


1School of Healthcare Sciences, College of Biomedical & Lifesciences, Cardiff University, Eastgate House, Cardiff, 2Division of Musculoskeletal & Dermatological Sciences, Manchester Biomedical Research Centre, The University of Manchester, 3University of Manchester, The Dermatology Centre, Barnes Building, Salford Royal NHS Foundation Trust, Manchester, 4The Psoriasis Association, Northampton and 5Postgraduate Medicine, University of Hertfordshire, Hatfield, UK
The Psoriasis and Well-being (PsoWell)™ training programme, incorporating motivational interviewing, improves clinicians’ knowledge and skills to manage complex psoriasis, including behaviour change. The aims of this study were to deliver the PsoWell™ training programme to dermatology specialists, and to evaluate the acceptability and feasibility of implementing the PsoWell™ model across dermatology services. Frame-work analysis of 19 qualitative semi-structured interviews was performed, following delivery of nine, 1-day PsoWell™ training days involving 119 participants. Two themes were identified: “Perceptions and Priorities” and “Awareness”, sub-divided into: “Awareness Not Competence” and “Increasing Awareness”. The PsoWell™ model was found to be acceptable and feasible to implement across dermatology settings. Participants were more skilled and motivated to address psycho-logical issues, including behaviour change, but wanted further training to ensure competency. The trainees claimed that scepticism among some colleagues regarding whole-patient management might prevent uptake. Data show-ing the impact on health outcomes are needed and might overcome scepticism. Remote consultation could adopt the PsoWell™ approach.
Key words: psoriasis; psychodermatology; medical education; qualitative research.
Accepted Apr 14, 2021; Epub ahead of print Apr 15, 2021
Acta Derm Venereol 2021; 101: adv00445.
doi: 10.2340/00015555-3802
Corr: Rachael M. Hewitt, School of Healthcare Sciences, Cardiff University, 35–43 Newport Road, Cardiff CF24 0AB, UK. E-mail: hewittr2@cardiff.ac.uk
Dermatology clinicians considered the PsoWell™ model acceptable and feasible to implement in a broad range of UK dermatology service settings. The brief training described here facilitated clinicians’ knowledge and consultation skills for behaviour change. Participants felt that not understanding the importance of behaviour change in managing psoriasis was a barrier to implementing PsoWell™ in clinical practice. This approach to whole-patient management and service delivery could be adopted for remote dermatology consultations, both during and beyond the COVID-19 pandemic. Demonstrating that PsoWell™ improves patient health is the next step and might help to reduce these barriers to its use in clinical settings.
Psoriasis is a complex, long-term inflammatory skin condition affecting 2–3% of the UK population (1). Comorbidities are common (2) and the increased risk of cardiovascular disease (CVD) for some is associated with obesity, physical inactivity, excess alcohol consumption and smoking (3). Changing these health risk behaviours (3) underpinning these comorbidities (2) could offset the increased risk of CVD.
Most clinicians recognize the role of health behaviours in managing psoriasis, but may lack the knowledge, skills (4) or confidence to support behaviour change (BC) (5). Management of psoriasis has largely focused on physical symptoms (6). The aim of BC training for professionals is to enhance their communication skills (4), and to increase the motivation and confidence of professionals to address the wider impact of psoriasis (5). The COM-B model identifies Capability, Opportunity and Motivation as essential components in BC (7).
The fidelity of complex interventions should be tested rigorously not simply assumed (8). Some psychological interventions appear to be effective in psoriasis (9), but few have been subject to large-scale trials. Educational and self-management training interventions typically assess patient outcomes only (9), and few are specific to dermatology specialists. Generic studies show increased shared decision-making and discussion and assessment of CVD risk factors, but generally do not address psycho-logical illness and behaviours (10). Another study showed increased dermatologist satisfaction with care provision, discussion around well-being, and recognition of health-related quality of life (11). Specific training is required to address psychological aspects of psoriasis, support patient-centeredness and upskill clinicians in BC, in order to reduce psoriasis flares and CVD risk.
