


1Department of Dermatology and Venereology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg and 2Department of Dermatology and Venereology, Region Västra Götaland, Sahlgrenska University Hospital, Gothenburg, Sweden
Research has shown higher rates of incomplete excision among high-risk than low-risk basal cell carcinomas, but data is limited. A single-centre, retrospective study including excised high-risk basal cell carcinomas (type II–III according to the Swedish classification) was performed to determine incomplete excision rates and associated clinicopathological risk factors. Overall, 987 consecutive cases were included. Of these, 203 (20.6%) were incompletely excised. Incomplete excision rates were higher for type III basal cell carcinomas (27.0% vs 17.6% for type II, p < 0.001) and localization on the face and scalp (22.4% vs 14.7% for other locations, p = 0.009), especially on the nose, ear, scalp and periorbital area (28.0–37.0% vs 9.5–16.9% for other locations, p < 0.0001). Circular excisions were also more often incomplete (28.5%) compared with elliptical excisions (17.7%) (p < 0.001). No association was found between incomplete excision rates and tumour size, excision margins, use of a preoperative biopsy or surgeon experience. Mohs micrographic surgery should be used more often for type II–III basal cell carcinomas on the face and scalp.
Key words: basal cell carcinoma; non-melanoma skin cancer; keratinocyte cancer; Mohs micrographic surgery; incomplete excision; risk factors.
Accepted Jun 28, 2021; Epub ahead of print Jun 29, 2021
Acta Derm Venereol 2021; 101: adv00496.
doi: 10.2340/00015555-3856
Corr: Hannah Ceder, Department of Dermatology and Venereology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, SE-413 45 Gothenburg, Sweden. E-mail: hannah.ceder@ vgregion.se
Due to aggressive and destructive local growth, complete surgical removal of high-risk basal cell carcinoma is of utmost importance and should preferably be accomplished at the first attempt. This study found that as much as one-fifth of these tumours were incompletely excised when traditional surgical excision was used. The most important factor associated with incomplete excision was tumour location. Higher incomplete excision rates were seen in the face and scalp, especially on the nose, ear, scalp and periorbital area. Using Mohs micrographic surgery more often in these areas would limit treatment failure.
Basal cell carcinomas (BCCs) can cause signi?cant morbidity due to aggressive and destructive local growth, especially in the head and neck area (1, 2). Internationally, BCCs are classified into 2 categories on the basis of their clinical and histopathological features: low-risk and high-risk subtypes (3). Histopathological growth patterns in low-risk BCCs include nodular and superficial, whereas high-risk BCCs show infiltrative, micronodular, morpheaform or basosquamous features (3–6). In Sweden, however, BCCs are histopathologically categorized according to a classification proposed by Jernbeck et al. (7) in 1988, which includes 4 categories: type IA corresponds to nodular BCC, type IB corresponds to super?cial BCC, type II corresponds to moderately aggressive infiltrative subtypes, and type III corresponds to highly aggressive infiltrative, morpheaform, micronodular or basosquamous subtypes.
For many BCCs, surgery is the recommended treatment (8–10). American, European and Swedish guidelines recommend excision with 3–10-mm clinical resection margins, depending on the clinical and pathological risk factors of the tumour. For high-risk subtypes, safety margins of 5–15 mm or Mohs micrographic surgery (MMS) are recommended depending on individual tumour and patient’s characteristics (3, 6). While MMS essentially guarantees complete removal of the tumour, traditional surgical excision can result in incomplete excisions.
Several studies have compared the incomplete excision rates (IERs) for BCCs of any subtype in different settings, showing IERs ranging from approximately 5% to 24% (11–25). Some of these investigations also identified risk factors for incomplete excision, including: aggressive histopathological subtype; recurrent tumour; and localization on the nose, periorbital area, scalp and ears (12–14, 26). A few studies have observed higher IERs in BCCs with a diameter >20 mm (10, 12, 13) or < 5 mm (14). Conflicting results have been reported regarding surgeon experience (13, 15, 16, 25). A few studies show lower IERs for dermatologists (11, 17, 18) compared with other physician specialties.
Among the risk factors for incomplete excision, the largest impact seems to be associated with an aggressive histopathological subtype. Several studies demonstrate that incomplete excisions of infiltrative or morpheaform BCCs occur in up to 40–50% of cases (11, 12, 15, 19–22). However, most of these investigations included only a limited number of high-risk BCCs, which makes it difficult to draw any conclusions regarding risk factors for this specific group. The aims of this study were to evaluate the IERs for high-risk BCCs and to determine which clinicopathological factors are associated with worse surgical outcomes in these cases.
