


1Department of Dermatology, Xiangya Hospital, Central South University, 2National Clinical Research Center for Geriatric Disorders as well as Key Laboratory of the Biology of Aging of Hunan Province, Xiangya Hospital, Central South University and 3Key Laboratory of Organ Injury, Aging and Regenerative Medicine of Hunan Province, Changsha, China
#These authors contributed equally and should be considered as first authors.
The exact mechanisms of rosacea development are unknown, but it has been suggested that tea consumption may be associated with its development. To determine the relationship between tea drinking behaviour and rosacea, this clinical case-control study recruited 2,063 participants, who completed a questionnaire about tea drinking behaviour. A 1:1 ratio propensity score matching method was used to generate 619 cases and 619 controls. High-frequency tea drinking (3 times/day: adjusted odds ratio (aOR) 2.592; 95% confidence interval (95% CI) 1.225–5.485; ≥ 4 times/day; aOR 8.86; 95% CI 3.43–22.887), non-fermented tea (aOR 2.172; 95% CI 1.562–3.022), and hot tea (aOR 2.793; 95% CI 1.796–1.344) were associated with an increased risk of rosacea. Further results showed that these tea drinking behaviours were significantly associated with an increased risk of flushing (aOR 1.41; 95% CI 1.07–1.87) and erythema (aOR 1.48; 95% CI 1.10–2.00). Tea drinking behaviour is closely related to rosacea and mainly affect flushing and erythema.
Key words: rosacea; tea drinking; inflammatory skin disease; case-control study.
Accepted Jun 21, 2021; Epub ahead of print Jun 23, 2021
Acta Derm Venereol 2021; 101: adv00488.
doi: 10.2340/00015555-3849
Corr: Ji Li and Yalin Wang, Department of Dermatology, Xiangya Hospital, Central South University, Xiangya Road, Kaifu District, Changsha, Hunan 410008, China. E-mail: liji_xy@csu.edu.cn, 1561821680@qq.com
Tea is a very popular drink among the Chinese population, but the relationship between tea consumption and rosacea remains unclear. This clinical case-control study selected a propensity score matched population of 619 cases and 619 controls by matching demographic characteristics. The type of tea consumed (non-fermented tea), frequency of tea consumption per day (≥3 times/day), and drinking temperature (hot tea) were related to rosacea. Tea drinking behaviour was found to be closely related to rosacea and mainly affected flushing and erythema. Therefore, we recommend that patients with rosacea should reduce the frequency of tea drinking per day, particularly hot tea, but can continue their tea drinking habits in the long term.
Rosacea is a chronic inflammatory skin disease that predominantly affects middle-aged women (1–3). According to previous investigations, 5.46% of adults worldwide are affected by rosacea, the prevalence of rosacea in China being 3.48% (2, 4). Many studies have shown rosacea to be a disease involving multiple factors, including skin immunity, microbiota, neurogenic dysregulation, genetics, and damaged skin barrier (5, 6). However, to date, the exact mechanisms responsible for development of rosacea are unclear.
In addition, numerous factors have been found to trigger rosacea, including spicy foods, certain beverages, sunlight, stress, strenuous exercise, certain skin care habits, and sleep quality (1, 6–9). Recent studies have shown that dietary changes may play a significant role in the prevention of rosacea. To date, studies on rosacea and dietary factors have focused mainly on coffee and alcohol. Li et al. (10, 11) found that alcohol intake was associated with the risk of rosacea in women, while increased intake of caffeine from coffee was found to reduce the risk of rosacea. Globally, tea and coffee are the most popular drinks after water (12). It is well-known that China has a long history of tea drinking, and tea is a very popular drink among the Chinese population (13). An increasing number of epidemiological studies have demonstrated the associations between tea consumption and various diseases, such as diabetes (13), coronary heart disease (CHD) (14), and certain cancers (15). Tea can be divided into 2 types, non-fermented tea (green tea) and fermented tea (black tea, white tea, dark tea, oolong tea, and yellow tea), based on their respective processing methods; the polyphenol content in the 2 types of tea is different (16). Some studies have shown that polyphenols and caffeine in tea provide antioxidative, immunomodulatory, and anti-inflammatory effects, which may be beneficial for the treatment of rosacea symptoms (17–21). However, there is currently no research that concludes whether these different types of tea have varying effects on rosacea development. Meanwhile, heat and hot beverages have also proven to be triggers for rosacea (22, 23). Tea is usually consumed when hot, but whether the drinking temperature of tea affects rosacea development is unknown. Furthermore, many of these studies have indicated that the frequency of tea consumption has different effects on different diseases (7, 24, 25). However, there is a general lack of research on the relationship between tea consumption and rosacea, and the existing evidence remains inconclusive regarding whether tea drinking behaviours affect rosacea.
