


1Unit of Virus, Lifestyle and Genes, Danish Cancer Society Research Center, 2Department of Dermato-Venereology, Copenhagen University Hospital, Bispebjerg Hospital, Copenhagen, 3Department of Pathology, Copenhagen University Hospital, Hvidovre Hospital, Hvidovre, 4Department of Nephrology, Copenhagen University Hospital, Herlev Hospital, 5Department of Nephrology and 6Department of Gynecology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
Renal transplant recipients have increased risk of human papilloma virus-related anogenital (pre)cancers. Less is known about their risk of anogenital warts. The aim of this study was to estimate the prevalence and odds of anogenital warts in renal transplant recipients compared with immunocompetent controls, and to assess risk factors for intra- and perianal warts in renal transplant recipients. The study examined 248 renal transplant recipients and 250 controls for cutaneous and mucosal anogenital warts. Participants completed a questionnaire on lifestyle and sexual habits. For external anogenital warts (including penile, vulvar and perianal warts), renal transplant recipients had higher prevalence and odds than controls, both in men (8.1% vs 1.6%, adjusted odds ratio (ORadjusted)=5.09, 95% confidence interval (95% CI), 1.03–25.04) and women (11.3% vs 1.6%, ORadjusted=8.09, 95% CI 1.69–38.82). For intra-anal warts, there was no clear pattern of higher odds in renal transplant recipients than controls. Current smoking and having had receptive anal sex increased the risk of intra-/perianal warts in renal transplant recipients. In conclusion, renal transplant recipients in this study had higher odds of external anogenital warts than controls.
Key words: renal transplant recipients; anogenital warts; human papillomavirus; cross-sectional study.
Accepted Jun 28, 2021; Epub ahead of print Jun 29, 2021
Acta Derm Venereol 2021; 101: adv00497.
doi: 10.2340/00015555-3858
Corr: Helle Kiellberg Larsen, Unit of Virus, Lifestyle and Genes, Danish Cancer Society Research Center, Strandboulevarden 49, DK-2100 Copenhagen, Denmark. E-mail: hellekl@dadlnet.dk
Renal transplant recipients are at increased risk of human papilloma virus (HPV)-related anogenital (pre-)malignancies. This clinical cross-sectional study, shows that renal transplant recipients also have increased risk of external human papilloma virus-related anogenital warts, especially vulvar and perianal warts, compared with an immunocompetent control group. These results support that renal transplant recipients should be regularly examined for anogenital warts in a routine setting.
Renal transplant recipients (RTRs) must receive lifelong immunosuppressive therapy to prevent graft failure (1). During recent years, increasing evidence has emerged of an elevated risk of human papillomavirus (HPV)-associated anogenital pre-cancers and cancers in RTRs (2–4). In addition, a high proportion of RTRs develop benign HPV-related cutaneous warts (5). However, less is known about the risk of anogenital warts (AGWs) in this population.
More than 90% of AGWs are caused by the low-risk HPV types 6 and 11 (6). A considerable decline in the incidence of AGWs has been demonstrated in young HPV-vaccinated women in recent years, with a significant herd protection of young male peers (7, 8). In contrast, the incidence of AGWs in unvaccinated older cohorts has remained unchanged (7). Despite being considered benign lesions, a history of AGWs is a strong risk factor for anal pre-cancer lesions among RTRs (9). Likewise, population-based studies have shown that persons with previous AGWs have increased risk of HPV-related anogenital cancers (10, 11). This may partly be caused by co-infection with high-risk HPV types with oncogenic potential (12, 13), due to the shared sexual risk factors for high-risk and low-risk HPV (14), and also by a reduced ability to clear HPV in individuals with AGWs.
Few studies have investigated the risk of AGWs in RTRs. A Danish nationwide, registry-based study showed a more than 3-fold increased rate of AGWs in RTRs compared with the general population (15). The few clinical studies that have investigated the prevalence of AGWs in RTRs were limited by small samples (< 150 RTRs) (16, 17); lack of an immunocompetent control group (17–20); studying RTRs in combination with other organ-transplant recipients (18, 19); and/or a low number of AGWs (16–18, 20).
The aim of this study was to investigate the prevalence and odds of AGWs at different anogenital sites in RTRs compared with an immunocompetent control group. A further aim was to study potential risk factors for intra- and perianal warts in RTRs.