This retrospective study included all BCCs excised with traditional surgical excision between November 2018 and May 2020 with subsequent histopathological verification as having an aggressive subtype (type II–III according to the Swedish classification) at the Department of Pathology, Sahlgrenska University Hospital, Gothenburg, Sweden. All histopathological slides were examined by pathologists specialized in skin cancer diagnosis. Only BCCs excised with the intention to remove the tumour completely were included. BCCs removed by shave excision, curettage, or partial biopsies were not included. The study was approved by the Regional Ethical Review Board in Gothenburg (approval number 430-16 & amendment approval number 2020-02933).
Electronic patient records and histopathological reports were used to collect the following data: patient age and sex, tumour location, tumour size (maximum diameter on day of surgery) histopathological subtype, preoperative partial biopsy (yes or no), physician specialty, physician experience (resident or specialist), type of excision (elliptical, circular or punch excision) and clinical resection margins (when ambiguous, e.g. 3–4 mm, the smallest margin was recorded). Incomplete excision was de?ned as having a histopathologically veri?ed positive surgical margin. Speci?c information regarding involvement of the lateral, deep or both margins were also registered.
Statistical analyses were conducted using R version 3.5.3 (The R Foundation for Statistical Computing, Vienna, Austria). Fisher’s exact test was used to compare proportions. Wilcoxon’s rank-sum test was used for 2-sample tests and Kruskal–Wallis was used when there were more groups. All tests were 2-sided and p-values < 0.05 were considered statistically significant.
In total, 987 type II–III BCCs were excised during the study period. These tumours were removed from 894 individuals (469 men, 52.5%), median age 75 years (range 31–101 years). The median tumour diameter was 10 mm (range 2–200 mm). The majority of the BCCs were histopathologically veri?ed as type II (n = 672, 68.1%). Among the 315 type III BCCs, 260 were subclassified as highly aggressive infiltrative (82.5%), while the remaining 55 lesions were other subtypes (i.e. morpheaform, micronodular or basosquamous).
The overall IER was 20.6% (n = 203). Among these cases, the lateral margin was affected in 52.7% (n = 107), the deep margin in 31.0% (n = 63) and both margins were positive in 16.3% (n = 33).
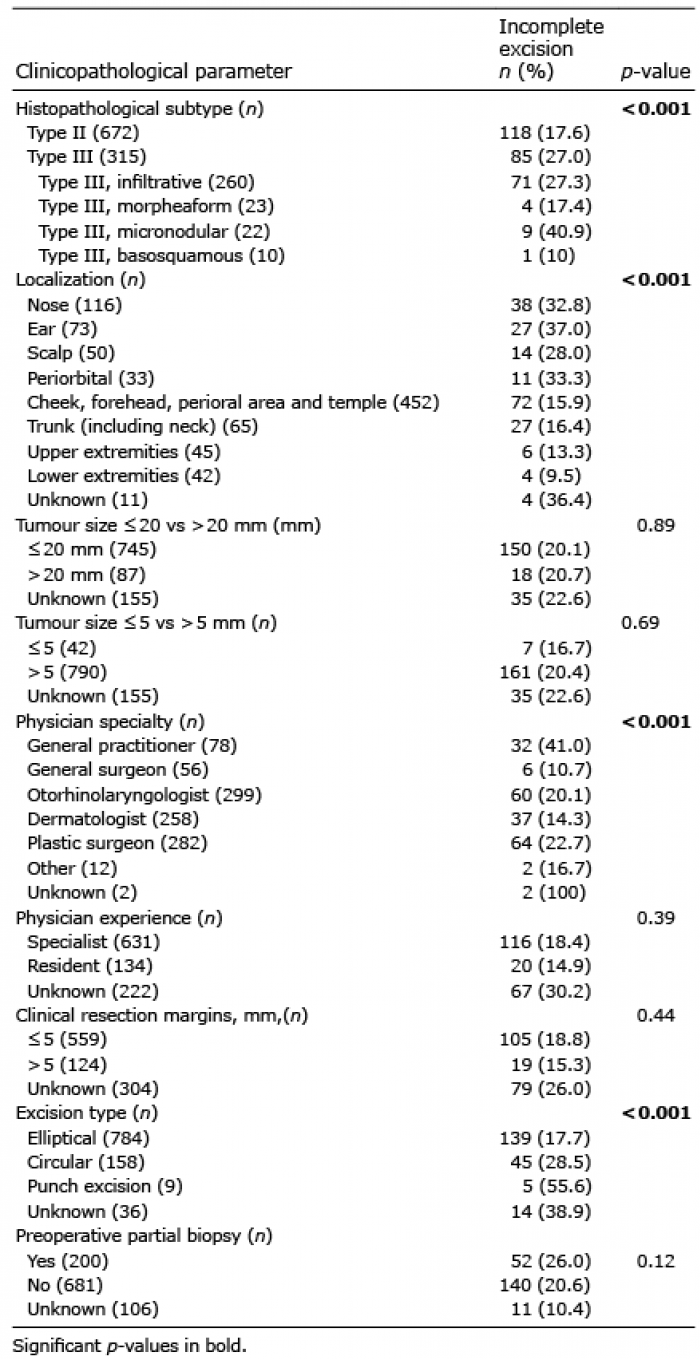
The association between clinicopathological parameters and IERs are listed in Table I. Type III BCCs were incompletely excised significantly more often than type II BCCs (27.0% vs 17.6%, p < 0.001).