The aim of this study is to explore the relationship between rosacea and tea drinking behaviour, by investigating a total of 2,063 participants from China, and to provide rosacea patients with guidance on tea drinking behaviour.
Study design and population
This was a clinic-based case-control study performed at Xiangya Hospital of Central South University. Between June 2018 and January 2020, the study enrolled 1,056 patients who were diagnosed with rosacea at the dermatology outpatient department and 1,202 healthy controls who underwent physical examinations in the same hospital. The diagnosis of rosacea was based on the National Rosacea Society Expert Committee (NRSEC) diagnostic criteria (3). Exclusion criteria were: (i) previously diagnosed rosacea that was relieved after treatment; (ii) patients who had received local facial treatment or medical treatment in the past 3 months; (iii) those having other diseases and presenting with facial erythema or itching, such as seborrheic dermatitis, and facial eczema; (iv) patients with severe physical or mental diseases, such as severe depression and malignant tumours; (v) pregnant and lactating women; (vi) patients who were unable to complete the questionnaire survey under the guidance of professionals; and (vii) those unwilling to participate in the questionnaire survey. In addition to the above, exclusion criteria for controls included those with previously diagnosed rosacea that was not significantly relieved after treatment.
Those who fulfilled the inclusion and exclusion criteria were asked to complete a questionnaire. All participants provided written informed consent upon completing and returning the questionnaire. Excluding cases with incomplete data, a total of 956 rosacea patients and 1,107 control subjects were included in the case-control study. The study complied with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Xiangya Hospital, Central South University.
Data collection
All information on participants was collected using a standardized questionnaire, including information on demographic characteristics and tea drinking behaviour (see Appendix S1). The clinical characteristics of patients with rosacea were also recorded. The questionnaire collected information on participant’s age group (< 25, 25–34, 25–34, and > 44 years), sex, marital status, occupation (physical labour or non-physical labour), and years of education (≤ 12 or > 12 years). Height and weight of all participants were also recorded, and body mass index (BMI) was calculated (kg/m2). According to the Asian BMI criteria (26), we categorized participants into 3 classes: underweight (< 18.5 kg/m2), normal (18.5–23 kg/m2), and overweight (23–25 kg/m2) or obese (≥ 25 kg/m2). The study defined a history of tea drinking as “drinking a cup of tea of no less than 50 ml at least once a week”. The tea drinking behaviour investigated all referred to that of the patients in the 2 years before the onset of symptoms. The tea was divided into 2 types: non-fermented tea (green tea) and fermented tea (black tea, dark tea and white tea). The study recorded the following data: frequency of tea drinking per week (none ≤ 3, 4–6, and 7 days/week), and per day (none ≤ 2, 3, and ≥ 4 times/day), tea per drink (not applicable (NA) < 3, 3–5, and > 5 g), total monthly tea consumption (none < 50, 50–124, 125–249, and ≥ 250 g), drinking temperature (NA, cold tea refers to the tea more than 30 min after steeping; warm tea refers to the tea 10–30 min after steeping; hot tea refers to the tea within 10 min after steeping), and history of tea consumption (none < 2, 2–5, and > 5 years). A tea drinking event was defined as drinking tea prepared by brewing new tea leaves, similar to the use of tea bags in Europe. In addition, because rosacea may contain a variety of possible signs and symptoms, in order to facilitate the diagnosis and treatment of rosacea, in 2017, NRSEC proposed a phenotype-base standard classification of rosacea (3). The main phenotypes include flushing, erythema, telangiectasia, papules and pustules, phymatous changes, angiotelectasis, etc. (3), and phenotype data and diagnosis were performed by dermatologists. Hence, this study also investigated the relationship between tea drinking behaviour and some main phenotypes of rosacea.
