


1Istituto Dermopatico dell’Immacolata-Istituto di Ricovero e Cura a Carattere Scientifico (IDI-IRCCS), Dermatological Research Hospital Rome, 2Dermatology Unit and Genodermatosis Unit, Genetics and Rare Diseases Research Division, Bambino Gesù Children’s Hospital, IRCCS, Rome, 3Dermatology Unit, 7Department of Biomedical Science and Human Oncology, University of Bari, 4Dermatology Unit, A. Perrino Hospital, Brindisi, 5Dermatology Unit, Oasi Scientific Institute, IRCCS, Troina, 6Dermatology-IRCCS Policlinico di S.Orsola, Department of Experimental, Diagnostic and Specialty Medicine (DIMES), Alma Mater Studiorum University of Bologna, Bologna, Italy, and 8Department of Dermatology, Reference Centre for Genodermatoses (MAGEC) Necker Enfants Malades Hospital, Imagine Institute, FIMARAD, Paris Centre University, Paris, France
#These authors contributed equally and should be considered as first authors.
Autosomal recessive congenital ichthyoses (ARCI) are characterized by generalized skin scaling, hyperkeratosis, erythroderma, and disabling features affecting the skin (palmoplantar keratoderma, fissures, pain, itch), eyes, ears, and joints. Disease severity and chronicity, patient disfigurement, and time and costs required for care impose a major burden on quality of life. This multicentre cross-sectional study investigated the impact of ARCI on quality of life of patients and families, using the Dermatology Life Quality Index (DLQI), the Children DLQI (CDLQI) and Family Burden of Ichthyosis (FBI) questionnaires. Disease severity was assessed by a dermatologist. A total of 94 patients were recruited, of whom 52 (55.3%) children. Mean age was 20.1 (median 13.5) years. The mean CDLQI/DLQI score was 7.8, and 21 patients scored >10, indicating a major impairment in quality of life: symptoms, feelings and treatment problems were the most affected domains of quality of life. FBI showed a major repercussion on psychological factors and work. The results of this study highlight the impact of ARCI on specific aspects of patient and family life, underlining the need for psychological support.
Key words: autosomal recessive congenital ichthyosis; lamellar ichthyosis; congenital ichthyosiform erythroderma; harlequin ichthyosis; Dermatology Life Quality Index; Family Burden of Ichthyosis.
Accpted May 5, 2021; Epub ahead of print May 6, 2021
Acta Derm Venereol 2021; 101: adv00477.
doi: 10.2340/00015555-3822
Corr: May El Hachem, Dermatology Unit, Bambino Gesù Children’s Hospital, Piazza Sant’Onofrio, 4, IT-00165, Rome, Italy. E-mail: may.elhachem@opbg.net
Autosomal recessive congenital ichthyoses are a group of severe and chronic genetic skin disorders. They manifest with generalized skin desquamation, thickening and redness, causing disfigurement and disability. Itch and pain are frequent. Treatment is based mainly on lifelong daily application of topical products. A multicentre Italian study was performed to evaluate disease impact on patients with autosomal recessive congenital ichthyoses and their families, using validated questionnaires. Patients’ quality of life, in particular aspects related to skin symptoms, feelings, and treatment problems, was significantly affected. Family burden particularly concerned psychological factors and work. The results can be used to improve care plans, including psychological support and therapeutic patient education.
