


1China Medical University, 2Department of Dermatology, The First Hospital of China Medical University, NHC Key Laboratory of Immunodermatology, Key Laboratory of Immunodermatology, Ministry of Education, Shenyang, China, 3Department of Dermatology, University of California-San Diego, San Diego, CA, USA, and 4National Joint Engineering Research Center for Diagnosis and Treatment of Immunologic Skin Diseases, Shenyang, China
#These authors contributed equally to this work
Balanoposthitis is a common inflammatory condition of male genitalia, while the overall microbiota spectrum and its relevance to contributing factors have yet to be determined. This case-control study included patients with balanoposthitis (n = 26) and matched healthy controls (n = 29), both uncircumcised. Overt fungal infection in balanoposthitis was excluded, swab samples were collected, 16S rRNA gene sequenced and analysed. The profile of the microbiome was further analysed in relation to the clinical severity of the disease and the physical barrier status of the glans penis, including mucosa pH, transepidermal water loss, and mucosa hydration. In general, the microbiota composition was similar between patients with balanoposthitis and healthy controls, while it was different between patients with balanoposthitis and healthy controls with redundant prepuce. Decreased hydration of the mucosa and increased pH were found in patients with balanoposthitis. Staphylococcus warneri and Prevotella bivia are the 2 most abundant balanoposthitis-associated species and are positively correlated with disease severity.
Key words: balanoposthitis; microbiome; male genital mucosa physical barrier; redundant prepuce.
Accepted May 19, 2021; Epub ahead of print May 24, 2021
Acta Derm Venereol 2021; 101: adv00466.
doi: 10.2340/00015555-3833
Corr: Li Zhang and Xing-Hua Gao, Department of Dermatology, The First Hospital of China Medical University, 155N Nanjing Street, Heping District, Shenyang 110001, China. E-mail: lizhang_1001@126.com; gaobarry@hotmail.com
Balanoposthitis is a common inflammatory condition, affecting approximately 6% of uncircumcised males. The overall microbiota spectrum and its relevance to contributing factors for this condition have yet to be determined. This study found that balanoposthitis was associated with an impaired male genital mucosa physical barrier and a higher colonization rate of Staphylococcus warneri and Prevotella bivia. A possible treatment regimen for balanoposthitis may therefore include restoration of the genital mucosa barrier and of the balance of the indigenous microbial population.
Balanoposthitis represents one of a group of the most common male genital inflammatory diseases. Inflammation involving the glans penis is termed balanitis, that involving the prepuce is termed posthitis, and that involving both areas is termed balanoposthitis (BP) (1). BP is thought to be caused by, or associated with, a range of disorders, such as infection, inflammatory dermatosis, tumours, trauma, autoimmune diseases, and drug eruptions (2). In addition to the contribution of Candida albicans, bacterial colonization, such as Staphylococcus aureus, group B streptococci (GBS), and group D streptococci (GDS) (3, 4), as well as anaerobic strains (5), are considered pathogenic in BP, based on conventional culture-based methods. Recent studies have revealed that the composition of the bacterial community of the penile mucosa is quite diverse, and can be influenced by circumcision (6) and by the vaginal status of monogamous sex partners (7). For example, there is a significant decrease in putative anaerobic bacterial families after circumcision, notably the Clostridiales and Prevotellaceae families (6, 8, 9). It has been reported that the incidence of balanitis is 4% in children (10), 11–13% in adults without circumcision, and 2% in adults with circumcision (11).
The microbiota profile in BP is yet to be established. This case-controlled study investigated the diversity of the male genital mucosa microbiome in patients with BP, by targeting region V4 of 16S ribosomal RNA (rRNA), and evaluated the correlation between genital mucosa microbiota and the clinical features of BP.
Study participants
Clinical materials were collected at the Department of Dermatology, the First Hospital of China Medical University, China, over the period 1 July to 1 November 2018. This study was approved by the ethics committee of the First Hospital of China Medical University, Shenyang, China (Chinese Clinical Trial Registry, Number: ChiCTR1800016901).