Statistical analysis
The distribution of characteristics between rosacea patients and the control group were compared using the χ2 test. Subsequently, the association of tea drinking behaviour and rosacea was further analysed by logistic regression analysis and the crude odds ratio and 95% confidence intervals (95% CI) were calculated. After adjusting for participant’s age, sex, marital status, BMI, occupation, and years of education, the adjusted odds ratio (aOR) and adjusted 95% CI were calculated for comparison. All data were analysed using SPSS 20.0 software (SPSS Software, Chicago, IL, USA). In addition, in order to eliminate possible confounding factors and make the control group and the case group comparable, propensity score analysis (27) was conducted on the covariates of age, sex, BMI, marital status, occupation and years of education, and the case group and the control group were matched using a 1:1 ratio matching method. Propensity score matching refers to screening the control group and the case group through certain statistical methods, so that the selected research objects are comparable in clinical characteristics (potential confounding factors). In this case, the difference in results between the control and case groups can be completely attributed to their exposure factors. A p < 0.05 (2-tailed) was defined as statistically significant.
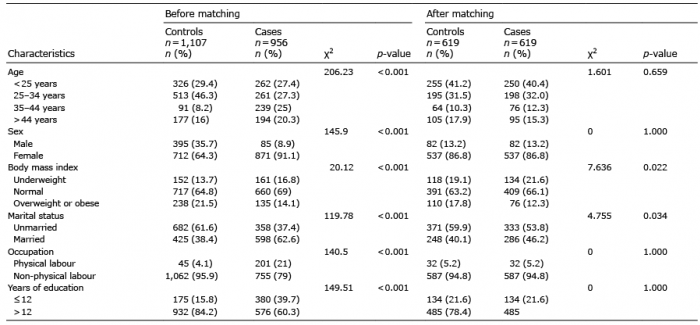
A total of 956 patients with rosacea and 1,107 controls responded to the questionnaire. The demographic characteristics of all participants before and after propensity scores matching are shown in Table I, respectively. As can be seen from Table I, the rosacea and control groups demonstrated statistically significant differences in the distribution of age, sex, marital status, years of education, BMI, and occupation (p < 0.05) before propensity scores matching. In order to reduce the confounding effect derived from the differences in demographic characteristics between the case and the control group, a propensity score matching analysis was conducted (Table I). After matching, 619 cases and 619 controls were included in the current study. There were no significant differences in age, sex, occupation, and years of education between the 1:1 matched cases and the control group (p > 0.05). However, compared with matched controls, the patients with rosacea trended to be of normal BMI (p = 0.022) and unmarried (p = 0.034). All of the above factors were therefore used for correction of the data in subsequent analyses of relationships between tea drinking behaviours and rosacea.
Table I. Distribution of demographic characteristics between rosacea and control groups before and after matching
After adjusting for the above confounding factors, the data suggests that tea consumption (aOR 1.631; 95% CI 1.244–2.319) was a risk factor for rosacea. High-frequency tea drinking (3 times/day: aOR 2.592; 95% CI 1.225–5.485; ≥ 4 times/day; aOR 8.86; 95% CI 3.43–22.887), non-fermented tea (aOR 2.172; 95% CI 1.562–3.022), hot tea (aOR 2.793; 95% CI 1.796–1.344), a short history of tea drinking (< 2 years; aOR 1.72; 95% CI 1.18–2.50), and a long history of tea drinking (> 5 years; aOR 1.531; 95% CI 1.077–2.177) were associated with an increased risk of rosacea. In addition, frequency of tea drinking per week (≤ 3 day/week: aOR 1.545; 95% CI 1.090–2.191; 7 days/week: aOR 1.770; 95% CI 1.162–1.265), tea strength per drink (< 3 g: aOR 1.639; 95% CI 1.219–2.203; > 5 g: aOR 1.69; 95% CI 1.448–13.718), and total monthly consumption (< 50 g: aOR 1712; 95% CI 1.208–2.4251; 125–249 g; ≥ 250 g: aOR 2.303; 95% CI 1.049–3.059; aOR 1.21; 95% CI 0.67–2.16) were also related to rosacea (Table II).