Study population
Recruitment for this cross-sectional study has been described previously (9). Briefly, RTRs were recruited from the Departments of Nephrology at Rigshospitalet, Herlev, Hilleroed, Holbaek and Roskilde Hospitals and from the Department of Dermato- Venereology at Bispebjerg Hospital during 2016 to 2017. The RTRs recruited from the dermatology-venereology department were attending screening for skin cancer, which is offered to all RTRs in Denmark. The controls were likewise consecutively recruited from Bispebjerg Hospital, where they were attending screening for skin cancer or laser treatment for capillary skin disorders. Participants were eligible if they were age ≥ 18 years, HIV-uninfected, had no prior HPV vaccination, no inflammatory bowel disease and no known condition requiring immunosuppressive treatment (except the renal transplantation in RTRs). RTRs were required to be at least 6 months post-transplant and to have a functioning graft. The study was approved by the local Health Research Ethics Committee (H-15014510) and the Capital Region Data Protection Agency (2012-58-0004). The study is registered in ClincialTrials.gov (NCT03018927).
Questionnaire and clinical information
As described previously (9), participants completed a questionnaire regarding sociodemographic characteristics, lifestyle, sexual habits and history of AGWs. Information on immunosuppressive medications of RTRs was collected from medical records, and information on transplantation-related characteristics was obtained from the nationwide Danish Nephrology Registry (21).
Anogenital examination
All participants were examined for clinically visible external (penile, vulvar and perianal) and internal (cervical, vaginal and intra-anal) warts using a Zeiss colposcope OPMI Pico (Carl Zeiss Meditec AG, Germany). Biopsies were obtained from all clinically suspicious lesions to confirm or rule out the AGW diagnosis. In case of multiple similar lesions, only one lesion was biopsied. Only histologically confirmed diagnoses were included in the study.
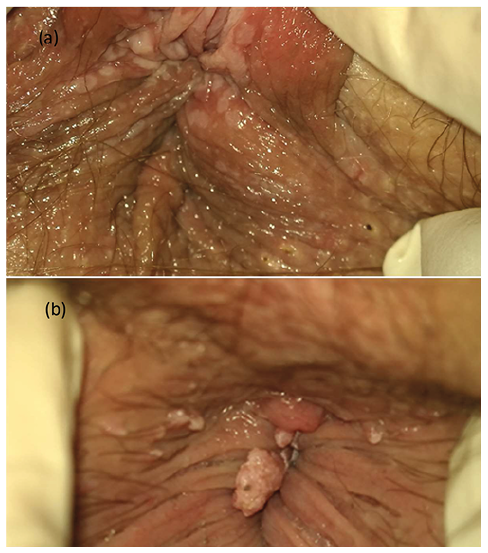
In the anal and perianal area, high-resolution anoscopy (HRA) was additionally performed, with application of 3% acetic acid, as previously described (9). The primary purpose of this was to identify intra-anal and perianal precancerous lesions. Lesions showing aceto-whitening were biopsied, and if the lesions were histologically confirmed as AGWs, they were defined in the present study as “subclinical intra-anal or perianal warts” (Fig. 1).
All clinical examinations, including biopsy-taking, were performed by the same medical doctor (HKL).
Fig. 1. Clinical photographs. (a) Participant with subclinical perianal warts, only visible after application of 3% acetic acid, confirmed histologically. (b) Participant with clinical perianal warts.
Histology
Biopsies were sent in formalin for histo-pathological examination at the Department of Pathology, Hvidovre Hospital. Histological criteria for AGWs were parakeratosis, hypergranulosis, koilocytes or binucleation. All histopathological evaluations were performed by the same experienced pathologist (TTL).
Statistical analysis
The crude prevalence of clinical AGWs in female and male RTRs and controls was calculated separately for each anogenital site (perianal, intra-anal, vulvar, vaginal, cervical and penile clinical warts). Furthermore, the prevalence of “any external clinical AGWs”, including vulvar, penile and perianal clinical warts, and the prevalence of “clinical AGWs at any site”, which included all clinical warts diagnosed in the study, were calculated. Finally, for intra- and perianal sites where acetic acid had been applied, the prevalence of subclinical warts was calculated in an additional analysis.