Inclusion and exclusion criteria
Patients were in the age range 18–65 years. According to the 2013 European guideline for the management of BP led by International Union against Sexually Transmitted Infections (2), clinical diagnosis of BP was given as inflammatory lesions involving the glans penis and prepuce (1), manifesting as ill-defined oedematous erythematous patches, erosions, papules, and excessive smegma, with or without a foul odour, soreness, or itching. Written informed consent was obtained from the patients. Exclusion criteria were: patients who received systemic antibiotics and antifungal drugs, or topical use of agents containing antibiotics, antifungal, glucocorticoids over the glans penis within one month prior to enrolment in the study; those with severe unmanageable systemic conditions, such as chronic hepatic or renal failure, ill-managed hypertension and diabetes, organ transplant recipient, type I allergic condition with sustained use of drugs; those with other defined genital diseases within 3 months, including, but not limited to, warts, psoriasis, lichens sclerosus; and those with overt candidal infection with positive KOH (potassium hydroxide) microscopic detection showing pseudohyphae or germinative spores. Healthy controls (HC) were volunteers who met the following criteria: age 18–65 years; generally healthy and no ill conditions at the site of the glans penis; who understand the content and nature of the study; and signed the consent form.
At the deadline for clinical recruitment, 30 BP were screened, among them, 4 were excluded due to positive microscopic fungal detection. Of the 30 HC screened, one was excluded due to self-report indisposed condition. In total, 26 patients diagnosed with BP and 29 HC consecutively entered the study. Redundant prepuce was defined as foreskin exceeding the middle point between the tip of glans penis and coronal sulcus, or longer (12).
Sampling for microbiome detection, clinical assessment and, measurement of physical barrier parameters
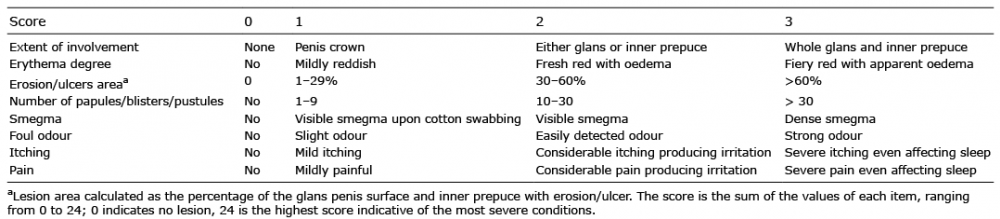
HC and patients with BP were asked to clean their genital area with water, the night before the day of their appointment. Participants were instructed to retract and flatten the foreskin. The glans penis and prepuce were scrubbed with a sterile cotton swab moistened with normal saline. Samples were placed in sealed sterile containers, transported to the laboratory, and stored at –80°C. At 30 min after sampling, 2 dermatologists graded symptom severity according to a 4-grade score (0–3 points) and arrived at a consensus. Items included within this severity score scale included erythema, oedema, erosions/ulcers, papules/blisters/pustules, smegma, itching, pain, and foul odour (Table I). The major clinical signs and symptoms were ranked and scored; the scores ranged from 0 to 24 (Table I). Physical barrier properties of the ventral surface of the glans penis, including male genital mucosa pH, trans-epidermal water loss (TEWL), and hydration content, were measured using the Courage + Khazaka electronic GmbH MPA 10 (Courage Khazaka, Version: 2.3.4.1/2017/2/1; Courage + Khazaka electronic GmbH, Köln, Germany) as instructed by the manual, under normal climatic conditions (20° C, 40–60% air humidity). Measurement for each site was repeated 3 times.