Table II. Comparison of tea consumption behaviour between case and control groups
Comparison of tea-related information from healthy controls and patients with rosacea revealed that rosacea was associated with tea consumption. The relationship between the above-mentioned factors and phenotypes of rosacea was examined further, including flushing, erythema, papules and pustules, phymatous changes, and angiotelectasis (Table III). It was found that these tea drinking behaviours were significantly associated with an increased risk of flushing (aOR 1.41; 95% CI 1.07–1.87) and erythema (aOR 1.48; 95% CI 1.10–2.00). Drinking hot tea correlated positively with an increased risk of flushing (aOR 1.69; 95% CI 1.16–2.47) and erythema (aOR 2.76; 95% CI 1.88–4.05). High-frequency tea drinking (3 times/day: aOR 2.13; 95% CI 1.12–4.07; ≥ 4 times/day; aOR 1.77; 95% CI 1.04–3.02) and frequency of tea drinking per week ≤ 3 day/week (aOR 1.59; 95% CI 1.11–2.27) correlated with an increased risk of erythema. A short history of tea drinking was positively associated with an increased risk of flushing (2–5 years: aOR 1.97, 95% CI 1.10–3.51), papules and pustules (aOR 2.08, 95% CI 1.15–3.75), and telangiectasia (aOR 2.30, 95% CI 1.20–4.40). However, as the length of tea drinking history increased, the risk of rosacea gradually decreased. Finally, a long history of tea drinking (> 5 years), and the type of tea drunk, were not significantly associated with any phenotype of rosacea. In addition, total monthly tea consumption 50–124 g (aOR 2.23, 95% CI 1.34, 3.73) was also positively associated with an increased risk of telangiectasia. However, the type of tea drinking has no significant effect on the subtypes of rosacea. None of the tea drinking behaviours evaluated had any effect on the aggravation of phymatous changes.
Table III. Comparison of tea consumption behaviour with rosacea phenotype in the case groups (n = 619)
Rosacea is a chronic inflammatory skin disease that can be irritated by many triggers. Tea is a popular drink in China, and tea drinking is a significant part of people’s daily lives in many areas. This study investigates the relationship between tea drinking behaviour and rosacea, in order to provide recommendations to patients with rosacea on tea drinking behaviour, which could help alleviate their symptoms.
Application of a multivariate model controlled for confounding factors in the patient’s general data, and the propensity score matching method was used to generate 1:1 matched cases and control group, thus reducing the differences between the 2 groups. Compared with the matched control group, non-fermented tea was associated with an increased risk of rosacea, while fermented tea had no effect on rosacea, which is likely to be related to the effects of different compounds in tea. Previous studies have indicated that non-fermented tea contains more polyphenols (mainly catechins) than fermented tea, which are converted into other compounds such as theaflavins and thearubins during the fermentation process (28). There was little difference in caffeine content between the 2 types of tea (28, 29); therefore, we speculate that polyphenols play a dominant role in development of rosacea due to their high content in non-fermented tea and the similarities in caffeine content between teas. As mentioned previously, some studies have shown that polyphenols in tea have antioxidative, immunomodulatory, and anti-inflammatory effects, which may be beneficial for treating rosacea symptoms (17–21); however, the results of the current study suggest the opposite. In addition to their protective effects, polyphenols have also been shown to induce vasodilation (30), which contributes to the pathophysiological process of rosacea. Kim et al. suggested that epigallocatechin gallate (EGCG), a polyphenolic catechin, has endothelial-dependent vasodilator activity (31, 32). The effect of tea on rosacea is therefore complex; although its compounds have anti-inflammatory and antioxidant effects, they can also promote the development of rosacea by stimulating vasodilation. We speculate that, due to the high concentration of polyphenols (especially catechins) in non-fermented tea, their vasodilatory effect may outweigh the anti-inflammatory and antioxidant effects, thereby increasing the risk of rosacea. As for fermented tea, theaflavin 3,3’-gallate has been shown to have higher antioxidant activity than EGCG (29, 33). Thus, the higher theaflavin content of fermented tea in comparison with non-fermented tea may induce a greater antioxidant effect (28), so that the antioxidant and vasodilating effects of fermented tea can reach a state of mutual balance, leading to no effect of fermented tea on rosacea. The mechanism by which the vasodilatory effect of polyphenols overpowers the anti-inflammatory and antioxidative effects needs further clarification. Based on these findings, we suggest that patients with rosacea should choose fermented tea over non-fermented tea.