Motivational interviewing (MI) is a collaborative consultation style used to increase internal motivation and capability to develop goals and action plans for BC (12). This approach can bolster self-confidence in healthcare staff and facilitate effective self-management (13) of long-term conditions (14) including psoriasis (9).
MI training interventions can enhance patient under-standing of psoriasis without inducing anxiety and can facilitate a whole-person approach (15). PsoWell™ (psoriasis and well-being), an MI-based training programme and clinical initiative that advocates a holistic, multi-disciplinary approach to managing people with complex psoriasis, has been shown to improve psoriasis-related knowledge and consultation skills in primary and secondary care clinicians (16). PsoWell™ was deemed acceptable and feasible in a specialized setting (16). Thus, MI-based interventions benefit patients and enable clinicians to provide psychological support.
The PsoWell™ approach was developed in a specialist dermatology centre; the feasibility of incorporating MI in dermatology services with fewer resources is not known. The aims of this study were to deliver an effective PsoWell™ training programme in dermatology centres across the UK and determine whether participants considered this training and clinical initiative feasible and acceptable to implement within local dermatology services.
Design
A cross-sectional, qualitative study involving semi-structured interviews (SSI) via telephone.
Participants in the training programme
Dermatology consultants, specialist nurses and registrars, as well as health and clinical psychologists participated in training.
Recruitment
Training programme. Snowball sampling using research team contacts within dermatology, psychodermatology and psychology departments of the National Health Service (NHS) trusts and boards and academic organizations, assisted by recruitment. Flyers containing study information, participant information sheets, and Uniform Resource Locators (URLs) for the forms for registering interest and training application (Appendix S1, appendices A–D) were distributed to contacts.
The study aimed to recruit at least one doctor and one nurse from a centre. Training sessions were organised in geographical locations where demand for training was highest; areas across the UK where we received the largest numbers of registering interest forms from potential participants.
Training places were funded by Psoriasis Association UK and were limited to 20 per group in order to enable individual skills coaching and maintain training quality.
Evaluation. Post-training, participants were invited via e-mail to participate in a SSI via telephone. There was no strict recruitment criteria, although purposive sampling was used to ensure that the sample included at least two participants from each training session and represented a wide range of clinical roles from different dermatology services across the UK.
Training intervention
Aim. A 1-day MI training programme (16) aimed to improve clinicians’ knowledge and skills for BC and enable them to integrate MI techniques into routine dermatology consultations.
Format. Lectures and interactive sessions plus individual coaching were delivered by experienced MI practitioner-trainers. The training agenda, including the content, type and length of sessions, are described in Appendix S1, appendix E.
Materials
Workbook. The training workbook (16) contained support materials for participants. A certificate for individual participants and a clinic certificate for dermatology teams were awarded on completion of training.
Interview schedule. Questions (see Appendix S1, appendix F) focused on the acceptability of the PsoWell™ model in clinical practice; the feasibility of upscaling and implementing the model in dermatology settings; and its usefulness in achieving a patient-centred consultation for BC.
Procedure
Ethics approval was obtained from Cardiff University Research Ethics Committee.
Training programme. Sessions were organized across nine UK regions in conference and academic centres from October 2019 to February 2020. Participants provided written informed consent and populated a demographic questionnaire (see Appendix S1, appendix G) to enable selection for the evaluation interview.
Semi-structured interviews. Encrypted audio-recorded interviews lasting 48–80 min were professionally transcribed verbatim.
Analysis
Semi-structured interviews. The Information Power Model (17) was used to determine the sample size. Data collection stopped when adequate information power was achieved: the comprehensive aims and cross-case analysis were balanced by the evidence, theory-based interventions and analysis; purposive selection from the target population; and high-quality dialogue generated from the interview schedule.
Framework analysis was conducted from an essentialist/realist epistemological standpoint describing the “experiences, meanings and reality of participants” (18). This method facilitated a systematic and transparent analysis of interview data (19).