Table I. Severity scores of patients with balanoposthitis
DNA extraction and sequence processing
Total genomic DNA was extracted by using the CTAB (hexadecyltrimethylammonium bromide) method. The V4 region of the 16S rRNA was amplified by polymerase chain reaction using primers 515F/806R as described (13, 14). Amplicons were sequenced on a desktop sequencer (Ion S5 XL, Thermo Scientific, Waltham, MA, USA). Soft Cutadapt was used to filter low abundance reads and short read lengths, while operational taxonomic units (OTUs) were clustered and annotated based on a ≥ 97% nucleotide sequence identity. Rarefaction was performed for further analysis. The genital mucosa microbiota was characterized based on the Silva132 Database (Max Planck Institute for Marine Microbiology and Jacobs University, Bremen, Germany).
Statistical analysis
Statistical analysis and graphic visualizations were performed using soft R (version 3.5.2). Differences in male genital mucosa physical barrier function items between the groups were compared using Student’s t-test. the observed species (number of taxa at species level) and the Shannon Wiener index (combining richness and evenness of microbiota) (15) were calculated with use of the phyloseq package on raw data for alpha diversity (individual-sample microbiota diversity) (16), and statistically tested using the Wilcoxon rank-sum test, the correlation between alpha diversity and Severity Scores was analysed using linear regression. For beta diversity (between-sample microbial compositions) (16), community structure differences between the groups were visualized with principal coordinate analysis (PCoA) plots based on weighted unifrac distances, tested by Multi Response Permutation Procedure (MRPP) based on Bray-Curtis dissimilarity index. Linear discriminant analysis effect size (LEfSe) was used to determine whether a particular OTUs abundance was statistically different between groups, linear discriminant analysis (LDA)>4 were chosen to show in the LEfSe. Random Forest (R packages “randomForest”) was used to analyse the associations between the top 35 OTUs and severity scores, and male genital mucosa physical barrier. The level of statistical significance was set at α=0.05.
Clinical features of participants
Demographic data from all participants were summarized in Table II, BP and HC cohorts were comparable concerning age, having sexual activity, cleansing frequencies, and body mass index (BMI) (all p > 0.05), all participants were uncircumcised. There were more participants with redundant prepuce in patients with BP than in HCs (25/26 vs 20/29, p < 0.05). Patients with BP had higher rates of history of STIs (10/26 vs 0/29, p < 0.05) and condom use (8/17 vs 2/17, p < 0.05) during sexual intercourse than the HCs. The 26 patients were scored with a mean score of 7.08.
Table II. General characteristics and male genital mucosa physio-barrier status of participants
Microbial distribution of balanoposthitis and healthy controls
A total of 4,429,670 paired-end reads were obtained from all samples. After sequence assembly, quality filtering, and chimera removal, a dataset of 4,192,347 high-quality, classifiable 16S rRNA gene sequences, with a mean of 76,224 sequences per sample, were obtained. OTUs (n = 8,963) were annotated with taxonomic information related to 63 bacterial phyla, 81 classes, 179 orders, 347 families, 1,054 genera, and 919 species. The most dominant phyla in both groups were Actinobacteria, Proteobacteria, Firmicutes, and Bacteroidetes. The top 10 genera with the greatest relative abundance in both groups were Finegoldia, Stenotrophomonas, Lactobacillus, unidentified Corynebacteriaceae, unidentified Prevotellaceae, Porphyromonas, Prevotella, Ezakiella, Dialister, and Staphylococcus.
Inter- and intra-group differences in genital mucosa microbiome between balanoposthitis and healthy controls
There were no statistically significant differences in alpha diversity between the BP and HC groups (p > 0.05), by community richness index (the observed species) and diversity index (the Shannon Wiener index) analysis, albeit species diversity levels within 43 out of 55 samples were high (mean of Shannon indexes were > 4). The observed species were inversely correlated with disease severity scores in BP (p < 0.05), i.e. a smaller number of taxa at species level was found in patients with higher severity scoring. The richness and evenness of microbiota (Shannon indexes) was not correlated with disease severity (p > 0.05).