Logistic regression was used to estimate odds ratios (ORs) with corresponding 95% confidence intervals (95% CIs) for each of the outcomes in RTRs compared with controls. The analyses were conducted separately for men and women. Models were initially adjusted for age (model 1), and subsequently further adjusted for current smoking (yes/no), lifetime number of sexual partners (linear), and history of receptive anal sex (ever/never) (model 2). Adjustment variables were selected a priori, based on existing knowledge of risk factors for AGWs and availability of information in the questionnaire. For the outcome of intra-anal warts, a sensitivity analysis was conducted in which we excluded individuals with a partially visualized transformation zone in the HRA, mainly due to internal haemorrhoids (13 RTRs; 15 controls). Since this did not change our estimates, the participants with partially visualized TZ were included in the results presented below.
Finally, logistic regression was used to investigate risk factors for intra-/perianal warts in RTRs, including both clinical and subclinical intra- and perianal warts. Intra-/perianal warts were selected as the outcome in this analysis, because they constituted the majority of AGWs diagnosed in the study. The analysis was performed for men and women combined, due to low statistical power. Potential risk factors were selected a priori, and adjustments were performed as described above. All statistical analyses were performed using SAS Enterprise Guide version 7.1 (SAS Institute Inc., Cary, NC, USA).
A total of 250 RTRs and 250 controls (125 men and 125 women in each group) were enrolled. In the analysis, 2 participants who had never had vaginal, anal or oral sex, were excluded, leaving 124 female RTRs, 125 female controls, 124 male RTRs, and 125 male controls for analysis.
The median age was higher in female RTRs (55 years; range 32–80) than controls (48 years; range 29–81), whereas the median age was similar in male RTRs (52 years; range, 23–75) and controls (53 years; range 26–89). The proportion of smokers was similar in female RTRs and controls (13% vs 11%), while slightly more male RTRs than controls were smokers (20% vs 14%). RTRs had fewer lifetime sexual partners than controls, both in women (median: 5 vs 10) and men (median: 8 vs 10). More than 40% of female RTRs and controls reported having had receptive anal sex (41% vs 47%), whereas only a few male RTRs and controls had received anal sex (5% vs 3%). Among RTRs, the median age at first transplantation was 44 years; the median time since first transplantation was 8 years; and 88% of RTRs had only had 1 renal transplantation. More than 90% of RTRs were treated with calcineurin inhibitors, anti-proliferative agents and steroids, whereas < 10% were treated with mTOR inhibitors.
Anogenital warts in renal transplant recipients vs controls
Overall, clinical AGWs at any site were diagnosed in 35 (14.1%) RTRs and 21 (8.4%) controls. Among patients with clinical AGWs, 14.0% (5/35) of RTRs and 5% (1/21) of controls had AGWs at more than 1 anogenital site (pFisher’s test = 0.39).
Table I shows the prevalence and ORs of clinical AGWs in RTRs vs controls, overall and separately for each anogenital site. No vaginal or cervical warts were found, and therefore these sites are omitted. RTRs had higher prevalence and odds of clinical perianal warts than controls, both in men (6.5% vs 1.6%, ORModel2 = 4.41, 95% CI 0.82–23.64) and women (7.3% vs. 0.8%, ORModel2 = 7.49, 95% CI 0.89–63.35). For clinical intra-anal warts, there was no clear pattern, as female RTRs tended to have slightly increased odds, whereas male RTRs tended to have slightly reduced odds compared with controls. The prevalence and odds of vulvar warts were higher in female RTRs than controls (5.6% vs 0.8%, ORModel 2 = 9.35, 95% CI 1.06–82.67). The same trend was seen for penile warts, although based on few cases (1.6% vs 0.8%, ORModel 2 = 1.80, 95% CI 0.15–20.58). When considering any external clinical AGWs (vulvar, penile and perianal clinical warts combined), the prevalence and odds were higher in RTRs than controls, both in men (8.1% vs 1.6%, ORModel 2 = 5.09, 95% CI 1.03–25.04) and women (11.3% vs 1.6%, ORModel 2 = 8.09, 95% CI 1.69–38.82).
When looking at subclinical perianal warts, the prevalence was similar in RTRs and controls, both in men (9.7% vs 8.8%) and women (6.5% vs 5.6%). Only a few participants had subclinical intra-anal warts (1.6% of RTRs vs 0.4% of controls) (data not shown).