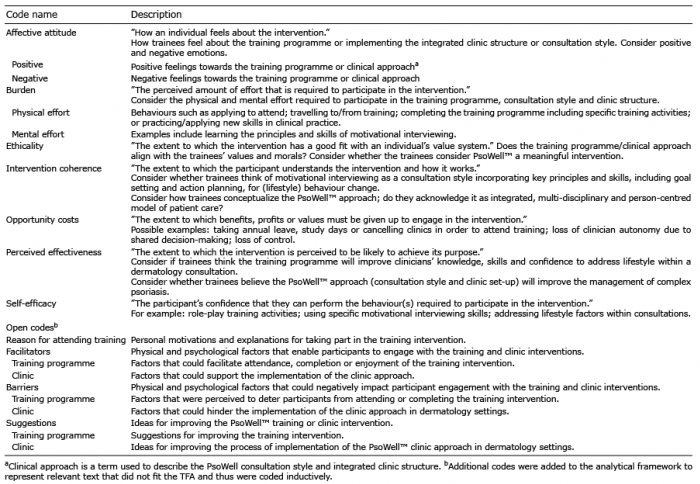
Transcripts were deductively coded against constructs of the Theoretical Framework of Acceptability (TFA) to determine the retrospective (experienced) and prospective (perceived) acceptability (20) of the PsoWell™ approach. Relevant text that did not fit the TFA was coded inductively.
Two authors independently coded one transcript before meeting with the research team, in order to check the consistency of coding, resolve discrepancies, and revise the framework accordingly. This process was repeated until agreement was reached. The first author applied the framework (Table I) to the remaining transcripts and the second author routinely sampled excerpts to ensure consistency. The transcripts were coded in NVivo. Surface-level themes were identified, refined and defined.
Table I. Theoretical Framework of Acceptability (TFA)
Of the 156 people who applied, 119 (76%) completed the programme in 9 locations. Participants’ demographics are described in Table II. Nineteen participants (3 males and 16 females) were purposively selected for interview comprising 6 dermatology consultants, 5 specialist nurses (2 with academic posts), 3 psychologists and 1 each of the following: dermatology registrar, GP with specialist interest in dermatology, advanced care practitioner and dermatology research fellow.
Two themes were identified: “Perceptions and Priorities” and “Awareness”, further subdivided into: “Awareness Not Competence” and “Increasing Awareness”.
Table II. Demographic information of 119 participants who attended the PsoWell™ training programme
Perceptions and priorities
Clinicians reported that medical school had not prepared them to manage complex psoriasis, and that addressing BC, especially for weight management, was challenging. All attended to improve their skills to ensure they were:
“giving the patient the best consultation” (specialist nurse);
“really seeing it as a priority, and not seeing it as an optional thing but thinking right this is as important as talking about side effects of medication” (consultant dermatologist).
Although no formal training barriers were identified, time away from clinic was the “main restriction” (dermatology registrar), with distance to travel to the training programme another. One participant observed that traditional models of psoriasis management and clinical job roles do not acknowledge psychological and behavioural factors and thus are a potential barrier:
“there are barriers in terms of feeling that this sort of work is for counsellors and psychologists as opposed to… the more usual found jobs in a dermatology department… and therefore struggling to make time for it … because of a belief that it’s not, it’s not part of their role” (clinical psychologist).
However, one participant felt barriers were not insurmountable: “I think if people had really wanted to come they’d have just got round it” (specialist nurse and lecturer). Clinicians noted the benefit of the PsoWell™ approach and supported implementation:
“PsoWell and motivational interviewing is really something that should be incorporated in-into all consultations” (consultant nurse).
“As well as job satisfaction I think that it is likely to lead to better outcomes for patients… it’s likely to be more cost effective for the department but also, for …, for the trust as a whole” (clinical psychologist).
Negative perceptions of mental health provision, long waiting lists and individual motivation were perceived barriers to patients attending appointments. Conversely, the integrated interdisciplinary PsoWell™ approach to care may be acceptable to patients, who report that they “want more of it” (counselling psychologist).
Clinicians working in interdisciplinary teams highlighted the value of co-treating patients:
“each practitioner can bring an expertise that would be usually absent… we’ve shown in psycho-dermatology clinics that to have that multi-disciplinary approach is clinically beneficial for the patient but also more cost-effective for … commissioners” (consultant dermatologist).