Next, the microbiome composition (beta diversity) was analysed by MRPP and displayed by PCoA. The differences in microbiome composition between the BP and HC groups were not significant (p 0.11 > 0.05, MRPP). All but one of the BP had redundant prepuce, while 9 HC had normal prepuce (HCNP) and 20 HC had redundant prepuce (HCRP). Beta diversity was statistically different between HCNP and HCRP, BP and HCRP (all p < 0.05), but there was no statistical difference between BP and HCNP (p > 0.05) (see Fig. 1). These results suggest that both redundant prepuce and inflammation might affect male genital mucosa microbiome composition. Again, there were no statistically significant differences in the Shannon index and observed species among the BP, HCNP and HCRP groups.
Fig. 1. Principal coordinate analysis (PCoA) plots of microbiota among 3 groups. PCoA plots based on weighted unifrac distances. The x- and y-axes of PCoA indicate the first and second coordinates, respectively. BP-HCNP-HCRP (HCNP-HCRP, p < 0.05; BP-HCRP, p < 0.05, BP-HCNP, p > 0.05; MRPP). BP: balanoposthitis; HCRP: healthy controls with redundant prepuce; HCNP: healthy controls with normal prepuce.
Male genital mucosa physical barrier function of participants
In general, low TEWL, high skin hydrational state, and low pH reflect the well physical barrier properties of the skin (17). When the length of the prepuce was counted, subjects with HCRP had significantly increased TEWL and water content, compared with HCNP, while the pH remained similar. The pH of BP (mean difference (95% CI): 6.34 (6.01–6.66)) was higher than that of HCNP (mean difference (95% CI): 5.71 (5.44–5.97)) and HCRP (mean difference (95% CI): 5.71 (5.52–5.89)). BP was more alkaline than that of HC and exceeded the normal range of 4.1–5.8 (18). The hydration content was significantly decreased in BP compared with HCRP.
Staphylococcus warneri and Prevotella bivia are 2 balanoposthitis-associated species
To determine different OTUs among groups. Staphylococcus warneri and Prevotella bivia were identified as 2 major species in the BP group compared with HC group (Fig. 2, upper panel). When compared with HCNP and HCRP groups, again, Staphylococcus warneri and Prevotella bivia were the major species in BP (Fig. 2, lower panel). Prevotella bivia was abundant in BP without sexual activity (LDA 4.492, p < 0.05), Staphylococcus warneri was abundant in BP with condom use (LDA 4.420, p < 0.05). genus Ezakiella was enriched in the HCRP group, species Porphyromonas somerae was enriched in the HCNP group.
Fig. 2. Linear discriminant analysis effect size (LEfSe) analysis of significantly different operational taxonomic units (OTUs) between groups. OTUs with significant differences among groups are shown, results with linear discriminant analysis (LDA) > 4 were selected. Taxonomic levels are represented with prefix p_: phylum, c_: class, o_: order, f_: family, g_: genus, s_: species. BP: balanoposthitis; HCRP: healthy controls with redundant prepuce; HCNP: healthy controls with normal prepuce.
Relationship between the microbiome and severity of balanoposthitis, and male genital mucosa physical barrier function
The abundant OTUs defined by the sum number of per sample reads that exceeded 10,000 (uniform treatment to 40,289 reads per sample) were selected. The top 35 abundant OTUs from the 8,963 OTUs were selected. The correlation between the microbial composition of the top 35 OTUs and severity scores was analysed by using the Gini index of Random Forest. The abundance of OTUs served as the independent variable, while severity score represented the value of each sample as continuous dependent variables. The current study found that the species Prevotella bivia, Staphylococcus warneri, and genus Phyllobacterium were prevalent in cases with higher severity scores (Fig. 3).
Fig. 3. MeanDecreaseGini index of 35 operational taxonomic units (OTUs) and severity scores. Gini index of OTUs using Random Forest to analyse associations between the 35 abundant OTUs and severity scores. The larger value of MeanDecreaseGini, the greater the importance of the OTUs for balanoposthitis (BP) or healthy controls (HC). Taxonomic levels are represented with prefix f_: family, g_: genus, s_: species.