Table I. Prevalence and odds ratios (ORs) of clinical anogenital warts in renal transplant recipients and immunocompetent controls
Risk factors for intra-/perianal warts in renal transplant recipients
Table II shows risk factors for intra-/perianal warts in RTRs (including both clinical and subclinical intra- and perianal warts). Current smoking (ORModel 1 = 3.10, 95% CI 1.48–6.48) and having had receptive anal sex (ORModel 1 = 2.67, 95% CI 1.21–5.90) were associated with increased odds of intra-/perianal warts when adjusting for age and sex, and these associations were similar in the further adjusted model. Having had ≥ 10 lifetime sexual partners was associated with increased odds of intra-/perianal warts in the age- and sex-adjusted model (ORModel 1 = 2.24, 95% CI 1.00–5.03), but the association was attenuated and became statistically insignificant after further adjustments. Furthermore, in the age- and sex-adjusted model, having a history of AGWs tended to increase the odds of intra-/perianal warts (ORModel 1 = 1.88, 95% CI 0.89–4.01), but the association was considerably attenuated in the further adjusted model (ORModel 2 = 1.04, 95% CI 0.43–2.48). Having been transplanted for ≥ 15 years and having had > 1 transplantation tended to increase the risk of AGWs.
Table II. Risk factors for clinical and subclinical intra-anal and perianal warts in renal transplant recipients (n = 248)
In this clinical study of 248 RTRs and 250 immunocompetent controls, RTRs had higher odds of external clinical AGWs than controls. Current smoking and having had receptive anal sex were identified as risk factors for intra-/perianal warts in RTRs.
The higher prevalence of external clinical AGWs in RTRs compared with controls in the current study is in line with a recent registry-based study from our group, where we showed a higher rate of AGWs in RTRs compared with non-transplanted individuals from the general Danish population (15). Likewise, a small, clinical study by Ogunbiyi et al. (16) showed higher prevalence of external AGWs in RTRs compared with controls. Our findings are also supported by previous studies finding increased rates of HPV-related anogenital pre-cancer lesions (3) and cancers (2, 3) in RTRs compared with the general population. It was also observed that, among individuals with AGWs, RTRs tended to be more likely than controls to have AGWs at more than one anogenital site. Although not statistically significant, this finding further supports that the RTRs were more susceptible to HPV-related lesions.
Interestingly, this study found that the prevalence of perianal clinical warts was higher in male and female RTRs than controls, whereas patterns for intra-anal clinical warts were mixed. In addition, the prevalence of vulvar warts was higher in female RTRs than controls, whereas we found no cervical or vaginal warts in either female RTRs or controls. The reasons for these findings are unclear, but there may be differences in the susceptibility of the epithelium of mucosal sites and cutaneous sites to HPV infection (22, 23). This could potentially influence the different trends observed for perianal and vulvar cutaneous warts and intra-anal and intra-vaginal/cervical mucosal warts. However, there might also be a methodological explanation, as examination for internal warts is more challenging than examination for external warts due to mucosal folds, mucus and, in the anal canal, haemorrhoids and stool. This could have led to some undiagnosed intra-anal warts, and such misclassification could have obscured a potential difference between RTRs and controls in the prevalence of intra-anal warts.
A further finding of the current study was that, although RTRs had higher prevalence of perianal clinical warts than controls, the prevalence of perianal subclinical warts was similar. Detection of subclinical AGWs is a sign of HPV infection, and it can be assumed that all AGW cases begin as subclinical HPV infections. Therefore, a hypothesis could be that RTRs and controls were equally likely to harbour subclinical HPV, but the RTRs were less capable of controlling the infection and thereby more likely to develop clinically visible warts. Immunocompromised patients, both HIV-infected individuals and RTRs, have an impaired host T-cell response, which is believed to reduce their ability to clear or control an established HPV infection (24). However, the failure to detect a difference in prevalence of subclinical warts between RTRs and controls may also be influenced by misclassification, as application of acetic acid to detect subclinical warts is imprecise (6, 25). Therefore, some cases of subclinical warts may have been missed in both RTRs and controls, and such non-differential misclassification could have masked a potential true difference in the prevalence of subclinical AGWs.
The prevalence of external clinical AGWs among RTRs in the current study (men: 8.1%; women: 11.3%) was higher than in most previous studies (0.3%–3.0%) (16, 18, 20). This might partly be due to differences in study design, as some prior studies did not clearly describe the methods for anogenital inspection (17, 18, 20). Nadhan et al. (19) found that the prevalence of AGWs in organ transplant recipients was 1.2% when a “standard genital examination” was conducted (the method was not described), but higher (24.2%) when they introduced a “standardized full genital examination of the mons pubis, bilateral inguinal folds, and external genitalia, with deliberate inspection of the scrotum, penis, vulva, perineum, and perianal area”. Other potential reasons for the different prevalences between studies could be differences in age distribution or sexual behaviour between the study populations.
