


1Department of Dermatology and 2Department of Pathology, Hôpital Cochin, AP-HP Centre-Université de Paris, FR-75014 Paris, France. *E-mail: nicolas.dupin@aphp.fr
Accepted Jun 21, 2021; Epub ahead of print Jun 23, 2021
Acta Derm Venereol 2021; 101: adv00486.
doi: 10.2340/00015555-3850
Since its appearance in China in December 2019, severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has quickly spread throughout the world, becoming a pandemic. The most common symptoms include fever, cough, shortness of breath and fatigue (1). The incidence of cutaneous lesions ranges from 0.2% in China to 20% in north Italy (2). To date, several cutaneous manifestations have been reported, although demonstration of the infection is often lacking. Among them, maculopapular and vesicular rashes, acral symptoms, such as chilblain-like lesions, urticarial rashes and vascular lesions are the most frequent (2, 3). Isolated cases of atypical cutaneous manifestations have also been reported, including erythema multiforme-like eruption, generalized pruritus, atypical erythema nodosum, atypical Sweet syndrome, Kawasaki disease-like presentation, and polymorphic patterns (4).
We report here a case of Sweet’s syndrome occurring 3 weeks after a confirmed severe coronavirus disease 2019 (COVID-19) infection.
A 51-year-old woman was admitted to the hospital for a febrile dyspnoea. She had a history of idiopathic pulmonary embolism 5 years earlier, treated with 3-months’ anticoagulation. Thorax computed tomography (CT) scan showed bilateral proximal pulmonary embolism and diffuse ground-glass opacities associated with a basal pleural effusion. Rhinopharyngeal SARS-CoV-2 reverse-transcription (RT)-PCR was positive. Oxygen and anticoagulation were introduced, along with a 5-day antibiotic therapy, including ceftriaxone and rovamycine. Dexamethasone was added (6 mg per day for 10 days). Non-invasive ventilation in the prone position was required.
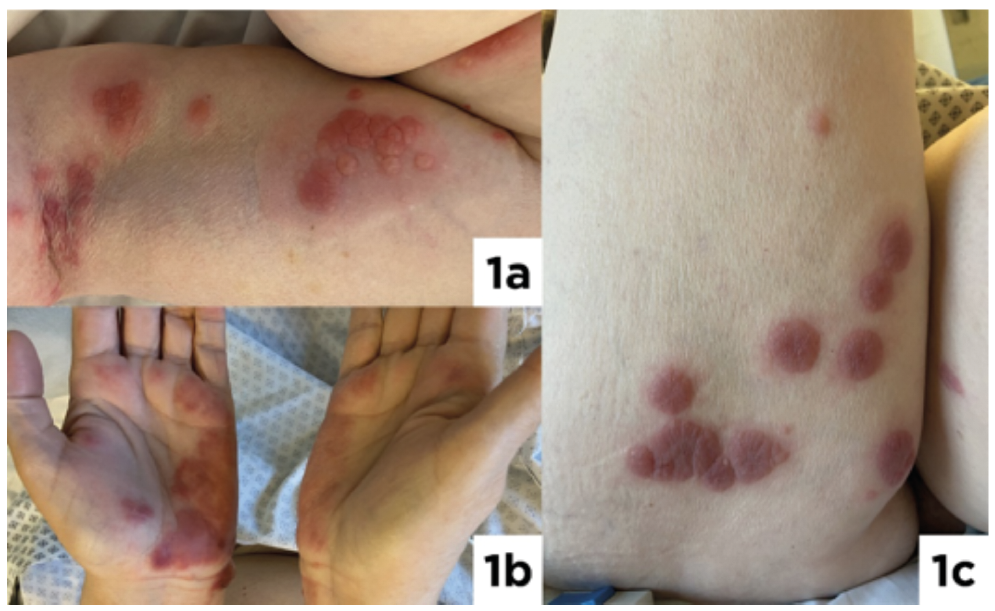
Nine days after stopping corticosteroids, while still oxygen-dependent, the patient developed painful raised dark erythematous oedematous plaques, measuring up to 2 cm. The lesions were distributed asymmetrically on the palms, inner arms, upper trunk and thighs, becoming coalescent bullous plaques (Fig. 1). Clinically, the skin lesions were suggestive of Sweet’s syndrome. No mucosal lesions were found. The patient had no fever, arthralgia or digestive symptoms. Her lymph nodes were not enlarged. Blood count showed normal levels of leucocytes and neutrophils. Laboratory findings showed elevated C-reactive protein level, a mild hepatic cytolysis. SARS-CoV-2 serology (IgG; Abbott, Chicago, USA) was positive for IgG with an index of 7.96. Herpes simplex and varicella zona virus PCR were negative on the lesions. SARS-CoV-2 RT-PCR in skin biopsy was negative (RT-PCR Xpert Xpress Cepheid, Sunnyvale, CA, USA). Histopathological examination showed an intense diffuse neutrophilic infiltrate within the upper dermis associated with a marked papillary dermis oedema, resulting in subepidermal vesiculation. A few eosinophils and lymphocytes were admixed with the neutrophils. Changes in frank leukocytoclastic vasculitis were absent (Fig. 2). Direct immunofluorescence was negative. These histopathological features were in agreement with the diagnosis of Sweet’s syndrome. A positron emission tomography scan, performed to rule out associated malignancies, showed no abnormalities. Protein electrophoresis was normal. The patient did not have any history of inflammatory bowel disease, and faecal calprotectin was negative. No supplementary drugs were added to what was indicated above.