In the current study, hot tea was positively associated with the risk of rosacea and, particularly, the risk of some phenotypes, including flushing and erythema. Drinking hot beverages has been suggested to induce neurogenic inflammation, leading to vasodilation, oedema, flushing, and inflammation (6, 23), which is consistent with the current results. According to previous studies, we speculate that this may be related to the activation of transient receptor potential channels, which may be one of the pathogenic mechanisms of rosacea. After activation through increased temperature, vanilloid channels (TRPV1–4) increase skin blood flow via neurogenic vasodilatation, leading to symptoms of rosacea, such as flushing and hypersensitive skin (6, 22, 23, 34, 35). Hence, when drinking hot tea, the above receptors may be activated by the temperature of the tea, which promotes the development of rosacea and aggravates the flushing and erythema phenotype. Therefore, we recommend that patients with rosacea should drink tea at lower temperatures and drink hot tea as little as possible.
Meanwhile, we also observed that high frequency of tea drinking (≥ 4 times/day) and a short history of tea drinking were associated with rosacea and particularly with flushing and erythema. Similarly, the frequency of tea drinking per week, tea strength consumed, total monthly consumption too much or too little, and a long history of tea drinking were mainly related to rosacea. Our previous studies have suggested that high frequency of tea intake may relate to rosacea (7), which is consistent with the results presented here. Garcia et al. proved that tea drinking can attenuate sympathetic activation (36) and that interruption of sympathetic nerves can increase skin blood flow (37). Furthermore, acute tea drinking can increase the skin’s response to heat stimulation and thus increase skin blood flow (38). Therefore, we make the following speculations: when the frequency of tea drinking is low (just once or twice a day), although sympathetic nerves may be suppressed and increase skin blood flow, this effect is not sufficient to induce rosacea. However, when the frequency of tea drinking surpasses the frequency of 4 times a day, and particularly when the frequency of drinking hot tea increases, sympathetic nerves may be in a constant state of suppression, which may lead to a continuous increase in skin blood flow that is sufficient for development of rosacea. On the other hand, the effect of the frequency of tea drinking per week, tea strength consumed, total monthly consumption, and the history of tea consumption on rosacea may be related to the role of polyphenols. We speculate that the vasodilatory effects of polyphenols may be transient, while the anti-inflammatory and antioxidant effects are accumulative. Therefore, when the frequency of tea drinking per week is relatively low, the tea intake is too small, or the history of tea drinking is relatively short, the vasodilatory effect of polyphenols plays a major role in promoting rosacea development. However, when the frequency of tea drinking per week, tea strength consumed, or the years of tea drinking gradually increase, the protective anti-inflammatory and antioxidative effects of polyphenols gradually accumulate. Therefore, in those with a certain range of tea drinking behaviours, such as frequency of tea drinking 3–6 days/week, tea consumed 3–5 g, total monthly consumption 50–125 g, or history of tea drinking 2–5 years, the harmful and protective effects of polyphenols may be in equilibrium, so that these compounds have no effect on rosacea. Whereas some studies have shown that, in addition to the antioxidant effect, high-dose EGCG may also have the opposite effect, namely pro-oxidant effect (39, 40). Furthermore, polyphenols have low bioavailability and rapid metabolism (39). Thus, with a long history of tea drinking over many years or high-dose tea intake, the accumulation effect of polyphenols’ antioxidant and anti-inflammatory effects is lower than its vasodilation and pro-oxidation effect, which ultimately promotes the development of rosacea. Therefore, we recommend that patients with rosacea should drink tea moderately, tea strength consumed and the frequency of tea drinking per week should not be too much or too little, and high-frequency tea drinking should be avoided.