Table I. Clinicopathological parameters and their association with incomplete excision rates
BCCs located on the face or scalp (74.2%) were incompletely excised to a greater extent than BCCs on other locations (22.4% vs 14.7%, p = 0.009). The nose, ear, scalp and periorbital area showed the highest IERs, ranging from 28.0% to 37.0%. Lesions on the cheek (n = 28, 17.2%), forehead (n = 17, 12.5%), perioral area (n = 6, 11.8%) and temple (n = 21, 20.6%) were incompletely excised to a lesser degree and are therefore presented as a group.
The median tumour diameter did not differ between incompletely and completely excised tumours (10 mm, range 2–200 vs 10 mm, range 2–60 mm, p = 0.61). Furthermore, the IERs did not differ significantly when comparing tumours ≤ 20 mm in diameter with those > 20 mm (p = 0.89) nor when comparing tumours ≤ 5 vs > 5 mm (p = 0.69).
The clinical resection margins varied greatly (1–30 mm), but the most common choice of margins was 3–5 mm (92.2%). Completely excised BCCs were removed with a larger mean clinical resection margin (3.63 mm, 95% confidence interval (95% CI) 3.48–3.78 mm) than incompletely excised BCCs (3.24 mm, 95% CI 3.07–3.42 mm) (p = 0.0015). However, BCCs excised with a clinical resection margin ≤ 5 mm did not have higher IERs than those with a clinical resection margin > 5 mm (p = 0.44).
Elliptical excisions were most common (82.3%), followed by circular excisions (16.7%) and punch excisions, which were uncommon (< 1%). The use of circular excisions was significantly more frequent on the face and scalp (90.5%) compared with elliptical excisions (71.6%) (p < 0.001). IERs were significantly different between these groups, with elliptical excisions having the lowest rates (p < 0.001).
A preoperative partial biopsy was taken in 200 of 881 BCCs (22.7%) for which data were available. Preoperative partial biopsies did not impact the IERs (p = 0.12). Among biopsied lesions, the preoperative histopathological subtype (II or III) corresponded with the postoperative subtype in 123 lesions (61.5%). In the remaining 77 lesions (38.5%), the histopathological subtype was upgraded in 92.2% of the cases and downgraded in 7.8%.
Overall, general practitioners had the highest IERs (41.0%). Nevertheless, dermatologists, otorhinolaryngologists and plastic surgeons carried out 85.2% of all excisions. When solely analysing excisions by physicians within these 3 specialties, dermatologists had the lowest IERs (p = 0.04). When only examining excisions on the face and scalp, however, no significant differences in IERs were observed between dermatologists (16.5%), otorhinolaryngologists (20.7%) and plastic surgeons (24.8%) (p = 0.12).
Among the 765 cases in which physician experience was known, the majority of BCCs were excised by specialists (82.5%). The IERs of specialists and residents were 18.4% and 14.9%, respectively (p = 0.39).
Fig. 1 shows the proportion of incomplete excisions for type II and type III BCCs according to location. Type III tumours on the nose (n = 40) were especially difficult to excise completely with an IER of 55.0%. It was also the only site with significantly different IERs between the 2 subtypes (p < 0.001).