Congenital ichthyoses are a clinically and genetically heterogeneous group of disorders of cornification (1, 2). They are more often present at birth or appear early in life, and are characterized by generalized hyperkeratosis and scaling, frequently accompanied by skin inflammation. Two types are distinguished: syndromic and non-syndromic ichthyoses. Among the latter, autosomal recessive congenital ichthyoses (ARCI) represent a major, genetically heterogeneous subgroup due to mutations in at least 10 genes (TGM1, ALOX12B, ALOXE3, ABCA12, NIPAL4, CYP4F22, PNPLA1, CERS3, SULT2B1, SDR9C7) (2). ARCI are characterized by severe and highly disabling clinical features: they manifest at birth with either a translucent membrane covering the entire body (collodion baby), or, less frequently, erythroderma and scaling (ichthyosiform erythroderma). Both presentations can be life-threatening and usually require hospitalization. Over time, patients develop whole-body skin scaling, commonly associated with palmoplantar keratoderma, and, in a proportion of cases, erythroderma. ARCI include 3 major clinical subtypes: (i) lamellar ichthyosis characterized by large, brown/dark scales and no or minimal erythema, (ii) congenital ichthyosiform erythroderma, typified by fine, white scaling with varying degrees of erythema, and (iii) the most severe, frequently early lethal, harlequin ichthyosis in which the newborn is encased in a thick “armour” and survivors develop large, lamellar scales with marked skin inflammation (1, 3). Additional ARCI features comprise recurrent infections, hypohidrosis with heat intolerance, fissures, foul-smell, pain, and pruritus (1, 3). Ocular complications include ectropion, lagophthalmos, dryness, recurrent corneal erosions and keratitis, which may lead to corneal opacities and visual impairment. Ear canal scaling is a constant feature, which can cause hearing defects and may interfere with language development in young children. Joint contractures of the extremities can develop over time and limit function. Thus, disease management requires a multidisciplinary team with periodic consultations. No curative therapy exists: available treatments are merely symptomatic and need lifelong administration. They are based on daily bathing, followed by whole-body application of topical emollients, keratolytics, and retinoids, combined in more severe cases with oral retinoids (3, 4). Overall, skin and extracutaneous manifestations profoundly alter patients’ physical appearance and affect their self-perception. These aspects, combined with disease symptoms and complications, the need for time-consuming topical treatments, and the direct and indirect costs related to global disease care, strongly affect quality of life (QoL) of the patients themselves and their families.
A few studies and 1 review (5–11) have evaluated the impact of inherited ichthyoses on QoL using general dermatological questionnaires. More recently, 2 ichthyosis-specific instruments have been proposed: the Ichthyosis Quality of Life-32 is a disease-specific questionnaire for patients (12); the Family Burden in Ichthyosis (FBI) measures the impact of the disease on family members and caregivers (13). The latter has been validated in France, and subsequently translated into Italian (14).
This Italian multicentre cross-sectional study assessed the disease impact on paediatric and adult patients affected by ARCI and their families.
Study design
This is as a multicentre cross-sectional study of patient-reported outcomes in ARCI, carried out within the framework of the European Reference Network for Rare and Undiagnosed Skin Diseases (ERN-Skin).
Study population
Patients with a clinical diagnosis of ARCI were recruited between March 2018 and June 2019 in the dermatology units of 5 Italian reference centres for inherited ichthyoses. In addition, the study design was shared with the Italian Ichthyosis Patient Association (UNITI), which collaborated by referring patients to Ospedale Pediatrico Bambino Gesù (OPBG). Consecutive outpatients or inpatients presenting with ARCI, defined by clinical features, were invited to participate. A proportion of the patients had also received molecular genetic diagnosis. Exclusion criteria were a diagnosis of a different ichthyosis form and/or refusal to provide consent to participate in the study. The study was approved by the Institutional Ethical Committee of the coordinating (OPBG) and participating centres and conducted in accordance with the Declaration of Helsinki. All participants or their legal guardians provided written informed consent before entering the study.
Study procedures
An expert dermatologist established or verified the diagnosis. The ARCI type (lamellar ichthyosis, congenital ichthyosiform erythroderma, harlequin ichthyosis) was determined based on clinical history and features, according to the ichthyosis classification definitions (1).
Outcome measures
Clinical evaluation. A standardized case-report form was used in all centres. Information was collected on patient demographics and history, family socio-economic and occupational status, frequency of disease-related consultations, consequences on school and working activities. Clinical severity was evaluated using a list of 19 signs and symptoms (e.g. ectropion, eclabion, ear deformities, etc.) (Table SI). Clinical characteristics were scored as 1 when present, and 0 if absent (total score range 0–19). Information on molecular diagnosis and mutated gene was also collected when available.
Dermatology Life Quality Index and Children’s Dermatology Life Quality Index. The DLQI and CDLQI are self-report questionnaires to measure health-related QoL over the previous week in patients with skin diseases (15, 16). The DLQI is validated for patients ≥ 16 years old; the CDLQI can be used between ages 4 and 16 years. They consist of 10 items covering symptoms and feelings, daily activities, leisure, work and school, personal relationships, and treatment. Each item is scored on a 4-point scale, with higher scores indicating a greater impact on QoL (total score range 0–30). For small children, who are unable to read or write, the parents asked the questions and registered the answers. The validated Italian versions of the 2 questionnaires were used.
