentation. (C) Clinical presentation after betamethasone and salicylic acid treatment. (D) Dermoscopic presentation after betamethasone and salicylic acid treatment.
Fig. 2. Histopathological examination. (A) The obliquely oriented cornoid lamella contains parakeratotic corneocytes arising from a superficial dell, the base of which contains several dyskeratotic cells. (B) Close-up view of cornoid lamella shows the characteristic absent epidermal granular layer, many dyskeratotic keratinocytes and, on the right, koilocytotic alteration. (C) A discrete column of parakeratosis overlies a zone of hypogranulosis and dyskeratosis defining the cornoid lamellae (haematoxylineosin stain ×100).
Acta Derm Venereol 2021; 101: adv00428.
Diagnosis: Porokeratosis of Mibelli
Porokeratosis (PK) are a group of rare, acquired or genetic dermatoses, characterized by a keratinization disorder of unknown origin, clinically presenting annular or linear, well-limited, keratotic plaques. PK of Mibelli consists of a single or several annular plaques, usually unilateral and less frequently bilateral and symmetrical (1). The lesions initially form as keratotic plaques, which slowly expand in a centrifugal way. Subsequently, the lesions become annular, well demarcated, with an atrophic centre edged by a peripheral keratotic ridge (2); they rarely evolve to spontaneous remission (3).
As in the current case, the lesions are generally asymptomatic, but in some cases may be pruritic, especially in the body folds. The aetiopathogenesis of PK is complex and multifactorial, but is not well known (1); genetic factors, immunosuppression, ultraviolet (UV) exposure, drugs, infectious agents and trauma may play a role in pathogenesis. The mode of inheritance can be sporadic or familial, transmitted as an autosomal dominant trait, more commonly in a random form, which is probably the case for the current patient, since none of her relatives were affected by the disease (3). It has also been described an association with mevalonate kinase (MVK) gene mutation, which is usually related to disseminated superficial actinic porokeratosis (DSAP) (4).
Differential diagnoses of PK of Mibelli include several dermatoses, such as psoriasis, Bowen’s disease, squamous cell carcinoma, actinic keratosis, acrokeratosis verruciformis, seborrhoeic and stucco-keratosis (1, 3). In the current paediatric case we mainly considered plane wart, eczema, dermatitis artefacta, annular lichen planus and scarring, even though no previous trauma was reported.
Diagnostic confirmation is achieved via incisional biopsy, performed on the periphery of the lesion, and histopathological examination. The histopathology of PK is specific; it is characterized by a stack of tightly fitted parakeratotic cells, which are well limited from the rest of other corneocytes; it represents the cornoid lamella (Fig. 2A). In addition, under the column of parakeratotic cells, the granulosum layer is absent and the epithelium thinned (Fig. 2B, C) (3).
In the current case we also found focal koilocytic changes (Fig. 2C), which might initially suggest a diagnosis of a plane wart; this is an interesting finding, and another paediatric case also reported it (5).
The current case shows that the diagnosis of PK can be very challenging, and that PK should be considered even in very young patients.
There are no standards of treatment for PK, and no international and national guidelines. The best outcome for PK of Mibelli has been shown to be achieved when treated with imiquimod 5% cream, and that cryotherapy can be considered for smaller lesions (6). In order to replace deficient mevalonate pathway end-products related to the possible pathogenetic role of MVK gene mutation, the application of topical cholesterol/lovastatin has also been proposed recently as a possible treatment for PK (4, 7, 8).
Due to the young age of the current patient and the reduction in lesion size after incisional biopsy, she was started on daily topical application of calcipotriol, which resulted in clinical stabilization of the lesion.


 Click to show fullsize
Click to show fullsize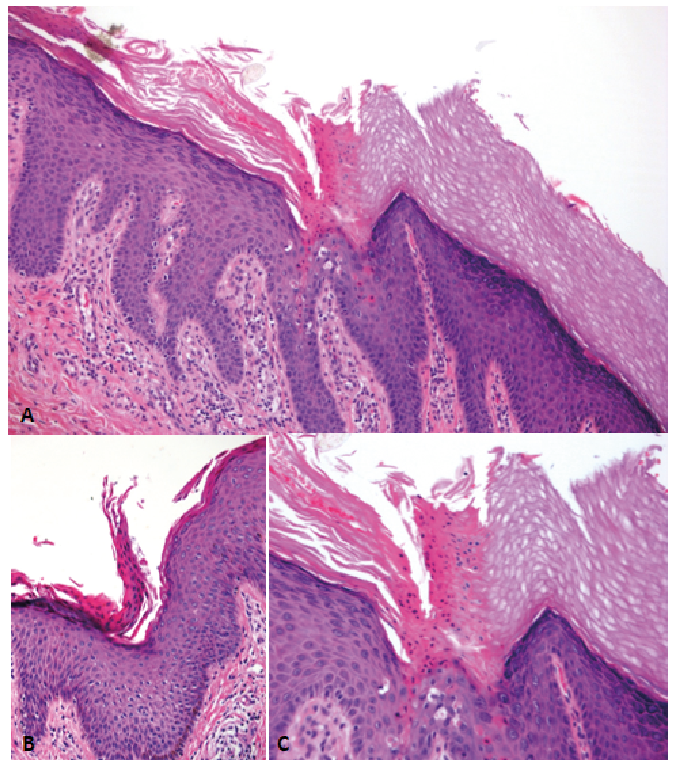 Click to show fullsize
Click to show fullsize