Fig. 1. Proportions of incomplete excisions for types II and III basal cell carcinomas on different locations. 95% CI: 95% confidence interval.
Associations between histopathological subtypes and other variables are shown in Table II. The sites with the highest and lowest proportions of any type III BCC were the scalp (50.0%) and the periorbital area (12.1%), respectively. Nose, ear and trunk (including neck) showed similar proportions of type III BCC (34.5–38.4%). Furthermore, type III BCCs were generally 1.5 mm larger than type II BCCs (p < 0.0001). Regarding physician specialty, plastic surgeons excised a higher proportion of type III BCCs (44.7%) compared with all other specialties. When analysing physician experience, this was not associated with the histopathological subtype of the excised BCCs. Lastly, the mean clinical resection margins were 0.63 mm wider for type III BCCs compared with type II BCCs (p < 0.001), but the median value for both groups was 3 mm.
Table II. Association between histopathological subtypes and other parameters
Tumours located on the face and scalp were generally smaller than those located on other locations (10 vs 12 mm, p < 0.0001) (Table SI). When only considering BCCs on the face and scalp, the largest mean tumour diameter was observed for BCCs on the scalp (12 mm), while BCCs on the nose had the smallest mean diameter (9 mm). General surgeons and plastic surgeons excised slightly larger tumours (median size 13 and 12 mm, respectively) than physicians with other specialties (9–10 mm) (p < 0.0001). In addition, almost half of the tumours excised by plastic surgeons (n = 148, 43.9%) had a median diameter >10 mm, compared with 25.8% and 16.9% for otorhinolaryngologists and dermatologists, respectively. Tumour diameter did not vary between tumours excised by specialists and by residents (mean diameter 10.0 mm in both groups, p = 0.41). Furthermore, larger tumours were excised with significantly larger clinical resection margins. Only 18.6% of tumours with a diameter ≤ 10 mm were excised with an excision margin > 3 mm, while tumours > 10 mm in diameter were excised with a margin of > 3 mm in 46.7% of cases (p < 0.0001).
Plastic surgeons more often excised tumours on the nose, scalp or periorbital area compared with physicians within other specialties (5.0–23.0% vs 0.8–12.7%) (Table SII). Tumours located on the ear or on the group of other facial areas (cheek, forehead, perioral area or temple) were excised more often by otorhinolaryngologists. Dermatologists more often excised tumours located on other locations (trunk and neck, upper and lower extremities) compared with plastic surgeons and otorhinolaryngologists (30.4% compared with 15.6% and 4.7%, respectively). Moreover, specialists excised a larger proportion of lesions on the face and scalp compared with residents (75.2% vs 64.2% respectively, p = 0.013).
This study found high IERs for high-risk BCCs (type II and III according to the Swedish classification). Overall, higher IERs were associated with type III BCCs, localization, physician specialty as well as excision type. IERs were not significantly associated with tumour diameter, physician experience, clinical resection margins, or whether a preoperative biopsy was obtained.
In other studies that have specified IERs for aggressive subtypes, the rates were 9.5–50.0% (11–17, 19–22, 24, 27, 28). Eight of these studies included < 200 lesions (14, 15, 19–22, 24, 27), 4 included an unknown number of lesions (13, 17, 18, 28), 1 included 275 lesions (11) and the largest study by Kappelin et al. (12) included 773 lesions. In the current study, the IER was 20.6% for all high-risk tumours: 27.3% for type III and 17.6% for type II. Our results for type III BCCs correlate very well with Kappelin et al. (12) where the corresponding number was also 27%. On the other hand, they reported IERs of only 7.5% for type II BCCs. This difference could possibly be explained by the fact that only 58.9% of their type II BCCs were located on the face and scalp (according to personal communication with the authors) compared with 75.0% in the current study.
Incomplete excisions involved the lateral margin (53%) more commonly than the deep one (31%). Similar results have been observed in other studies, including all subtypes of BCC with lateral margins affected in 52–82% of the cases, deep margins affected in 14–36%, and both margins affected in 2–15% (11, 13, 16, 23, 28, 29). Nevertheless, the majority of previous studies examining which margin was affected included all subtypes, without specifying the rates for each subtype.
Of the tumours located on the nose, type III BCCs were excised incompletely to a greater extent than type II BCCs. A similar trend was seen for periorbital BCCs, but the total number of lesions was small (n = 33), making interpretation of significance difficult. For other locations, however, there was no significant difference when taking into account the histopathological subtype. This indicates that MMS, which is especially recommended for type III BCCs, should also be considered for type II BCCS in sensitive areas (30–33).