Furthermore, there was a clear need and desire for dedicated psychological support in dermatology:
“It’s something that we definitely need that we don’t know we need… both from a clinical team perspective, but also from a patient perspective” (consultant dermatologist).
A lack of mental health services and inequities in psychology provision were identified as “broader” (consultant dermatologist) problems within the NHS. Barriers to employing psychologists included insufficient funding and clinic space. Some believed that MI was time-consuming to implement within standard consultations, yet this was not always the reality in clinical practice:
“I thought it [MI] would end up making the consultation longer but it actually makes it shorter” (consultant dermatologist).
Similarly, the cost of employing psychologists was raised:
“I’m not sure why they [doctors] think it’s expensive… they don’t compare it against, what actually they can save, the sort of benefit it might have in terms of use of medication… they don’t do all the health economics, that Psychology might involve… it’s a little bit more complicated, than actually saying, it’s just a salary” (counselling psychologist).
Individual perceptions of job roles and time restraints may negatively affect willingness to complete PsoWellTM training. Implementation of this inter-disciplinary clinic approach to patient care will depend on service leaders’ perceptions of its value.
Awareness
Awareness not competence. The training included experiential and vicarious learning with feedback through role-play activities, which, despite being something that people found challenging, was considered fundamental for MI skills:
“I actually got quite a lot out the role play, even though we all hate it was quite interesting to watch and learn from” (advanced care practitioner).
Working alongside clinicians and academics with similar “ideologies” (consultant dermatologist) provided a valuable learning opportunity to discuss experiences and “disintegrate any sense of … hierarchy” (consultant dermatologist). Following training, clinicians felt more confident to support BC:
“It gave me the confidence in knowing how to … open up those conversations on behavioural change, which maybe I found more difficult to do beforehand” (specialist nurse).
Clinicians did not claim MI expertise: “I don’t feel skilled particularly in MI” (specialist nurse and lecturer), but seeing skills demonstrated encouraged them to be more mindful of their clinical practice:
“it was an extremely beneficial day that…, made me aware of different ways of conducting a consultation that I wouldn’t have known about before and techniques that I will put into clinical practice, that I think will improve the overall management of my patients” (consultant dermatologist).
MI techniques were viewed as “the sort of things that you sort of need to practice and sort of develop over time” (consultant dermatologist). The training materials were considered a useful prompt for continued MI practice, but practical follow-up sessions were requested to increase confidence in supporting health BC.
Increasing awareness. Increased psychology provision within dermatology services was desirable, but most recognized the need to demonstrate improved patient outcomes to convince budget holders to prioritize and invest in psychologists:
“The ones who make the decisions… they have a finite pot and I think we just need to kind of raise, I don’t know, raise the profile or show more the benefits of, of having a psychologist in a service, in a way which is understood by budget holders, or service commissioners” (specialist nurse).
Increasing awareness of the benefits of this approach at the service and policy level is necessary to ensure implementation of the PsoWell™ model.
Participants felt better prepared to address BC with relevant patients, but required further training to ensure competence. Outdated or inaccurate beliefs of colleagues, commissioners or service managers might prevent increased specialist psychological support from becoming a funding priority
This study replicated and extended the original PsoWell™ training programme findings (16) in a wider sample of clinicians from primary, secondary, community and non-specialist settings. Participants reported being more knowledgeable, skilled and confident to address BC for the management of psoriasis and CVD risk and reported their clinical practice and research is aligned with the PsoWell™ approach. This was expressed most clearly among clinicians from multi-disciplinary teams including psychologists. As well as increasing capability, training renewed clinicians’ motivation and enthusiasm to provide holistic patient care through interdisciplinary working, and helped them to create opportunities during their routine consultations.
“Personal models” (beliefs, emotions and experiences) of psoriasis influence clinicians’ approaches to patient care (21). The current participant sample indicated that dermatology staff who did not believe they should address well-being or BC were unlikely to attend training, reinforcing the key role of beliefs about psoriasis in delivering whole-person care.
Implications for practice
There is a gap in the medical curriculum relating to the wider impact of psoriasis on other conditions, including the role of health behaviours as risk factors for those conditions. The importance of communication skills training for medical practitioners is now widely recognized (22). The inclusion of MI to address psychological issues and BC across long-term conditions would be beneficial.