The current study preliminarily establishes links between tea drinking behaviour and rosacea, and also has a relatively large sample size. Moreover, the propensity score matching method was used to reduce the difference between the case group and the control group, and some potential confounders were minimized.
This study also has some limitations. The data are from a questionnaire survey, which may have recall bias. According to our previous research, the current survey did not adjust those dietary habits, such as coffee, alcohol, and smoking, and these may interfere with the results. Some other possible confounding factors, such as unknown skincare products, family history, etc., are missing. Because the production and types of tea have certain regional characteristics, the survey is limited to the Chinese population and may not be fully applicable to patients with rosacea in other regions. However, the current results provide a theoretical basis for subsequent studies on tea polyphenols and rosacea.
In conclusion, this study found that tea drinking behaviour is closely related to rosacea, and mainly affects flushing and erythema. The associations were related to the type of tea consumed (non-fermented tea), frequency of tea consumed per day (≥ 3 times/day), drinking temperature (hot tea), strength of tea per drink (< 3 or > 5 g), total monthly consumption (< 50 or ≥ 125 g), and history of tea drinking (< 2 or > 5 years). This study may provide some evidence that altering the tea drinking behaviour of patients with rosacea could potentially improve their symptoms. Hence, it is recommended that patients with rosacea should moderate the frequency of tea drinking per day, particularly hot tea, but can continue their tea drinking habits in the long term. The mechanisms behind the promotion of rosacea by some compounds in tea remain to be elucidated.
We thank all the participants in the study and the investigators who participated in the field survey for their efforts. We thank Editage (www.editage.cn) for English language editing.


 Click to show fullsize
Click to show fullsize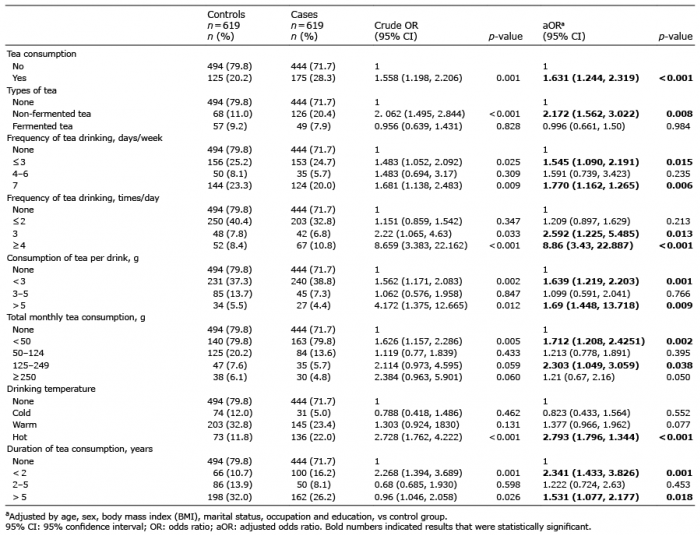 Click to show fullsize
Click to show fullsize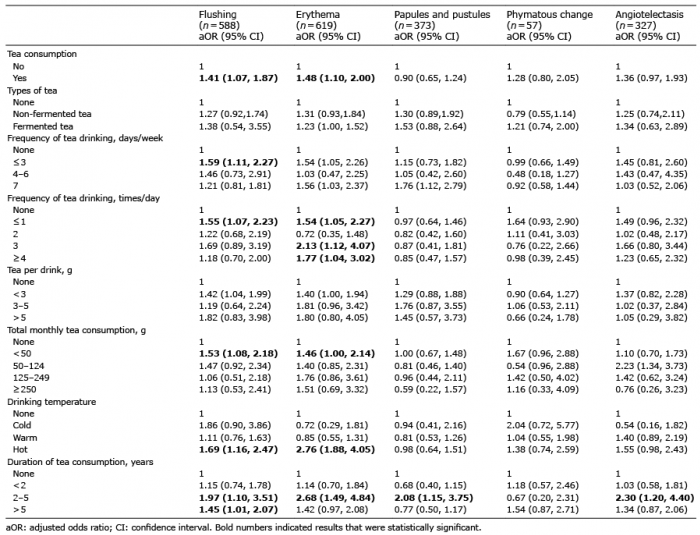 Click to show fullsize
Click to show fullsize