The current study found that tumours on the face and scalp were more often incompletely excised compared with tumours on the rest of the body (22.4% vs 14.7%). Other studies including all subtypes of BCC also indicate that tumour location affects the IERs (11–14, 20–23, 26, 29). The highest rates were observed on the nose (21–23), ear (12, 26), periorbital area (29) and scalp (13). In several studies including BCCs of all subtypes, IERs varied between 9% and 38% for BCCs on the nose (12, 13, 21–23, 26, 29), while rates of 11–29% were described for BCCs on the ear (12, 13, 21–23, 26).
In the current study, type III BCCs were 1.5 mm larger in median diameter than type II BCCs. However, the actual clinical relevance of such a small difference is questionable. No difference was seen in the IERs if the tumour diameter was ≤ 20 mm or > 20 mm, nor when comparing tumours ≤ 5 vs > 5 mm. Both the Swedish and European guidelines for BCC state that aggressive BCCs >20 mm in diameter require larger clinical resection margins, which is not in line with the results of the current study (10, 34). Only one study has shown that BCCs with a diameter ≤ 5 mm were incompletely excised significantly more often than BCCs with a large diameter (14). Furthermore, there was no difference in median tumour size between incompletely and completely excised tumours. These results are in line with previous studies where the same conclusion was reached (13, 14, 25). Nevertheless, these studies included all histopathological subtypes of BCCs.
There was no significant difference in IERs for BCCs on the face and scalp between otorhinolaryngologists, dermatologists and plastic surgeons. The tumours of general surgeons and general practitioners were localized only on the face and scalp in 2% (n = 2) and 18% (n = 14) of cases, respectively, so it was deemed irrelevant to further analyse IERs for these physician specialties. Consistent results with no significant differences in IERs between different physician specialties have been observed in some studies (25, 35). Although a few studies have shown that dermatologists have lower IERs than other physician specialties (11, 17), the relevance of physician specialty when looking at IERs of aggressive BCC subtypes on the face and scalp is probably limited or non-existent and highly affected by confounding factors.
The IERs were not affected by whether the physician was a specialist or a resident. Regarding the difficulty of their cases, the 2 groups excised type III BCCs to the same extent and their excised tumours had the same mean diameter, while specialists excised a significantly larger proportion of tumours on the face and scalp. Two studies including all subtypes of BCC concluded that the IERs were independent of the physician’s experience (13, 16). One study showed that consultant surgeons had higher IERs, which was most likely due to more complex cases in this group (23). Another study showed higher IERs for junior trainees (15).
Regardless of physician specialty and experience, the current results and other studies generally show that the IERs of aggressive BCCs on the face and scalp with traditional surgical excision is clearly substandard. MMS can therefore be seen as a much more suitable treatment method for aggressive BCCs in sensitive areas, such as the face and scalp.
A preoperative partial biopsy did not affect IERs. These results are consistent with the results of a previous study including all subtypes of BCC (14). Another study with excisions performed by general surgeons, however, showed higher IERs when a preoperative partial biopsy had not been performed (26). The reason that a preoperative partial biopsy did not improve the IERs in the current study could be due to the fact that the subtype reported following the preoperative biopsy did not always correspond to the postoperative histopathological report. Notably, this was the case for 38.5% of the preoperative partial biopsies and in as many as 92.2% of these cases, type II BCCs were upgraded to type III postoperatively. Disparate pathology reports between preoperative and postoperative biopsies have also been shown in other studies in up to 20–40% of cases (36, 37). Thus, a preoperative histopathological report showing a moderately aggressive infiltrative subtype (type II) may be misleading and lead to inappropriate choices regarding the clinical resection margins or not using MMS as the surgical method when it is actually indicated.
Unsurprisingly, circular and punch excisions were associated with higher IERs. The number of punch excisions was very limited, making it difficult to draw any strong conclusions. However, circular excisions were incomplete as often as 28.5% of the time compared with 17.7% for elliptical excisions. To our knowledge, this has not been reported previously, but may be due to the fact that circular excisions were more frequent on the face and scalp. Due to the high IERs when using circular excisions, it may be inappropriate to immediately cover defects following circular excisions of aggressive BCCs with a graft before confirming that the excision is complete, and flap reconstructions should especially be avoided.
