


Department of Dermatology, Royal Perth Hospital, GPO Box X2213, Perth WA 6847, Australia. E-mail: aaron.frederiks@health.wa.gov.au
Accepted Jun 28, 2021; Epub ahead of print Jun 29, 2021
Acta Derm Venereol 2021; 101: adv00493.
doi: 10.2340/00015555-3860
Cladophialophora bantiana is a neurotropic fungus found worldwide, which is known for causing brain abscesses. A review of cerebral infections found a 65.0% mortality rate irrespective of immune status (1). C. bantiana is a dematiaceous fungus, characterized by its cell wall, which contains melanin-like pigments (1). It can infect the skin, presenting clinically as either phaeohyphomycosis, chromoblastomycosis or eumycotic mycetoma (2).
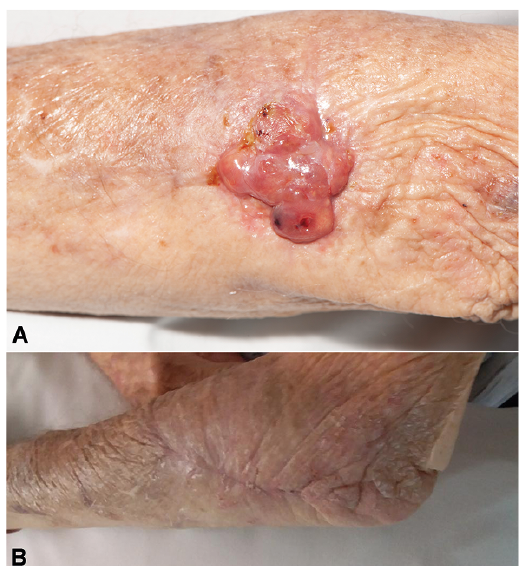
An 87-year-old man presented with a background of recently diagnosed multiple myeloma (MM) and an enlarging cutaneous lesion on his left proximal forearm that had developed in the preceding 4 months (Fig. 1A).
The patient had fallen on a concrete path near a lake in April 2020, grazing both arms. The grazes healed, but a “blood blister”-like lesion developed on his left proximal forearm. His general practitioner initially lanced the lesion, but the lesion continued to enlarge. Examination revealed a solitary, irregular, 3.6×3.8 cm plaque on the left proximal forearm.
Fig. 1. (A) Solitary, irregular 3.6×3.8 cm plaque over the dorsal aspect of the left proximal forearm in an 87-year-old man. The tissue cultured Cladophialophora bantiana (C. bantiana), a neurotropic fungus known for causing brain abscesses in immunocompetent and immunocompromised patients. (B) Complete healing of the left proximal forearm site 1 month after complete excision of the lesion with direct closure.
Two biopsies of the lesion were taken for histopathology in August 2020, which demonstrated dematiaceous fungi (Fig. 2) consistent with phaeohyphomycosis (2). A subsequent biopsy was taken for tissue culture in September 2020. Although fungal elements were not visible on microscopy, after 7 days of incubation at 35°C on Sabouraud plus chloramphenicol agar and brain heart infusion agar plus chloramphenicol, small black colonies had grown in moderate numbers. Identification of C. bantiana strain was confirmed by internal transcribed spacer (ITS) sequencing, which produced a 99.6% match to reference strain CNRMA10.950 (sequence id: KP131824.1) in the GenBank library.
Fig. 2. Haematoxylin and eosin stain (×40 magnification) of a biopsy of the patient’s left proximal forearm demonstrating pigmented (dematiaceous) hyphae and yeast-like structures in an inflammatory background, including multinucleate histiocytes. The biopsy was in keeping with phaeohyphomycosis.
The patient was referred to the infectious diseases department. There was no clinical evidence of extracutaneous or systemic involvement, and a computed tomography (CT) scan of the patient’s head showed no cerebral involvement.
The patient’s MM had been diagnosed in the course of investigating anaemia, just prior to his diagnosis of C. bantiana. A normocytic anaemia and single 6-mm calvarial lesion were his only signs of end-organ involvement. His haemoglobin level was 95 g/l (reference range (rr) 135–180 g/l), platelets 325 × 109/l (rr 150–400 × 109/l), neutrophils 3.12 × 109/l (rr 2.00–7.50 × 109/l) and white cell count 5.37 × 109/l (rr 4.00–11.00 × 109/l). Haematology decided to defer the patient’s treatment with bortezomib, lenalidomide and dexamethasone until after the C. bantiana infection was treated.