Family Burden of Ichthyosis. The FBI is a 25-item self-administered questionnaire, addressing 5 domains: economic aspects, daily life, familial and personal relationships, work, and psychological impact (13). Answers are given on a 4-point Likert scale: definitely yes, sometimes, definitely not, and I do not know. Higher scores indicate a greater family burden of ichthyosis. The crude scores were transformed to a scale of 100. The questionnaire was administered to the parents of all paediatric patients and to caregivers of adult patients. The Italian version of the questionnaire, produced by our study group was used (14).
Statistical analysis
Categorical variables were described as numbers and percentages, and continuous variables as means and standard deviations (SD). Then, for each level of the variables of interest, mean (SD) and median (minimum–maximum) values of the patient-centred measures (i.e. DLQI and CDLQI, FBI) were computed. Differences were tested using the Mann–Whitney U test for 2 samples, and the Kruskal–Wallis 1-way analysis of variance (ANOVA) for 3 or more samples. The correlation between the disease severity score and patient-reported outcomes was studied using Pearson’s correlation coefficient. All analyses were performed using the statistical package IBM SPSS Statistics for Windows, Version 26.0.0.1 (IBM Corp., Armonk, NY, USA).
Age was grouped into 2 categories, i.e. 1–17 and ≥ 18 years of age. Given the different age ranges of the QoL instruments described above, possible differences in the FBI scores between children 0–3 and 4–17 years old were checked: since FBI scores in these 2 categories were very similar, to increase the power and precision of the estimates, it was decided to use only 2 age categories. The total disease severity score, based on clinical signs and symptoms, was grouped into 2 categories, i.e. 0–5 and ≥ 6; this cut-off was chosen to isolate the quintile/quartile of patients with the most symptoms/signs.
Of 102 consecutive eligible patients, 8 refused to participate. The response rate was thus 92.2%. The series included 52 paediatric patients (55.3%), the remaining ones being adults (Table SII). Mean age was 20.1 years (median 13.5 years). Paediatric patients included 4 infants, 13 children aged 1–3 years, 23 aged 4–10 years, and 12 aged 11–17 years. Adult patients comprised 23 individuals aged 18–39 years, and 19 aged ≥ 40 years. Eighty-eight out of 94 patients were Caucasian (93.6%). Most patients (n = 78, 83.0%) were affected by lamellar ichthyosis (LI), followed by congenital ichthyosiform erythroderma (CIE) (n = 14, 14.9%), and 2 children with harlequin ichthyosis (HI) (Fig. S1). Forty-eight patients (51.1%) usually underwent 1 consultation/year, 28 patients (29.8%) 2–3 times a year, and 18 (19.1%) 4 or more consultations/year. Frequent signs and complications were: palmoplantar keratoderma (n = 64, 68.1%), large scales (n = 41, 43.6%), foul-smell (n = 31, 33.0%), followed by fissures (n = 28, 29.8%), ectropion (n = 27, 28.7%), external ear deformities (n = 18, 19.1%), and recurrent infections (n = 18, 19.1%). Itching was a very frequent symptom, being present in 80 patients (85.1%), and hypohidrosis was also extremely common (n = 70, 74.5%). Molecular diagnosis was available in 49 patients (52.1%).