In the current study, both male and female RTRs had higher prevalence of external clinical AGWs than controls, but the pattern was slightly more pronounced in women. This is in line with the Danish registry-based study by Larsen et al. (15) in which the increased hazard of AGWs compared with non-transplanted individuals was more pronounced in women (age-adjusted hazard ratio 4.94; 95% CI 3.79–6.43) than men (hazard ratio 2.70; 95% CI 2.13–3.43). Likewise, Ogunbiyi et al. (16) found an AGW prevalence of 7.5% in female RTRs compared with no AGWs in male RTRs. In a previous paper based on the same study population as the current study, a similar trend was seen for oral HPV infection, where female, but not male, RTRs tended to have higher oral HPV prevalence than controls (26).
Having had receptive anal sex and current smoking were found to increase the odds of intra-/perianal warts in RTRs in the current study, and a similar trend was seen for high lifetime number of sexual partners. This is in line with previous studies of risk factors for AGWs and HPV infection in immunocompetent persons (27, 28). A review of the impact of smoking on HPV infection and development of AGWs concluded that the incidence and recurrence rate of AGWs are significantly increased in smokers (28). Furthermore, we found that a history of AGWs borderline significantly increased the odds of AGWs among RTRs. It is known that recurrence rates of AGWs after treatment are high, even in immunocompetent individuals (29, 30). Individuals with a diagnosis of AGW may have sexual behaviours that increase the risk of new infections (29) and/or may be less capable of clearing HPV infections, thereby increasing their risk of recurrent AGWs. In the current study, the association between previous AGWs and peri-/intra-anal warts was markedly attenuated when adjusting for smoking, number of sexual partners and receptive anal sex, indicating that these factors explained most of the association.
Strengths and limitations
A major strength of this study was the inclusion of an immunocompetent control group, which, to our knowledge, has only been done by one prior clinical study of RTRs (16). In addition, a large sample of RTRs was recruited from 5 nephrology departments and a dermatology department, and the RTRs enrolled in the current study resembled the overall RTR population in Denmark in terms of age at first transplantation, most common cause of renal failure and treatment regimen (3, 15, 31, 32). Furthermore, in contrast to most studies (18–20), we collected information on not only external clinical warts, but also perianal subclinical warts, and intra-anal subclinical and clinical warts. This provides a more comprehensive estimate of the total HPV-related burden in RTRs. Finally, AGW diagnoses in the current study were histologically verified, and we obtained comprehensive questionnaire data on all participants, including information on sexual behaviour.
However, the current study also has some limitations. First, the control group was a convenience sample from a clinical setting. Therefore, we cannot be entirely sure that the controls are representative of the general population, which may have caused us to underestimate the association between RTR status and AGWs. However, the prevalence of external clinical AGWs in the control group (1.6%) was comparable to the prevalence of AGWs among women aged 30–45 years in a Danish population-based study (33) and was within the range of prevalences reported in a review by Patel et al. (34). Secondly, acetic acid was only applied in the intra-anal and perianal area, although applying acetic acid on the penis, vulva, vagina and cervix might have revealed more HPV-related lesions. The current study used 3% instead of 5% acetic acid as recommended in the guideline of the International Anal Neoplasia Society published after the start of the current study (35); this may have caused us to miss some subclinical AGWs. Thirdly, we did not have statistical power to estimate risk factors for AGWs separately in male and female RTRs, or risk factors for other AGWs than intra-/perianal warts. Finally, although our sample size was larger than most previous studies of AGWs in RTRs (16, 17), we still had few AGWs at the different anogenital sites, which led to wide 95% CIs for some of the estimated ORs.
Conclusion
The current study found a higher prevalence of external clinical AGWs in both male and female RTRs compared with controls. In addition, more RTRs than controls had multi-zonal AGWs, although this finding did not reach statistical significance. Smoking and having had receptive anal sex increased the odds of intra-/perianal warts in RTRs. Taken together with previous findings of a higher risk of HPV-related precancerous lesions and cancers in RTRs (2, 3, 4, 9), these results point to RTRs as a high-risk group for HPV-related diseases. Thus, the current results support that RTRs should be examined for AGWs in a routine setting, and a thorough anogenital examination should include inspection of the vulvar, penile and perianal region. In case of clinically visible vulvar warts, inspection for vaginal or cervical warts should be performed, and correspondingly, anoscopy should be performed in case of clinically visible perianal warts, preferably using magnification of a colposcope. Likewise, attention must be given to lesions suspicious for anogenital high-grade squamous intraepithelial lesions. Data on the effectiveness of HPV vaccination in RTRs is sparse, but vaccination should be considered before the transplantation or at least 1 year post-transplant (36).