Based on the diagnosis of Sweet’s syndrome, corticosteroid therapy with prednisone, 0.5 mg/kg/day, was introduced. The lesions flattened in 48 h, allowing for a rapid decrease in corticosteroids over a week. The patient received oral corticosteroids for a total of 3 weeks without any relapse.
Fig. 1. Coalescent vesiculo-bullous plaques on (a) the inner left arm, (b) palms and (c) back of the right thigh.
Fig. 2. Histopathological examination of the skin biopsy showing a diffuse neutrophilic infiltrate within the upper dermis associated with a marked papillary dermis oedema. Haematoxylin-erythrosine-saffron (×100).
First described in 1964, acute febrile neutrophilic dermatosis or Sweet’s syndrome is a reactive process characterized by a sudden onset of painful polymorphic lesions most often on the face and upper extremities. Histological examination shows predominantly neutrophilic-dense infiltrates in the upper dermis. The cause of this syndrome remains unknown in most cases. However, it has been associated with inflammatory diseases, haematological or visceral malignancies, pregnancy, drug exposure, and upper respiratory and gastrointestinal infections (5). Ta?k?n et al. (6) reported the first case of atypical Sweet’s syndrome associated with SARS-CoV-2 in a 61-year-old woman presenting several erythematous nodules on the scalp, trunk and extremities, and aphthous ulcers on buccal mucosa, concomitant with typical symptoms of SARS-CoV-2. We describe here a typical Sweet’s syndrome occurring 22 days after COVID-19 infection. Although the patient was still oxygen-dependent at the onset of dermatological symptoms, she no longer had signs of active SARS-CoV-2 infection. The neutrophilic dermatosis was not concomitant with the infection, unlike urticarial and maculo-papular rashes that mainly manifest during SARS-CoV-2 symptoms (3, 4). Associated malignancy and inflammatory bowel disease were ruled out. The possible involvement of the administered drugs was investigated, but no strong evidence was found in terms of extrinsic and intrinsic imputability. We therefore suggest an aetiological role for SARS-CoV-2 in the current patient.
Neutrophilic infiltrates in dermis vessels have been reported previously in a purpuric maculopapular eruption (7) and in erythema multiforme-like eruptions (8). Histopathological examination revealed diffuse neutrophilic infiltration in the upper dermis in a previously published case (6). Severity of COVID-19 infection could be correlated with the neutrophilic response: as described in a lung autopsy of a patient with severe COVID-19 with neutrophil infiltration (9). Although less frequently reported, the occurrence of Sweet’s syndrome associated with COVID-19 could be a clinical marker of severity, unlike chilblains, which are associated with a better prognosis (2, 3).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize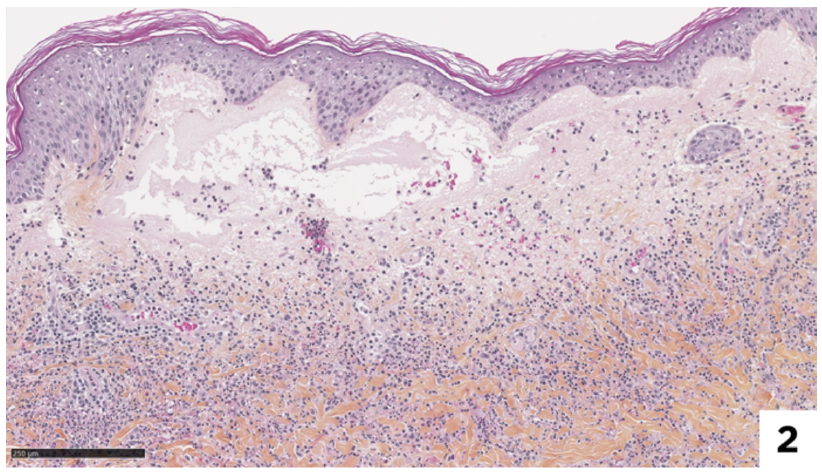 Click to show fullsize
Click to show fullsize