To date, this is the largest study on aggressive BCCs (type II–III according to the Swedish classification) evaluating clinicopathological factors associated with IERs. The extensive material with consecutive cases increases statistical certainty and decreases the risk of selection bias. Another strength is that we performed further analyses of possible confounding factors, thus minimizing the risk of inappropriate conclusions. A clear limitation of this study, however, is that it is a retrospective review of electronic patient records and histopathology reports; hence it was not possible to retrieve all clinicopathological data. Another important limitation is the use of the Swedish histopathological classification for BCCs, which is not transferable to the WHO classification system (38). Furthermore, some type III subtypes (i.e. morpheaform, micronodular and basosquamous BCCs) were infrequent, making it difficult to draw conclusions regarding these aggressive subtypes. Also, perineural invasion could not be taken into consideration, since its presence or absence was not always described in the histopathological reports.
In summary, one-fifth of all excised aggressive BCCs were incompletely excised, with the highest IERs found in type III BCCs on the nose. Type II and III BCCs on the ear, nose, scalp and periorbital area should be considered high-risk areas. Tumour diameter, clinical resection margins, the use or not of a preoperative partial biopsy, and physician experience did not affect the rate of incomplete excision. Although these results were inconclusive, it seems unlikely that there is an association between physician specialty and IERs. In our opinion, patients with aggressive type II and III BCCs on the face and scalp should be offered MMS to a greater extent than they are at present in Europe.
The authors thank statistician Martin Gillstedt for his help with the data analysis and Dr. Jan Siarov for his help with data collection.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize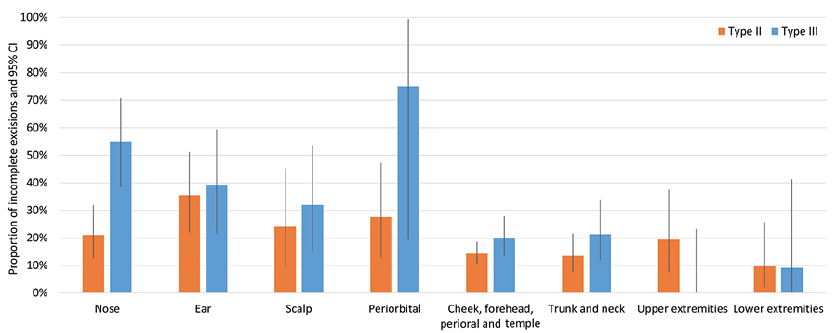 Click to show fullsize
Click to show fullsize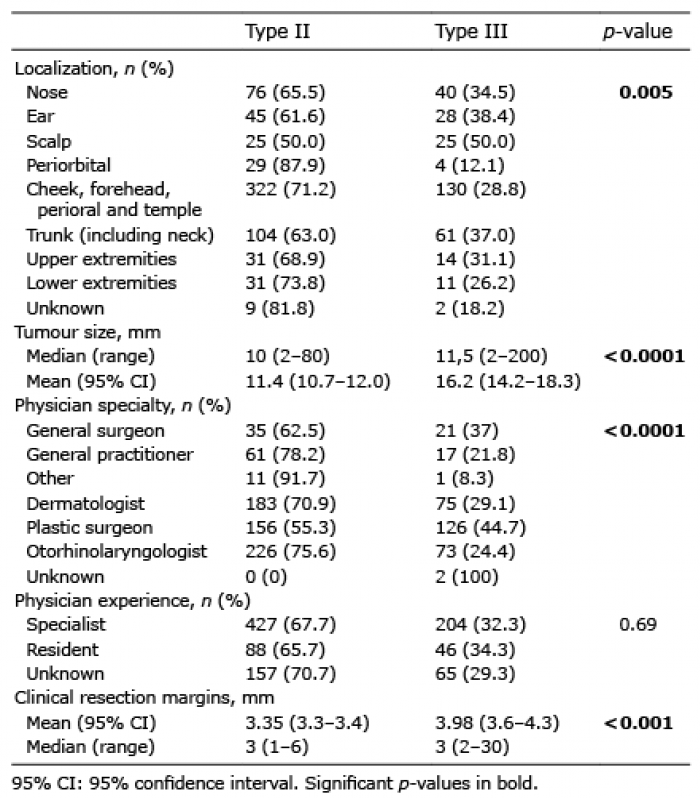 Click to show fullsize
Click to show fullsize