The same method was used to analyse the correlation between microbiota and male genital mucosa physical barrier function, genus Phyllobacterium, genus Dialister, species Prevotella corporis, genus unidentified Cyanobacteria, and genus unidentified Corynebacteriaceae were the first 5 OTUs related to high pH; genus Stenotrophomonas, species Bacteroides fragilis, genus Stenotrophomonas.1, species Corynebacterium tuberculostearicum, and species Enterococcus durans were the first 5 OTUs related to high TEWL; genus Phyllobacterium, genus Ezakiella, species Negativicoccus succinicivorans, genus unidentified Corynebacteriaceae and species Bacteroides fragilis were the first 5 OTUs related to high male genital mucosa hydration (data not shown).
BP is a common inflammatory male genital mucosa disease that mostly affects uncircumcised males. The diagnostic criteria for this relatively common condition remain vague and depend mainly on clinical manifestations and exclusion of sexually transmitted diseases, along with specific inflammatory and neoplastic male genital mucosa diseases. The main purpose of the histopathological examination is to confirm the special type of balanoposthitis, such as circinate balanitis and plasma cell balanitis, and to exclude pre-malignant conditions (2). When accompanied by persistent erythematous lesions involving the balanopreputial sac in uncircumcised patients, infiltration of lymphocytes, histiocytes, and plasma cells can be seen in the upper part of the chorion (19).
The male genital mucosa microbiome can be influenced by physical barrier integrity, inflammation, antimicrobial peptides, and even lipids, as reported in atopic dermatitis (20, 21). One recent study about male genital lichen sclerosus found that Fusobacterium spp. was enriched in the microbiota of balanopreputial sac and urine (22), the most common bacteria present in their healthy controls, such as Finegoldia, Corynebacterium, Prevotella, and Dialister, were also found in this study, which mean these genera have adapted themselves to healthy host-microbe cross-talk and local genital microenvironment. The mucosa of the prepuce and glans penis have fewer similarities to other parts of the skin, except that there was no hair follicle or eccrine sweat gland exist on the glans penis, penis crown, and preputial mucosa (23). The BP enrolled in the current study showed a higher rate of redundant prepuce (all of the 26 cases except for one, this is a limitation of this study as there are fewer patients with a normal prepuce), higher incidences of STIs, and tended to use a condom during sexual behaviour. Some bacteria were influenced by lifestyle, for example, Staphylococcus warneri was abundant in BP with condom use, Prevotella bivia was abundant in BP without sexual activity (LDA 4.492, p < 0.05).
This study profiled the bacterial diversity and richness in BP by using a high throughput 16s rRNA sequencing and to compare the physical barrier status between BP and HC, and score their inflammation severity by designing a scoring algorithm for BP. Irritation to genital mucosa and washing with soap predispose the recurrence of BP (24). We presume dysbiosis and damaged physical barrier are additional causal factors to BPs, except those with overt fungal infection. To the best of our knowledge, this is the first report to assess the male genital mucosa microbiome regarding BP and genital mucosa physical barrier in the glans penis.
Regarding physical barrier status, it was found that HCRP had increased TEWL and genital mucosa hydration, which maintained a higher level of water content and exudation compared with HCNP. Considering that redundant prepuce is one of the leading clinical causes of BP, the hyperhydration of skin might not only disrupt the ultrastructure of the stratum corneum by forming intercellular pools of water (25), but might also support the growth of adherent microbes. The current study found that there was no difference in pH between healthy subjects with or without redundant prepuce. BP had increased pH and decreased male genital mucosa hydration compared with HCRP. The high pH value in BP may favour the growth of certain bacteria, such as that of the optimal pH of 7.5 for Staphylococcus aureus (18). It has been reported that cutaneous pH is influenced by filaggrin degradation, fatty acid content, sodium-hydrogen exchanger activation, and melanosome release (18).