PsoWell™ is an acceptable framework for the holistic management of psoriasis and, potentially, other dermatological and long-term conditions. This study reinforces the desire amongst dermatology clinicians for dedicated psychological support provided by psychologists as well as, not instead of the PsoWell™ approach, but this information should be communicated to service commissioners. Resourcing this initiative may be challenging, due to the impact of COVID-19, although the subsequent shift towards remote service delivery presents a valuable opportunity to deliver MI in a cost-effective manner.
Implications for future research
This study demonstrates that brief intervention to address BC is acceptable to dermatology clinicians. Further research is needed to determine if the PsoWell™ approach improves patient outcomes compared with standard treatment in psoriasis.
In 2018, the top priority of the James Lind Alliance Psoriasis Priority Setting Partnership was support for health-related BC in managing psoriasis. Testing psycho-logical interventions for patients was also in the top 5 priorities (23). Those with psoriasis and increased risk of CVD because of obesity and inactivity constitute a vulnerable group who are at greater risk of contracting COVID-19 (24), making this programme of work a priority.
Strengths and limitations
An established BC theoretical framework was used to make this intervention reproducible. The training programme was tailored rather than generic and was delivered by experts in MI with experience in working with people with psoriasis, therefore, ensuring quality.
Self-selection of participants may limit this work, as participants were motivated by the content and may not represent the wider dermatology community. The first author co-delivered the training sessions and conducted the interviews, thereby potentially introducing bias towards participants’ positive training experiences. Finally, the lack of real-time evaluation of the use of MI skills is arguably a limitation; however, our previous work established an increase in clinicians’ consultation skills using this approach (16).
Conclusion
PsoWell™ training is a necessary and acceptable BC intervention. Participants claimed it increased their capa-bility, confidence and motivation to support health BC in patients. They believed that, with adequate resourcing, they could implement this training as part of their whole-person management practice. The COVID-19 pandemic has changed the way dermatology services are delivered. NHS trusts should capitalize on these changes to provide cost-effective MI training for staff and increase dedicated psychological support in face-to-face and remote dermatology consultations.
The authors thank the Psoriasis Association UK for funding this work (grant number 50 P/1/515477), and the participants for their valuable contributions to recruitment, the training programme and interviews.
CEMG is a National Institute for Health Research (NIHR) Emeritus Senior Investigator and is funded in part by the NIHR Manchester Biomedical Research Centre.
This study was funded by the Psoriasis Association UK.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize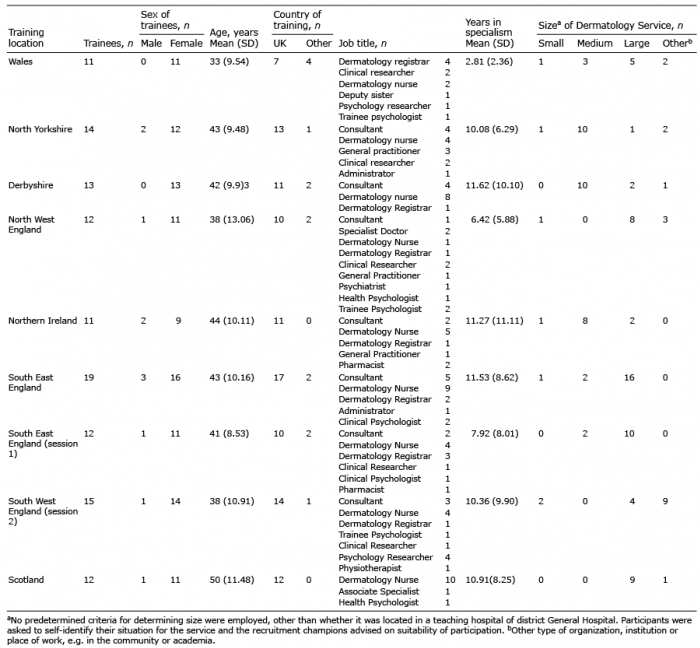 Click to show fullsize
Click to show fullsize