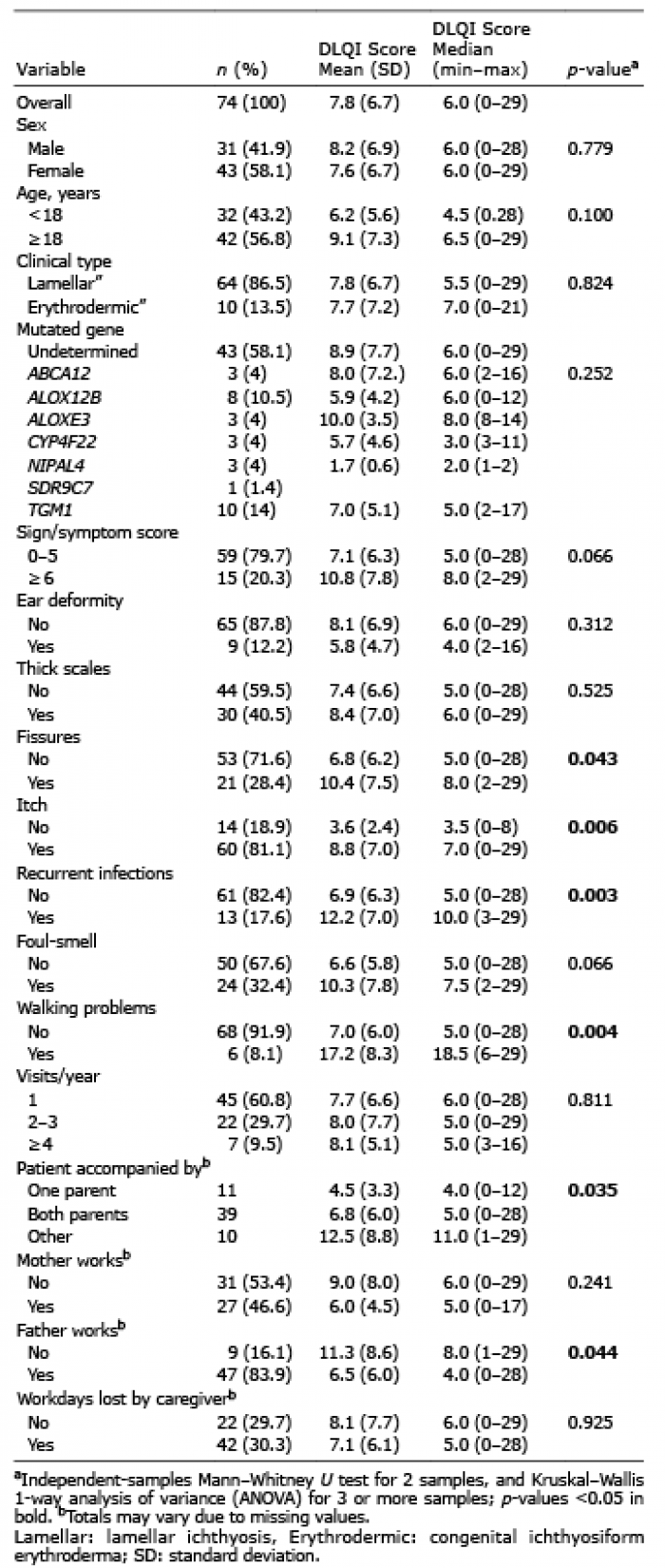
The CDLQI was administered only to patients older than 4 years, so that a total of 74 out of 94 patients (78.7%) completed the CDLQI/DLQI questionnaire. Thirty-two (43.2%) were paediatric patients and the remaining patients (n = 42, 56.8%) were adults. The majority (n = 64, 86.5%) were affected by LI, the remaining 10 had CIE (13.5%). The association between the CDLQI/DLQI score and patients’ demographics, diagnosis, clinical features, symptoms, and parents’ occupational status is detailed in Table I. The overall mean DLQI score was 7.8, and 21 participants (27.0%) scored more than 10 points, indicating a serious impairment in QoL (17). No significant differences were observed for sex and age (though adult patients had a score approximately 50% higher than paediatric patients). As for clinical signs and symptoms, the dichotomized total disease severity score was close to statistical significance (p = 0.066). However, the linear correlation between the total disease severity score and the CDLQI/DLQI, although weak (Rho 0.284), was statistically significant (p = 0.014). Interestingly, different single signs or symptoms were significantly associated with higher DLQI scores, i.e. fissures, itch, recurrent infections, and walking problems due to limb flexion contractures. Ten adult patients not accompanied by parents, but by other caregivers, had worse QoL. Also of note, although only 9 patients had an unemployed father, they had significantly higher DLQI scores.
Table I. Association between clinical features and (Children) Dermatology Life Quality Index (C)DLQI
When looking at the single DLQI items (Fig. 1), significantly higher scores were observed for items 1 (symptoms such as itch and pain), 2 (embarrassment and self-consciousness), 4 (problems with clothing choice), and 10 (problems caused by treatment).
Fig. 1. Mean, and 95% confidence intervals (CI), for the Dermatology Life Quality Index (DLQI) questionnaire single-item scores.