No significant differences in alpha or beta diversity were found between BP and HC, in general. The current study confirmed the previous finding that there was a significant difference in beta diversity between HCNP and HCRP, suggesting that the prepuce could not be a neglected niche for the local anatomical environment (9). Noting that there was a significant difference in beta diversity between BP and HCRP, we postulate that inflammatory status can influence the beta diversity under the same circumstances. Beta diversity was not statistically different between BP and HCNP (p > 0.05), patients with BP and HCNP had similar hydration levels of the genital mucosa (Table II), which may be favourable for the similar beta diversity. Specifically, it was found that the observed species decreased with higher severity scores of BP, similar findings were reported in atopic dermatitis, that Eczema Area and Severity Index (EASI) score correlated negatively with the observed species (26).
Using LEfSe analysis, this study found that Staphylococcus warneri and Prevotella bivia were 2 balanoposthitis-associated species, which were more abundant in patients with high disease severity. Staphylococcus warneri, a coagulase-negative pathogen, can adhere and invade human epithelial cells by forming biofilm via ica-independent mechanisms, and to destroy cells by extracellular toxins (27). Prevotella bivia was reported as a cause of bacterial vaginosis, through its capacity to alter barrier properties and induction of epithelial cell activation in the vagina (28). We postulated that Prevotella bivia is pathogenic to BP. As genus Prevotella could be found in the urethra and bladder (29), retrogradation of Prevotella bivia in BP could not be ignored. Adjusting the pH to normal range, applying moisturizing cream may help restoring the barrier integrity. In addition to direct suppression of the overgrowth of the above-mentioned microbes in BP by applying antibiotics, probiotics as exemplified by Lactobacillus may suppress the growth of Prevotella bivia (30).
The current study has some limitations. The number of patients and HC enrolled were small, and the BP with normal prepuce should be included in the future studies. Albeit KOH microscopic detection of pseudohyphae or germinative spores is a common practice, the sensitivity and specificity of the test, as reported, were 66% and 98%, respectively (31); thus there is a possibility that a small number of patients with candidal BP be neglected. We could not rule out the possibility that the previous history of STIs confounded the onset and development of BP. We did not perform bacterial culture test for the enrolled cases. The V3 or V3V4 region of the 16S rRNA is preferable to V4 region applied in the present study (32), as V4 is considered a relatively low informative region for taxonomic assignment, which may poorly capture skin commensal microbiota and downstream results.
In summary, this study found that the microbiome in BP could be associated with clinical symptoms, foreskin length, physical barrier status, and behavioural factors. Staphylococcus warneri and Prevotella bivia emerged predominantly in BP, and its pathogenic role remains undetermined.
The authors thank Professor Mao-qiang Man of Dermatology, VAMC San Francisco, Northern California Institute for Research and Education, and Professor Yu-ping Lai of School of Life Science, East China Normal University for their critical revision of this manuscript.
This work was supported by the National Natural Science Foundation of China (grant number 81673070), the 111 Project of Ministry of Education of the People’s Republic of China (D18011), and the program of the Liaoning Education Bureau (number FWZR2020007).