The lesion was completely excised with direct closure and the patient commenced on a 3-month course of oral itraconazole, 100 mg daily. One month after surgery, the site had healed completely (Fig. 1B). Four months after surgery there were no signs of recurrence of infection. However, the patient died of an unrelated cause.
A comprehensive literature review was carried out up to November 2020 to identify other cases worldwide of cutaneous infection with C. bantiana. Table SI summarizes the year, country of origin of patient, whether infection was acquired in country of origin, patient age and sex, immune status, description of cutaneous lesion(s), extracutaneous involvement, management and outcome for the 36 total identified cases (including the present case), when information was available.
Table SII provides a summary comparison of the demographics and immune status for cases of cutaneous infection and cerebral infection with C. bantiana. Whilst the highest and second highest proportion of cases of cerebral infections were in India (32.5%) and the USA (24.2%) respectively, with cutaneous infections the highest proportion were in the USA (28%) followed by India (17%).
Cutaneous lesions affected the limbs, torso and head, with heterogeneity in lesion descriptions and development. Table SIII provides a summary of the salient features of cutaneous infections, including prior exposures at the lesion site, pigmentation and extracutaneous involvement.
There are no best-practice guidelines on the management of cutaneous infections with C. bantiana. Table SIV provides a summary of management, including cases managed with surgical and medical therapy, medical management alone, surgical management alone, and no management. The most common drug used was itraconazole, followed by voriconazole and amphotericin B. Posaconazole was used in only 2 (8%) of 24 cases, despite it having an in vitro minimum inhibitory concentration (MIC90) of 0.125 µg/ml, equal most effective with itraconazole, out of 8 antifungals tested against C. bantiana (3). Of the 26 cases with a reported outcome, 4 (15%) were deceased, all 4 of whom had cerebral involvement.
In conclusion, the current patient is the oldest case in the literature in which C. bantiana has been found in the skin, and only the third reported case infecting the skin of an Australian patient. The current case adds further support for complete surgical excision, where possible, in addition to systemic antifungal therapy.
Dermatologists should pay particular attention to non-healing expanding lesions, particularly if there has been prior injury or intervention at the site, contact with plant, tree or soil material, or blackening/pigmentation in the lesion. Tissue culture is needed to confirm the diagnosis. If C. bantiana is found on culture, it is critical to review the patient for extra-cutaneous involvement, particularly central nervous system involvement, given the neurotropism of C. bantiana and high mortality rate associated with such infection.
A multidisciplinary approach is recommended, with urgent review by an infectious diseases physician, to guide anti-fungal therapy and surgical excision, depending on the size and complexity of the lesion. Given the potential for recurrence of infection, the patient should be followed up regularly.
The authors acknowledge the valued contribution of Dr Gordon Harloe, Consultant Anatomical Pathologist, who provided the histopathology photomicrograph demonstrating Cladophialophora bantiana infection. The authors would also like to acknowledge the valued contribution of PathWest Laboratory Medicine, in particular Ammie Higgins, Senior Scientist in Mycology, who performed the tissue culture and identification of C. bantiana and assisted with the description of mycology in the manuscript.
The patient in the current case report consented to the publication of all material, including photographs, within the article.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize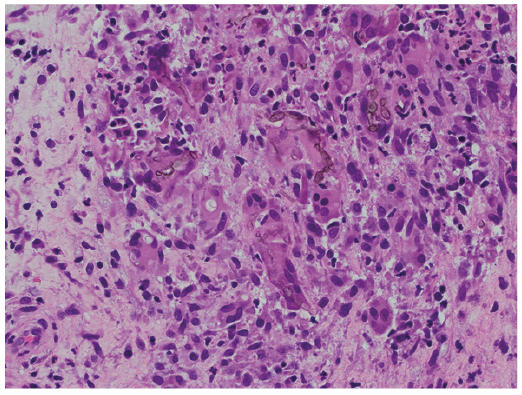 Click to show fullsize
Click to show fullsize