Table II summarizes the associations between the main variables of interest and the FBI total score. Sixty-five caregivers of the 94 patients (69.1%) completed the FBI questionnaire. Specific to paediatric patients, almost all parents/guardians completed the FBI (i.e. 51 of 52). The mean score for the whole sample was 48.4 (median 48.0). When considering the total FBI score generated by the 25 items, a greater family burden was observed for patients with lamellar or harlequin ichthyosis (p = 0.002), for patients with a higher total disease severity score (close to statistical significance, p = 0.070), and for patients with thick scales, fissures, or foul smell. It should be noted, though, that the linear correlation between the total disease severity score and the FBI, although moderate (Rho 0.356), was statistically significant (p = 0.004). In addition, FBI scores were significantly higher for family members of patients who required ≥ 4 visits per year.
Table II. Association between clinical features and Family Burden of Ichthyosis (FBI)
The FBI scale scores are shown in Fig. 2A: the highest score was observed for the Psychological Impact scale, followed by the Work scale. The study compared the scale scores in caregivers of patients with LI vs CIE, and observed significant differences for all the scales except the Economic scale (Fig. 2B).
Fig. 2. (A) Means and 95% confidence intervals (95% CI), for the scores of the 5 scales of the Family Burden of Ichthyosis (FBI) questionnaire. (B) Mean and 95% CI for the scores of the 5 scales of the FBI questionnaire, by clinical diagnosis (lamellar: lamellar ichthyosis; erythrodermic: congenital ichthyosiform erythroderma).
This study evaluates, for the first time, disease burden and QoL in patients with ARCI and their families. The predominance of paediatric patients vs adult ones in our series might be ascribed to the progressive loss-to-follow-up with age (18). The extremely high response rate (92.2%) was probably due to direct administration of the questionnaires during hospital consultations. Indeed, previous studies on QoL in inherited ichthyoses were based on postal or online surveys, and achieved significantly lower response rates (5–9). The mean and median DLQI scores (7.8 and 6.0, respectively) in the current patients are consistent with values obtained in previous studies conducted on French, American, and Swedish patients, although the study populations are not directly comparable due to the different ichthyosis types (5–9, 19). The trend towards a worse QoL in adults vs children has also been reported in patients with ichthyosis (7). This might be related to increasing difficulty in coping with a chronic, lifelong disease, but also to shifting of follow-up towards the more severe cases over time. The correlation between total disease severity and DLQI score was modest, but statistically significant, confirming the findings seen in other chronic skin conditions when clinical severity indexes are considered together with patient-reported outcomes (20). This suggests that, in addition to the extent of clinical involvement, personal experience and feelings also affect disease impact. Previous studies detected a greater correlation between DLQI score and disease severity, which, however, was evaluated by the patients/caregivers themselves (7, 8), while, in the current study, the dermatologist examined the patients and independently assigned disease scores. On the other hand, specific signs and symptoms were meaningfully associated with a higher DLQI. In particular, itch was present in > 80% of our patients and strongly associated with a worse QoL, in line with literature data (6, 8, 9) and with a recent study evaluating itch in patients with ichthyosis (21). Indeed, in the current study, the highest single-item DLQI score was obtained for the presence of itch, stinging and pain. In this regard, fissures were also significantly associated with a higher DLQI score. Fissures are painful, chronic, and require an adapted treatment with increased complexity of care (22). The current findings point to the need for improved management in this often neglected, but relatively common (29.8% in our series), complication of ichthyosis. Although recurrent cutaneous infections are seen in only a minority of patients with ARCI, they greatly affect QoL, due to increased itching and pain, modified care plan, including additional dermatological visits. Functional damage, in particular walking problems, were present in a small number of severely affected patients with ARCI, who had a mean DLQI score of 17.2, corresponding to a very large effect on QoL (17).
The worse QoL in patients with ARCI with unemployed fathers might be related to decreased income, with consequent difficulty affording the costs of disease management. Although the Italian Health System should cover ichthyosis care costs, there are major variations on a regional basis, in particular for reimbursement of detergents, emollients, and travel for medical reasons. Furthermore, ichthyosis requires substantial additional indirect expenses for home management (e.g. cleaning, clothing), resulting in extra financial burden for families. Consistent with this last observation, when examining the DLQI profile score, the highest value following symptoms corresponded with problems related to treatment. This is not surprising, considering that almost all patients need daily topical skin care (e.g. bathing, keratolytics, and emollients), which is stressful and time-consuming, particularly in children. In addition, scaling and malodorous skin requires frequent changes of clothing and bed linen. Indeed, the items with next highest score were problems with clothing choice, and skin-related embarrassment. These data are in keeping with previous studies on QoL in ichthyoses (6, 8, 9).