 Click to show fullsize
Click to show fullsize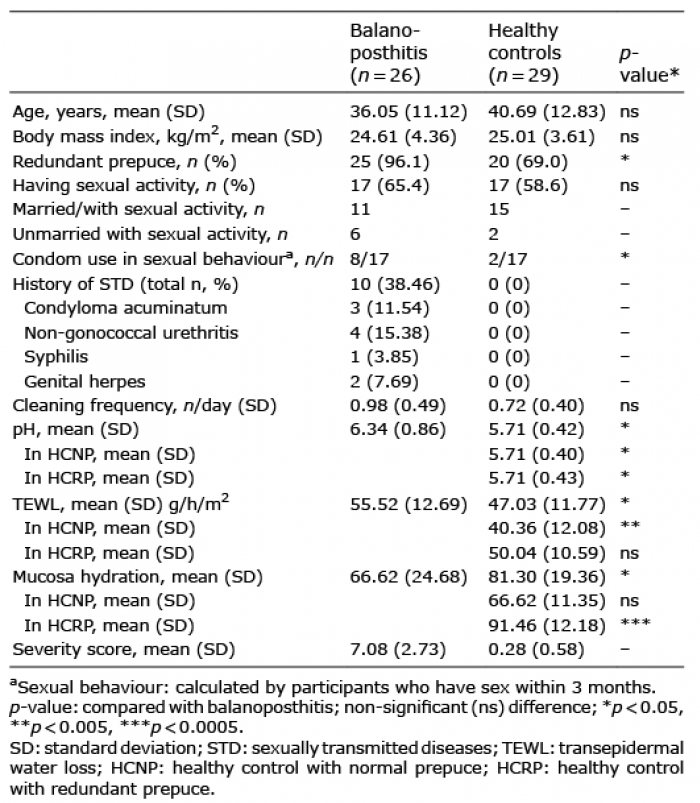 Click to show fullsize
Click to show fullsize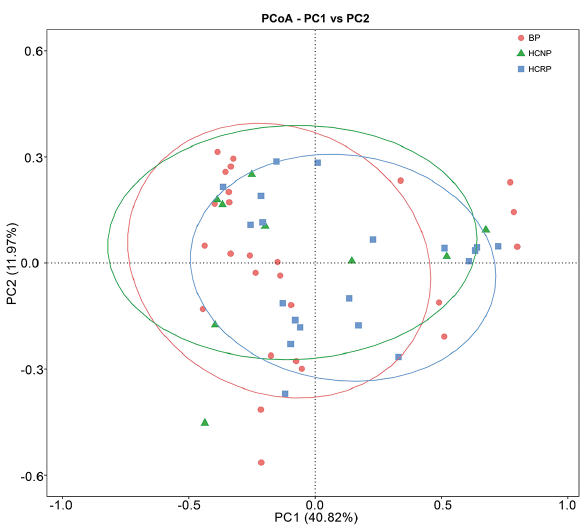 Click to show fullsize
Click to show fullsize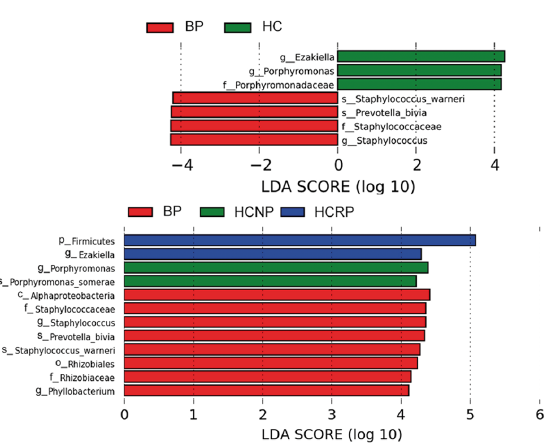 Click to show fullsize
Click to show fullsize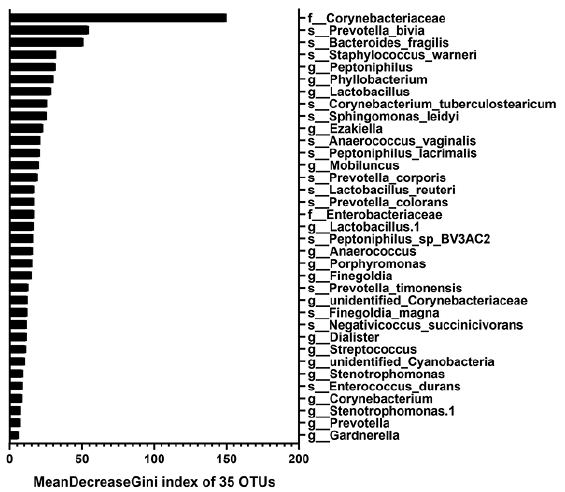 Click to show fullsize
Click to show fullsize