The authors thank research nurse Benedikte Maria Skov for patient recruitment, and Dr Lisbet Brandi, Dr Niels Loekkegaard and Dr Michael Munch for patient recruitment from Hilleroed, Holbaek and Roskilde Departments of Nephrology. We thank all the patients who participated in this study.
This work was supported by the Scientific Committee of the Danish Cancer Society (grant number R134-A8560-15-S42, the Aage Bang Foundation (grant number 46-2014/15), the Arvid Nilssons Foundation, the Johannes Clemmensen Foundation (grant number 117844), the Grosserer L. F. Foghts Foundation (grant number 21.053), the Danish Dermatological Society Research Foundation, and the Danish Kidney Association Research Foundation.
SKK has previously received lecture and scientific advisory board fee from Merck and a research grant through her institution from Merck. HKL, MH, LTT, TTL, SSS and JMH have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize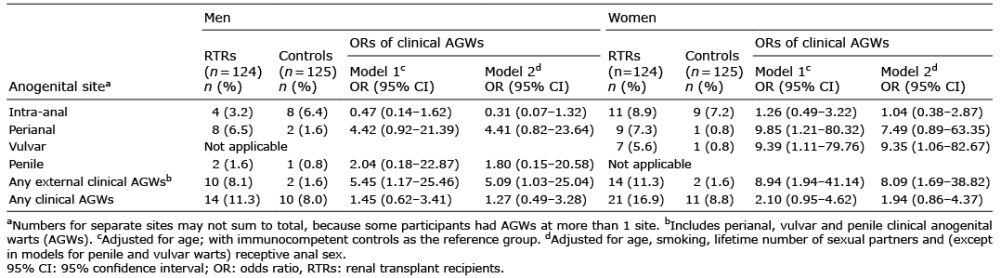 Click to show fullsize
Click to show fullsize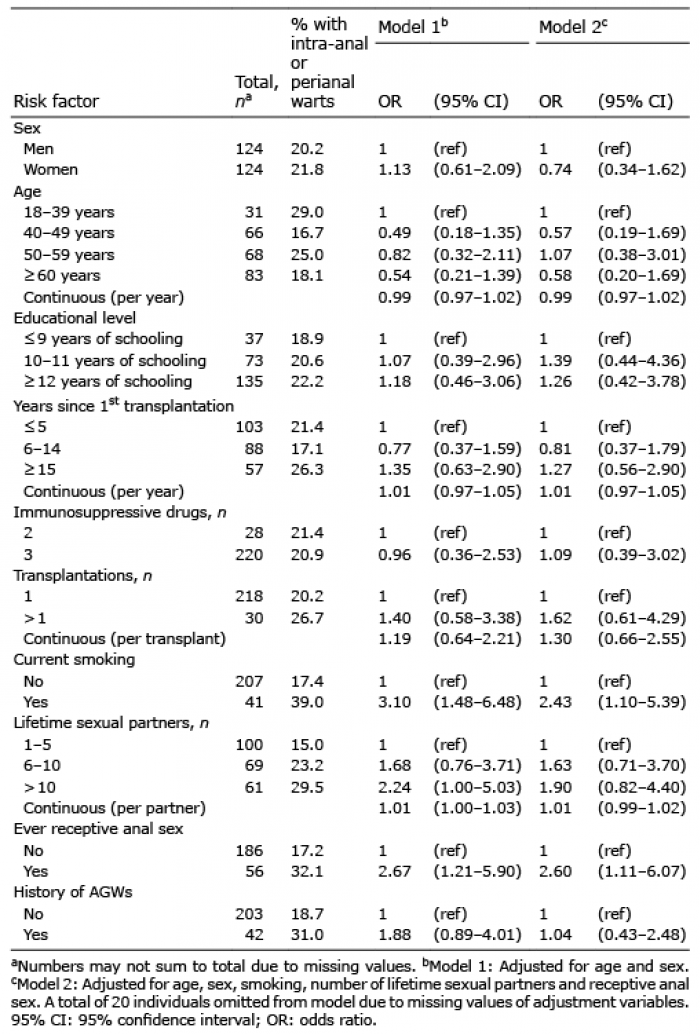 Click to show fullsize
Click to show fullsize