To date, family burden in ichthyoses has been evaluated in a single French study, which developed and validated a disease-specific questionnaire, the FBI (13). Recently, we have translated and validated the Italian version, which was administered to the patients in the current study (14). The total FBI score significantly correlated with disease severity in the current study, in agreement with the original French one (13). The mean FBI score of the current study population was 48.4, with the highest value for the psychological dimension. Although absolute scores were lower in our patients than in the original French study, the FBI psychological impact was the most important determinant of disease burden in both studies. It is notable that family disease burden was considerably higher in our patients with LI, compared with those with CIE. This finding may be related to the significantly higher FBI score obtained in patients with thick scales and smelly skin, typical of LI. Moreover, the most affected dimension after the psychological one in LI was the disease impact on caregiver work, possibly reflecting the engagement and time needed for daily management in this severe and disfiguring ichthyosis subtype. In addition, the need for frequent hospital visits (≥ 4/year) correlated positively with a higher FBI score. Finally, the familial relationship dimension was significantly affected in both CIE and LI, in line with the major impact of all ARCI subtypes on the whole family and on the relationship between the parents, planning of leisure activities, holidays, visits to friends and relatives, etc. (10).
A limitation of the current study is that molecular diagnosis was available for only a proportion of the patients. Nevertheless, ARCI diagnosis remains primarily clinical and was confirmed by expert dermatologists in reference centres for ichthyoses.
In conclusion, this study confirms the major burden that ARCI imposes on QoL of patients and caregivers, further highlighting the need for improved and integrated care protocols, while waiting for new treatments to become available. More specifically, these results emphasize the need to offer psychological support to both patients and family members aimed at reducing disease burden and improving QoL. A primary role is obviously played by the psychologist, but other multidisciplinary team members, in particular dermatologists, dedicated nurses, and social workers, should also actively participate. From this perspective, the patient’s care plan for ichthyosis should include educational programmes also taking into account patient and family disease burden, as well as information about patient support groups. Finally, these findings could be relevant in guiding the choice of outcome measures in future observational clinical studies and randomized controlled trials.
We thank the patients, their families, and the Italian Ichthyosis Patient Association (UNITI) for constant and constructive collaboration. We are grateful to Mr Gabriele Bacile for iconography preparation and Mrs Lavinia Serra for secretarial assistance. DA, RR, AD, SG, IN, AV, DC, GZ, CB, and MEH are members of the European Reference Network ERN-Skin. DA, DC, and GZ are supported, in part, by the “Progetto Ricerca Corrente 2020” of the Italian Ministry of Health, Rome, Italy.


 Click to show fullsize
Click to show fullsize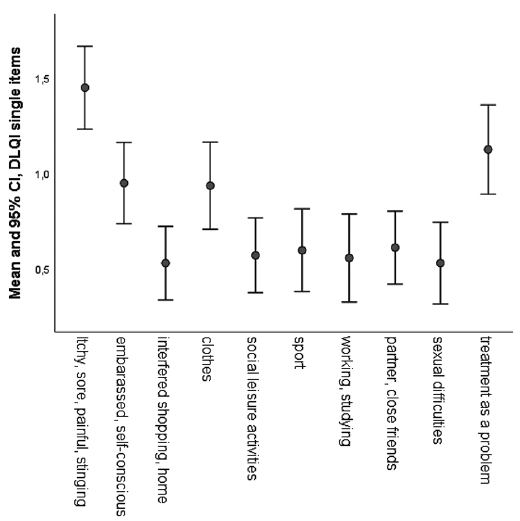 Click to show fullsize
Click to show fullsize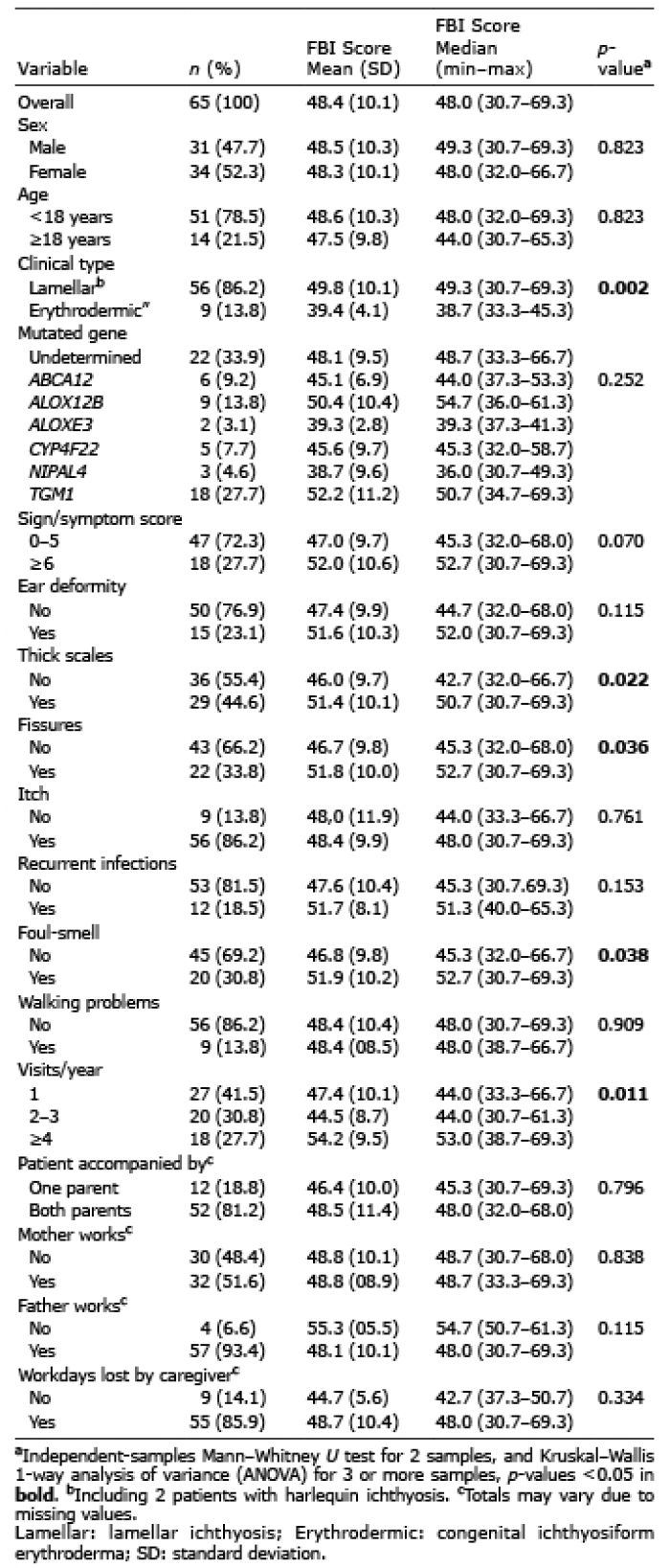 Click to show fullsize
Click to show fullsize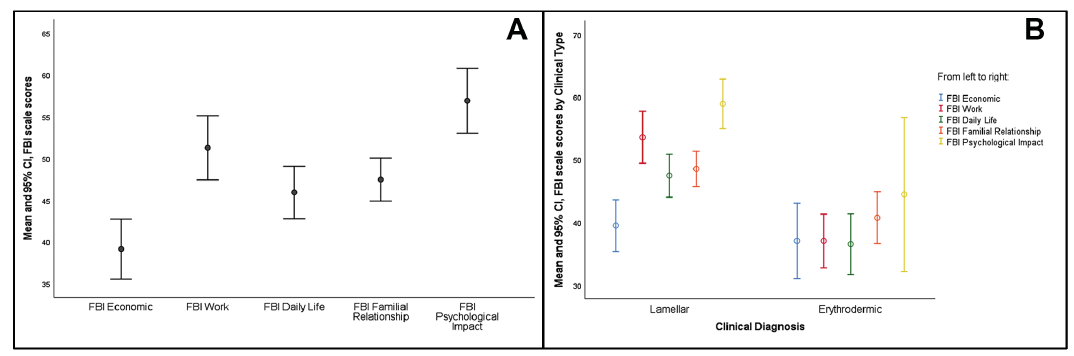 Click to show fullsize
Click to show fullsize